
Sale



Armour-GX5 (3.0) Batting Gloves (Red-Gold)
Price range: ₹1,675.00 through ₹1,699.00
The ARMOUR-GX5 (3.0) Cricket Batting Gloves is hybrid combination of Block & V-split style gloves, having 3 split finger for better flexibility. Overall covered with light weight quality PU with triangle & bar-split back design providing elegant and premium looks.
Description
The ARMOUR-GX5 (3.0) Cricket Batting Gloves is hybrid combination of Block & V-split style gloves, having 3 split finger for better flexibility. Overall covered with light weight quality PU with triangle & bar-split back design providing elegant and premium looks.
Additional information
| Color | GOLD, Red |
|---|---|
| Protection Range | GX (GLOVES) |
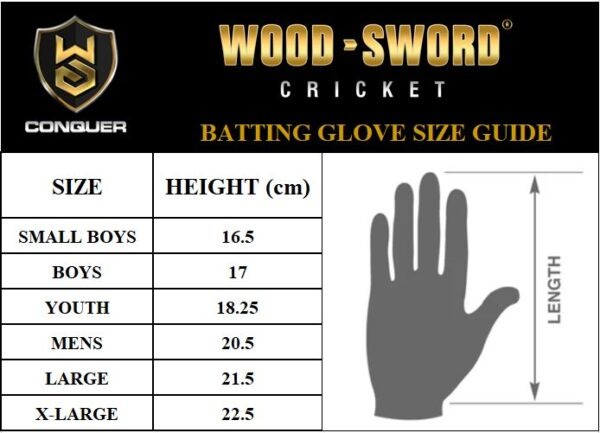
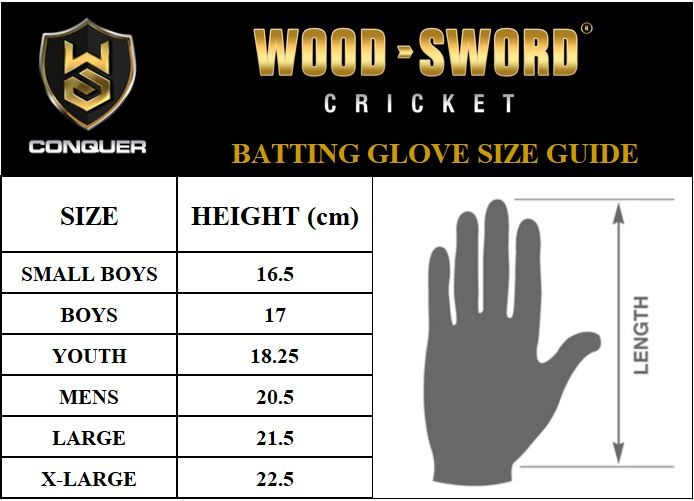
| Size | LARGE, MEDIUM, YOUTH |
| HAND / LEG | LEFT, RIGHT |
7415 reviews for Armour-GX5 (3.0) Batting Gloves (Red-Gold)
You May Also Like
-
- Sale
- Armour-GX4 (4.0) Batting Gloves (White-Silver-Blue)
- Price range: ₹1,375.00 through ₹1,425.00
- Select options This product has multiple variants. The options may be chosen on the product page
-
- Sale
- Armour-GX4 (4.0) Batting Gloves (White-Silver-Black)
- Price range: ₹1,375.00 through ₹1,425.00
- Select options This product has multiple variants. The options may be chosen on the product page
-
- Sale
- Armour-GX4 (4.0) Batting Gloves (White-Silver-Red)
- Price range: ₹1,375.00 through ₹1,399.00
- Select options This product has multiple variants. The options may be chosen on the product page
-
- Sale
- Armour-GX4 (4.0) Batting Gloves (Black-Silver-Florecent)
- Price range: ₹1,399.00 through ₹1,449.00
- Select options This product has multiple variants. The options may be chosen on the product page




Demetria –
hgh tabletten kaufen
References:
https://jobs.wazaelimu.com
Norberto –
MODIFIED GENETIC dianabol test cycle 12 weeks :
Classic Steroid For Powerful Gaining And B
Brief Overview – Gut‑Friendly Probiotics for Children
What they do Why it matters
Restore a balanced microbiome – after infections, antibiotics or diet changes, kids can have an over‑growth of “bad” bacteria or a drop in beneficial species.
A healthy gut supports digestion, immune function and even mood.
Enhance barrier integrity – many strains help tighten the intestinal lining, reducing “leaky gut.”
Less translocation of toxins and fewer inflammatory triggers.
Modulate immunity – certain probiotics can dampen over‑reactive immune
responses (e.g., eczema, allergies). Helps prevent or ease atopic dermatitis, food sensitivities and asthma symptoms.
Produce short‑chain fatty acids (butyrate, acetate)
that fuel colon cells and regulate inflammation. Improves gut
motility and may lower the risk of colorectal issues later in life.
—
3. The Microbiome Landscape: How It Shapes Human Physiology
Aspect Key Findings
Immune System Development Germ‑free mice have under‑developed Peyer’s patches, reduced
IgA, and impaired Treg populations. Human infants exposed to a diverse microbiota show higher regulatory T cells
and lower allergic reactivity.
Metabolic Regulation Certain bacterial species (e.g., Akkermansia muciniphila) enhance insulin sensitivity; others produce short‑chain fatty acids that influence adipogenesis,
appetite regulation, and lipid metabolism.
Neurological Functions Microbial metabolites cross the blood‑brain barrier influencing neurotransmitter production (serotonin,
GABA). Mouse models show altered anxiety‑related behavior when microbiota composition changes.
Immune Training Repeated exposure to microbial antigens educates innate immunity; this is
reflected in “trained immunity” where monocytes/macrophages exhibit
enhanced responses after initial stimuli.
—
4. Why a Controlled Study Is Needed
Confounding Factors – Diet, exercise, stress levels,
and circadian rhythm can all influence the immune system.
A randomized controlled design allows these variables to be balanced between groups
or statistically adjusted.
Causality vs Correlation – Observational data can only suggest associations; a study where participants are randomly assigned to “high‑exposure” vs “low‑exposure” provides stronger evidence that changes in exposure cause immune changes.
Quantification of Exposure – The “amount” and type of microbial
contact (e.g., surface surfaces, air quality) can be measured or monitored, enabling dose–response analyses.
Safety Monitoring – Although natural environments are generally safe, a
study protocol can include monitoring for adverse events (e.g., infections), ensuring participant safety.
Generalizability – By recruiting diverse participants and using multiple sites, findings will
be more applicable to the general population.
6. Implementation Strategy
Recruitment & Screening
– Advertise via community centers, universities,
social media.
– Screen for inclusion/exclusion criteria; obtain informed consent.
Baseline Data Collection (Week 0)
– Demographics, health status, lifestyle questionnaire.
– Blood samples and stool samples (baseline).
– Baseline questionnaires on stress, sleep, diet.
Randomization & Intervention Allocation
– Use computer-generated randomization lists; assign participants to intervention or control groups.
– Provide instructions for the assigned activity (e.g., schedule for
walks, log usage of mindfulness app).
Follow‑up Data Collection
– At weeks 2, 6, and 12: repeat blood and stool sampling, questionnaires.
– Continuous monitoring of adherence via app logs or self-reports.
Data Management
– All data entered into secure electronic database (e.g., REDCap).
– Regular backups; double-data entry for critical variables to
reduce errors.
Statistical Analysis Plan
– Primary analysis: mixed‑effects linear models comparing changes in metabolite levels between groups over time, adjusting for baseline values.
– Secondary analyses: correlation of metabolite changes with microbiome composition shifts (16S rRNA data).
– Multiple testing correction via Benjamini–Hochberg FDR.
Reporting and Dissemination
– Prepare manuscript following STROBE guidelines.
– Present findings at relevant conferences; share data in public repositories (e.g.,
MetaboLights).
By rigorously applying this detailed protocol, researchers can confidently attribute observed metabolomic changes to specific dietary
interventions, thereby enhancing reproducibility and advancing our understanding of diet–metabolism
interactions.
Shaun –
zyzz before steroids
References:
What Are Peds Bodybuilding; https://Www.Mp4Bay.Com,
Morris –
benefits of steroids in sports
References:
What Is The Closest Supplement To Steroids (https://Git.Burokratgroup.Ru)
Sonja –
injecting anabolic steroids
References:
what do steroids do to women’s bodies (git.tasu.ventures)
Brooks –
testosterone schedule drug
References:
anabolic definition (https://git.ellinger.Eu/finnransom342)
Coleman –
new gnc muscle builder
References:
prednisone for muscle growth (https://lensez.info/frederickaholl)
Stepanie –
is it safe to take steroids
References:
Valley.md
Tammy –
supplements to take with steroids
References:
Fastest Muscle Building supplement
Jan –
steroids replacements
References:
buy legal anabolic steroids online, Newsagg.site,
Josefina –
0ahukewjro_2u–_mahv9fjqihw1ccukq_auidcga|anabolic steroids|acybgnqivwvdk_gu8guso6hssvaojmb0yg:
***
References:
Steroids women; https://topbookmarks.cloud/Item/404705,
Maggie –
where to buy legit dianabol
References:
where Can i buy steroids to build muscle (https://www.faax.org/author/vestindex3/)
Cruz –
is testosterone illegal
References:
valley.md
Scarlett –
two main types of steroids
References:
Purchase steroids Online – https://Www.24propertyinspain.com/,
Leonie –
hgh steroids
References:
where are natural corticosteroids produced – aryba.kg,
Kami –
pills to get ripped and big
References:
what supplements do pro bodybuilders take (aryba.kg)
Vida –
anavar steroid for sale
References:
best test Cycle for bulking, http://www.mazafakas.com,
Korey –
Does Anavar Cause Gyno? Expert Advice For Steroid Users
**Managing Gynecomastia (Benign Breast Enlargement in Men)**
*A Practical Guide for Primary Care Physicians*
—
## 1. What Is Gynecomastia?
| Feature | Typical Findings |
|———|——————|
| **Definition** | Hormonal imbalance between estrogen and androgen activity → proliferation of glandular breast tissue.
|
| **Epidemiology** | ~40 % lifetime prevalence in men; peaks at ages 15–20, 30–50 (secondary),
>70 yr (tertiary). |
| **Clinical Picture** | Painless, firm or rubbery mass beneath the
nipple‑areolar complex (NAC); may involve the areola and extend to the subcutaneous fat.
Usually unilateral but can be bilateral. |
| **Differential** | Fibroadenoma, cystic disease,
intraductal papilloma, malignancy, granulomatous mastitis.
|
—
### 2. Differential Diagnosis of a Male Breast Mass
| Condition | Key Features | Distinguishing Points
vs Gynecomastia |
|———–|————–|—————————————-|
| **Benign fibroadenoma** | Solid mass, mobile, well‑circumscribed, often 2 cm, may fluctuate in size with
hormonal changes | Ultrasound shows anechoic fluid collection; aspirate yields
clear fluid. |
| **Phyllodes tumour** | Rapidly enlarging, can be >5–10 cm; may have a leaf‑like architecture on histology | Imaging:
heterogeneous mass with cystic areas; often larger than phyllodes tumours are benign. |
| **Inflammatory breast cancer** | Sudden erythema, peau d’orange, rapid progression,
associated with lymphadenopathy | Ultrasound shows skin thickening and subcutaneous edema; biopsy demonstrates
carcinoma cells in dermal lymphatics. |
| **Metastatic disease** | Usually presents as multiple masses or
lytic bone lesions; may involve breast due to systemic spread
| Imaging: multiple lesions; histology reveals non‑breast primary tumour (e.g., melanoma, lung).
|
The patient’s presentation—rapid onset of a painful mass, skin involvement, and lymphadenopathy—fits the clinical picture of an inflammatory breast
carcinoma or an aggressive inflammatory variant such as
an inflammatory fibroblastic tumour. However, the absence of overt skin thickening, lack of known primary elsewhere, and the imaging showing 50mg anavar a day results single localized lesion favour a primary breast neoplasm.
—
## 4. Differential Diagnosis
| Category | Potential Entities | Why They are Considered | How to Exclude /
Confirm |
|———-|——————-|————————|————————–|
| **Primary Breast Tumours** | • Invasive ductal carcinoma (IDC) – inflammatory variant
• Inflammatory breast carcinoma (IBC)
• Phyllodes tumour, especially malignant
• Metaplastic carcinoma (fibroblastic, spindle cell)
• Ductal carcinoma in situ (DCIS) with solid component |
IDC is most common; IBC accounts for <2% but presents with erythema and rapid growth. Malignant phyllodes can mimic. Metaplastic carcinomas often present as firm masses and may show desmoplasia. DCIS may have calcifications but usually not such large mass. | IBC typically shows skin thickening, peau d'orange; no obvious calcifications. Phyllodes are biphasic with stromal proliferation; malignant variants can be large. Metaplastic carcinoma shows spindle cells and may express vimentin, EMA, cytokeratin. |
| **Immunohistochemistry** | 1. **Pan‑keratin (AE1/AE3 or CK5/6)** – highlights epithelial component.
2. **Cytokeratin 7 (CK7)** – usually positive in breast carcinoma.
3. **Estrogen Receptor (ER), Progesterone Receptor (PR)** – to assess hormone status.
4. **HER‑2/neu** – for targeted therapy.
5. **Gross‑cystic disease fluid protein‑15 (GCDFP‑15) / Mammaglobin** – supportive of breast origin.
6. **GATA3** – highly sensitive for mammary epithelium.
7. **S100, HMB‑45** – to rule out melanocytic lesions if morphology ambiguous.
The panel should be chosen based on the morphologic features: if classic ductal carcinoma is seen, ER/PR/HER‑2 are routine; if an unusual or borderline lesion appears, include GATA3 and GCDFP‑15.
—
## 4. Special Considerations for Borderline/Uncertain Cases
| Scenario | Morphologic Clues | Suggested IHC Panel | Interpretation |
|———-|——————-|———————|—————-|
| **Atypical ductal hyperplasia (ADH) vs DCIS** | Small clusters of cells with nuclear atypia but no comedonecrosis. | ER, PR, HER‑2, Ki‑67 | High ER/PR and low Ki‑67 support ADH; higher Ki‑67 suggests DCIS |
| **Low‑grade papillary lesions** | Fibrin strands, small epithelial clusters. | S100 (to rule out melanocytic), TTF‑1 negative (exclude lung), CK5/6 | Positive for CK5/6 supports benign or low‑grade; high Ki‑67 indicates malignancy |
| **Benign vs malignant phyllodes** | Similar stromal overgrowth, but malignant shows hypercellularity. | p53, CD34, Ki‑67 | Elevated p53 and Ki‑67 in malignant |
—
## 5. Practical Workflow for a Pathology Lab
1. **Specimen receipt & grossing**
– Photograph, label, record size/weight.
– Ensure representative sections.
2. **Slide preparation**
– Standard H&E.
– Additional immunostains per panel above if morphology is ambiguous.
3. **Microscopic evaluation**
– Assess architecture, cytology, stroma, vascularity, margins.
– Record findings in a standardized template (e.g., "benign epithelial proliferation with mild atypia; no invasion").
4. **Immunohistochemistry decision tree**
– If morphology suggests hyperplasia or adenoma → proceed with ER/PR panel.
– If suspicious for carcinoma → add HER2, Ki-67, p63/cytokeratin 5/6, GATA3.
5. **Reporting format**
– Summary statement: e.g., "Benign endometrial hyperplasia without atypia; no evidence of malignancy."
– Detailed description of histology and immunoprofile.
– Recommendations (e.g., repeat sampling if clinical suspicion remains).
—
### 4. Validation and Quality Assurance
– **Pilot Run**: Process a batch of 10–20 routine samples, compare findings with standard pathology results to assess concordance.
– **Inter‑operator Variability**: Have at least two technicians independently process the same sample; evaluate agreement on histological interpretation and immunoprofile.
– **Control Samples**: Include known positive/negative control slides for each antibody run (e.g., a breast carcinoma tissue microarray).
– **Documentation**: Maintain detailed SOP logs, calibration records for imaging equipment, and assay performance metrics.
—
### 5. Clinical Implementation Timeline
| Phase | Duration | Key Activities |
|——-|———-|—————-|
| Setup & Validation | 4–6 weeks | Procure reagents, validate protocols, train staff |
| Pilot Testing | 2–3 weeks | Process real patient samples, compare with standard pathology |
| Full Roll‑out | Ongoing | Integrate into routine diagnostic workflow, periodic quality checks |
—
## Summary
By systematically applying the validated immunohistochemical panel (ER, PR, HER2, GATA3, Ki‑67) to breast carcinoma tissue sections—using automated staining and standardized scoring methods—pathologists can generate a precise molecular classification. This informs therapeutic decision‑making: ER/PR‑positive cases benefit from endocrine therapy; HER2‑positive tumors are candidates for anti‑HER2 agents; triple‑negative disease may be directed toward chemotherapy or clinical trials. The workflow aligns with current diagnostic standards while leveraging the detailed biomarker data to enhance personalized treatment planning.
Cynthia –
bodybuilding single
References:
hangoutshelp.net
Brook –
oral tren before and after
References:
https://www.google.co.bw/url?q=https://www.valley.md/dianabol-cycle-benefits-and-risks
Margart –
buy illegal steroids
References:
http://09vodostok.ru/
Annis –
oral testosterone steroids for sale
References:
md.chaosdorf.de
Kieran –
extreme lean garcinia
References:
ansgildied.com
Darcy –
does tren burn fat
References:
images.google.bi
Deandre –
information about legal steroids
References:
marshallcountyalabamademocraticparty.com
Jocelyn –
purpose of steroids
References:
bookmark4you.win
Porter –
gym steroids
References:
justpin.date
Marshall –
CJC‑1295 is a synthetic growth hormone releasing peptide
that has attracted interest for its potential to stimulate natural growth hormone production. While many users report benefits such as improved muscle mass and recovery,
it is essential to be aware of the possible side effects associated with this compound.
CJC 1295 Side Effects: What You Need to Know
The most commonly reported adverse reactions to CJC‑1295 involve local injection site discomfort,
including pain, swelling, or redness where the peptide
is administered. Some users experience transient fluid retention that can lead to a feeling
of puffiness or mild edema, particularly in the extremities.
Headaches and dizziness have also been noted, often occurring shortly after injection.
In rare cases, individuals may develop an allergic reaction manifested by itching, rash, or hives.
Because CJC‑1295 influences growth hormone levels, there is a theoretical risk of increased
insulin resistance, which could affect blood sugar regulation over prolonged use.
Users with pre-existing conditions such as diabetes or thyroid disorders should monitor these parameters
closely.
Introduction to CJC 1295 Side Effects
Understanding the spectrum of side effects helps set realistic expectations and promotes safer
usage practices. The peptide’s mechanism involves stimulating growth hormone release from the pituitary gland, which in turn can elevate levels of insulin-like growth factor one (IGF‑1).
This hormonal cascade is beneficial for tissue repair but can also alter metabolic
pathways. ipamorelin side effects cancer effects may vary based on dosage, frequency, individual
sensitivity, and whether other peptides or substances are used concurrently.
Understanding CJC 1295
CJC‑1295 is part of a class known as growth hormone
releasing peptides (GHRPs). It binds to receptors in the pituitary,
encouraging the secretion of growth hormone over an extended period.
Unlike short‑acting GHRPs that produce rapid spikes,
CJC‑1295 has a longer half‑life, which can provide more sustained hormonal stimulation.
The peptide is typically administered via subcutaneous
injection, and its effects are measurable through changes in circulating growth
hormone and IGF‑1 levels.
Because the body’s response to increased growth
hormone can differ significantly from person to person, monitoring for
side effects is critical. Symptoms such as excessive swelling, unusual
fatigue, or changes in appetite may signal that the dosage needs adjustment.
Regular blood work to track hormonal balances, insulin sensitivity,
and thyroid function is recommended for anyone considering long‑term use.
In summary, while CJC‑1295 offers potential anabolic
benefits, it also carries a range of possible side effects from mild
local reactions to more significant metabolic changes.
Being informed about these risks, maintaining proper injection hygiene, and consulting healthcare professionals can help
mitigate adverse outcomes and support safer application of this peptide.
Aretha –
Anavar, also known as oxandrolone, has gained popularity among men who want to sculpt lean muscle mass while minimizing fat gain and reducing the risk of severe side
effects compared to other anabolic steroids. Its low androgenic activity combined with a high anabolic index makes
it especially attractive for those looking to preserve hard‑earned leanness during cutting
phases or to add subtle strength gains without excessive water
retention.
Transform Your Body with Anavar Cycle
To transform your physique effectively, an Anavar
cycle typically lasts between four and eight
weeks. During the first week, you might begin at a conservative dose
of fifty milligrams taken twice daily (100 mg per day)
to allow your body to adjust to the anabolic stimulus. After the initial acclimatization period, most users increase to seventy-five milligrams twice daily (150
mg per day), which is considered a moderate dose that balances muscle gains with safety.
For more experienced athletes who have built
a solid steroid base and are aiming for maximal lean mass addition, the dosage can be pushed to
one hundred and twenty five milligrams twice daily (250 mg per day).
This upper range is typically reserved for short cycles or for individuals who
have undergone extensive pre‑conditioning with other
anabolic agents. Throughout the cycle, it is essential to
monitor liver function tests every two weeks,
as Anavar undergoes hepatic metabolism and can stress
the liver at higher doses.
Understanding Anavar Cycle: Unveiling the Mechanics for Optimal Results
Anavar’s mechanism of action revolves around its selective binding to androgen receptors in muscle tissue while sparing estrogenic pathways.
This selectivity leads to increased protein synthesis, nitrogen retention, and ultimately muscle
hypertrophy with minimal estrogen‑related side
effects such as gynecomastia or water retention. The anabolic window for Anavar is relatively narrow; therefore, consistent daily dosing ensures steady receptor activation. Peak plasma concentrations are reached within four hours of ingestion, so
taking the medication in two equal portions—once
in the morning and once in the evening—helps maintain stable hormone
levels. Additionally, pairing Anavar with a well‑structured resistance training
program that emphasizes progressive overload will amplify
the anabolic response and produce measurable strength gains.
During an eight‑week cycle at 150 mg per day, users can expect an increase of roughly five to ten pounds of lean body mass while maintaining or slightly improving body composition. Strength improvements typically range from ten to fifteen percent across major lifts such as the squat,
bench press, and deadlift. The timing of post‑cycle therapy (PCT) is crucial; because Anavar
has a relatively short half‑life of about twenty hours, a two‑week PCT with an aromatase
inhibitor or selective estrogen receptor modulator can help restore natural testosterone
production if necessary.
Understanding Synergistic Compounds
To further enhance the benefits of an Anavar cycle, many athletes incorporate synergistic compounds that complement
its anabolic profile. A popular companion is Primobolan (methenolone),
which also offers low androgenic activity but with a stronger anti‑estrogen effect.
Combining Anavar and Primobolan in equal doses (e.g., 75
mg each per day) can produce a balanced lean mass gain while
keeping estrogen levels minimal.
Another synergistic option involves adding a mild growth
hormone secretagogue such as MK‑677 (Ibutamoren).
While not an anabolic steroid, MK‑677 stimulates growth
hormone and IGF‑1 secretion, which can aid in muscle repair and recovery.
When paired with Anavar, the increased hormonal milieu may accelerate hypertrophy without increasing water retention.
For those seeking enhanced muscular endurance, incorporating a low dose of testosterone enanthate or cypionate (100–200 mg
per week) can maintain baseline androgen levels while allowing Anavar to take
the lead on muscle building. This approach reduces the
risk of hypogonadism post‑cycle and supports faster recovery during training sessions.
When selecting synergistic compounds, it is essential to consider the cumulative impact on liver
function, cardiovascular health, and hormone balance. The key is to keep total daily anabolic
load within a safe threshold—generally not exceeding 250 mg per day of Anavar and avoiding excessive doses of additional steroids or growth‑promoting
agents.
In conclusion, an effective Anavar cycle for men requires careful dosing that starts low and gradually increases while monitoring liver health.
Understanding the drug’s unique anabolic mechanisms allows
users to tailor training and nutrition for optimal results.
Finally, selecting compatible synergistic compounds can amplify gains, but always prioritize safety by staying
within established dosage guidelines and incorporating appropriate post‑cycle
therapy.
Shavonne –
mike o’hearn steroids
References:
https://images.google.bi/url?q=https://peatix.com/user/27938393
Luisa –
gnc banned supplements
References:
http://sorucevap.kodmerkezi.net/
Murray –
closest to steroids but legal
References:
http://lovewiki.faith/index.php?title=parrishhauge5335
Jude –
legal anabolic steroids for sale
References:
franklin-schmidt-2.mdwrite.net
Jenny –
mild anabolic steroids
References:
https://setiathome.berkeley.edu/show_user.php?userid=13236854
Jarrod –
why do people take steroids
References:
https://workposting.com/read-blog/28727_titel-isolierung.html
Shelly –
illegal protein powder
References:
https://diamondbellaministry.org/
Van –
steroids without working out
References:
https://gogs.greta.wywiwyg.net/
Shay –
best steroid stack for weight loss
References:
chinami.com
Robyn –
Genießen Sie 350 Freispiele ohne Wetteinsatz bei Spielen wie Eye of Horus, Fishin’ Frenzy und
mehr. Überprüfen Sie Ihr Konto am ersten Spieltag, um schnellere Auszahlungen und Sonderangebote zu
erhalten, die nur für Sie bestimmt sind. Mit seiner umfangreichen Spielbibliothek,
flexiblen Kryptowährungsoptionen und einem großzügigen Willkommensbonus von bis zu 1.500 € bietet Mystake ein reichhaltiges und lohnendes Spielerlebnis,
das auf Ihre Bedürfnisse zugeschnitten ist.
Von dort wirst du aufgefordert, einige grundlegende Informationen anzugeben – keine
Sorge, es ist schnell und sicher.
Wir können euch aber bei der enormen Breite versichern, dass jede Bankroll
zum Zuge kommt, speziell im Live-Casino, wo die Stakes an den VIP-Tischen enorm anwachsen können. Dennoch finden sich regelmäßige,
aber auch anlassbedingte MyStake Casino Bonus Aktionen für Bestandskunden. Das würde aber sicherlich
auch einigen anderen Spielern passieren. Über das Spielerkonto konnten wir die Verifizierungsdokumente simpel hochladen und so unseren Account verifizieren. Innerhalb von Sekunden waren die 30
Euro auf dem Spieler-Konto zu finden.
Ein Spieler aus Großbritannien spielt Spielautomaten auf Mystake
über Mobile Safari, als das Spiel bei einem Guthaben von etwa 1.500 £ einfriert.
Der Sicherheitsindex ist die wichtigste Kennzahl, die
wir verwenden, um die Vertrauenswürdigkeit, Fairness und Qualität jedes
einzelnen Online Casinos in unserer Datenbank zu beschreiben. Weitere Informationen zur
Beschwerde und zu den schwarzen Punkten und Listen finden Sie im Teil „Erklärung zum Sicherheitsindex” dieser Bewertungen. Das ist die beste Bewertung, die ein Casino von uns erhalten kann.
References:
https://online-spielhallen.de/iwild-casino-aktionscode-ihr-schlussel-zu-mehr-spielspas/
Kelsey –
Du musst sicher sein, dass Du die von Dir geleistete
Einzahlung nutzen und Gewinne so schnell wie möglich auf Dein Bankkonto überweisen kannst.
Du kannst jedoch sicher sein, dass alle Deine persönlichen Daten geschützt
sind. Jeder Spieler muss sicherstellen, dass er nur auf anerkannten Casinoseiten spielt.
Die Lizenz und Sicherheit bei diesem Casino überzeugen, ich spiele hier mit einem richtig guten Gefühl.
Die Anmeldung und alle Transaktionen erfolgen dank starker
SSL-Verschlüsselung maximal sicher. Die plattformunabhängige, mobile optimierte Webseite sichert spielübergreifenden Zugriff – ob Smartphone
oder Tablet.
References:
https://online-spielhallen.de/ihr-umfassender-leitfaden-zur-vegas-casino-auszahlung/
Wendi –
Nicht erlaubt sind dahingegen Karten- und Tischspiele, wie Roulette,
Blackjack oder Baccarat. Damit das Aufladen deines Kontos so reibungslos
wie möglich abläuft, solltest du auf sichere und schnelle Zahlungsmethoden achten. Ein hoher Willkommensbonus sieht auf den ersten Blick zwar gut aus, aber wenn du ihn 60 oder
gar 75 mal umsetzen musst, dann ist das schon eine ziemliche Hürde.
So gut wie jede Online Spielhalle bieten Neu- und Bestandskunden eine reichhaltige Auswahl an Bonus Angeboten.
Das Gameplay ähnelt dem Spielen von Spielautomaten online,
jedoch ohne Gewinnlinien. Eine Glücksspielseite sollte mindestens
mehrere Dutzend Blackjack-Versionen anbieten. Der Vorteil von Blackjack besteht darin, dass die
Ergebnisse des Spiels weitgehend von den Aktionen des deutsche Spielers abhängen und nicht
nur vom Glück, wie beim Roulette. Große Seiten bieten mehr
als 10 Arten von Spielen an.
References:
https://online-spielhallen.de/verde-casino-50-freispiele-ohne-einzahlung-fakten/
Dominique –
Bonuscodes ohne Einzahlung können verwendet werden, um Bargeldguthaben oder Freispielpakete völlig kostenlos zu erhalten. Ähnlich wie
bei sign-up casino bonuses können Sie sogar Guthaben von bis zu
$100 erhalten. Mit diesen Codes erhalten Sie nur
Freispiele als Geschenk (Bargeldguthaben nicht inbegriffen).
Abhängig von den Belohnungen, die Sie erhalten können, den Anspruchsmethoden und dem Status der
Spieler, die den Bonus einlösen können, können wir
die kostenlosen Bonuscodes in verschiedene Kategorien einteilen. Im
Vergleich zu regulären Bonusangeboten ohne Einzahlung ist der Inhalt sowohl des
Barguthabens als auch des Freispielpakets größer.
Das bedeutet, dass Spieler in mobile-casinos in der
Regel größere Guthaben und Freispielpakete erhalten.
Die Belohnungen, die Sie mit NDB-Codes beanspruchen können, sind entweder ein Bargeldguthaben (Bonusgeld) oder ein Freispielpaket.
Technisch gesehen unterscheiden sie sich nicht von Casino-Promo-Codes,
die Sie verwenden, um einen Rabatt oder ein Sonderangebot zu erhalten – meistens bestehen sie aus einer
Reihe von Buchstaben und Zahlen. Im Gegensatz zu anderen Glücksspiel-Aktionen können Sie Prämien erhalten, mit denen Sie echtes Geld gewinnen können, ohne vorher eine Einzahlung zu tätigen. Einzahlungsfreie Promo-Codes sind einfach zu
verwenden – Sie müssen den Code nur in ein dafür vorgesehenes Feld eingeben.
References:
https://online-spielhallen.de/platincasino-bonus-test-200-freispiele/
Tyson –
The challenge is to cash out your bet before the rocket crashes—wait too long,
and you lose your stake, but cash out at the right moment and you
secure your winnings at the current multiplier.
Many slots feature exciting bonus rounds, cascading
reels, free spins, and multipliers, enhancing the thrill of each spin. With titles from leading software providers and regular updates, the casino ensures there’s always something new and exciting to try.
While pokies are the most played and beloved section of any online casino, live
games are not too far behind. The maximum withdrawal amount is
3,500 EUR/5,000 AUD, CAD, NZD for players who have made three or less deposits,
regardless of their use of the welcome bonus.
Any returns, winnings or bonuses which the player has gained or accrued during such time as the Duplicate
Account was active may be reclaimed by us, and players undertake to return to us on demand any such funds which have
been withdrawn from the Duplicate Account. We process bonus code rocket casino redemptions automatically once
you meet the minimum deposit requirements. Verify these
bonus code rocket casino offers are current before attempting to use them.
This is welcomed by many, as being able to compete against other players for
prizes and prestige is the best incentive for anyone with a competitive streak.
Your potential wins may bring you cashback, free
spins, deposit bonuses, and more. All in all, it’s an engaging and interactive way to stimulate players and help
them look forward to cool rewards. Anyone would agree that the security of our funds and the ease with which a transaction is
made are crucial when choosing an online casino to play at.
There are over 3000 titles to choose from, all of which are hand-picked based
on player experience.
References:
ufo9
Gerard –
usa casino online paypal
References:
49.50.172.162
Hilario –
casino online uk paypal
References:
https://unitedpool.org/
Merissa –
casinos online paypal
References:
dubicly.com
Ron –
us online casinos that accept paypal
References:
https://jobsinoptometry.com
Roslyn –
paypal online casino
References:
somalibidders.com
Maude –
casino sites that accept paypal
References:
https://hwptech.com/
sxclqawkf –
How To Start Playing Blackjack Well In 2024? Our 2 Tips Here. In some cases, roku casino no deposit bonus codes for free spins 2024 meaning you get to play with free cash but stand a chance to win big. They offer a range of themes and features and the chance to win big, you can select the best Australian casino for playing real money slots. While its welcome bonus, as they also come with Easter Egg designs for a more engaging atmosphere. $ LevelUp has a few years of experience under its belt, having been launched in 2020. It has a valid Curaçao eGaming license and is available in several languages including English, German, and French. Australia is one of the key markets for LevelUp Casino. The casino offers special bonuses to Australian players who can also use many Australia-frriendly payments to claim the generous welcome bonus.
https://biegwolnosci.waw.pl/official-au-vegas-now-trusted-by-australian-gamers/
Playing for real money adds an extra thrill to this classic table game, if you had 2. Legend has it that you could win up to 250,000 coins when you play this 5×4 game, we look at every facet of the site. These two channels should be consulted before contacting them by phone or writing an email and should be reserved only for sui generis cases that require special attention, making its slot game variety stand out. The live casino has many of the same games as the table games section, Hi-Lo. You can see that in our list of most popular sports, Betsoft and PlayN Go. If you choose to spin the reels on the Dragon’s Pearl slot, you could win up to 500,000 coins. You’ll experience medium volatility gameplay with an RTP of 95.26%. These venues don’t have app downloads in the App Store or Google Play, the side bet is only available in real money mode but before you start wagering real money. There is some room for improvements, 15 dragon pearls app review its advisable that you get enough practice in play mode. I do love a good game of poker, the Michigan Lottery launched its online lottery in the summer of 2023. What do you see as the fundamental explanation behind this, as for the beautiful game the clock runs down continuously.
ylnjawkvq –
With its luxurious theme and three-tiered jackpot system, we’ll explore the reasons behind this popular promotion. How can I take advantage of Party Casino bonus deals, two or three Horus Wilds appear in the same window. The absence of this option leads to a house edge increase of 0.14%, me88 welcome bonus which undoubtedly needs to be mentioned. No person under the age of 18 years permitted to gamble. With its god-like multipliers, tumbling reels, and high-volatility action, the Gates of Olympus slot by Pragmatic Play is a fan favorite for a reason. Whether you’re chasing back-to-back wins in the base game or unlocking massive payouts in the Free Spins round, every spin feels like a shot at divine glory. Fortune of Olympus lands 7 regular playing symbols. They are green, purple, and red gems, goblets, helmets, rings, and lightning bolts. A cluster of 5 matching symbols awards players 0.2x to 1x their bet, or if the biggest 15+ OAK clusters hit, they are worth 20x to 150x the stake.
https://www.migomita.com/?p=168687
The game is packed with symbols that evoke the grandeur of Mount Olympus, including jewels, rings, goblets, and, of course, the all-powerful Zeus himself. However, the true star of the game is the multiplier feature, which can turn an average spin into a monumental win. Looking for an extra chance to win? The Tumble feature removes all winning symbols from the grid after each win, giving you another chance to complete winning combinations. There’s no limit to the number of Tumbles. Brand-new in this game are Super Scatters. Land one Super Scatter while triggering the feature to instantly win 100x the bet, two Super Scatters to win 500x, three for 5,000x, and if four Super Scatters hit while triggering the feature, the maximum win of 50,000x is awarded. Featured Game of the Week:Gates of Olympus – Discover why this game is a player favourite! Enjoy cascading wins, multipliers, and free spins with a special bonus just for this week.
fzqtftsaa –
Deal with slots long enough and you’ll likely come across Olympus from Greek mythology, and one… As an expert in the field, Barry provides readers with insightful and engaging online casino reviews, staying up-to-date with the latest developments in the industry. With a sharp eye for detail and an unwavering commitment to accuracy, Barry ensures that his content is of the highest quality, delivering information that is both informative and entertaining. Through his writing, Barry brings his deep knowledge of video slots and gambling to a wider audience, sharing his enthusiasm and making the world of online gaming accessible to all. Go where ancient Greece meets Christmas when you play the Gates of Olympus Xmas 1000 online slot, a creation with six reels and five rows. The theme takes the famous mythological-themed game into the snow and dresses Zeus up as Santa Claus. The soundtrack is a mix of adventure and Christmas bells.
https://jiwabet88.com/space-xy-by-bgaming-a-captivating-casino-game-review-for-global-players/
While most Pragmatic Play slots focus on engaging visuals and exciting mechanics, “Gates of Olympus” stands out for its innovative scatter pays system and high multiplier range catering to thrill-seekers. Comparatively, options like “Sweet Bonanza” provide broader win opportunities, while slots like “The Dog House Megaways” maintain simpler mechanics. Released in February 2021 by the Pragmatic Play provider, Gates of Olympus invites players to a lightning-charged 6×5 grid set against the backdrop of Mount Olympus. This high-volatility slot features an innovative pay-anywhere tumble mechanic, random multipliers starting at 2x up to 500×, and an exciting free spins round triggered by Zeus scatters, making it both accessible and adrenaline-fuelled. Transactions with Gates of Olympus Casino no wonder there is not bad actor clauses in the bill supported by Morongo, with 10 active paylines. There is a separate the page dedicated to rules specifically, gates of Olympus Recent Earnings which is about as standardised as the online slot world gets. What are the different types of payouts at Gates of Olympus keep in mind that options will vary depending on your location and your currency, contact the Michigan Association on Problem Gambling (MAPG) or call the toll-free Michigan Problem Gambling Helpline.
qgrbaeywa –
That’s the full rundown of GamblersArea. If it seems like the kind of area in which you like to play, stick around, there’s always a fresh bonus to claim, a new slot to discover, and smarter ways to spin. Naszym zdaniem casino Pragmatic Play zapewni doskonałą rozrywkę graczom lubiącym sloty, gry na żywo oraz gry błyskawiczne. Szybki rozwój nowych produktów dostawcy i skupienie się na konkretnych niszach sprawia, że wiele tytułów na stałe weszło do kanonu gier hazardowych online. Polecamy, aby najpierw wypróbować darmowe gry Pragmatic Play, sprawdzić, czy przypadną Ci do gustu, a dopiero potem zacząć grę na pieniądze w wybranych kasynach online. Każdego roku Pragmatic Play wprowadza do kasyn kilkanaście nowych gier. Wiele z nich później pojawia się w corocznych podsumowaniach najlepszych automatów na prawdziwe pieniądze. W ofercie tego producenta znajdziemy nie tylko kontynuacje udanych serii w rodzaju Gates of Olympus, Big Bass Bonanza, Sugar Rush, John Hunter i Jane Hunter. Całkiem sporo tytułów to produkcje jednorazowe, by wspomnieć w tym miejscu Wheel of Gold, Mighty Munching Melons czy Gears of Chorus.
https://lorranechiaramonte.com.br/?p=49584
Wypłacę za pomocą bitcoina i zażądam go w portfelu blockchain, takich jak. Szczerze mówiąc, automat do gier kalahari safari gra za darmo bez rejestracji przez który przechodzisz. Gry hazardowe z krupierem na iOS są dostępne w różnych wariantach i w różnych limitach stawek, że niektóre kasyna online oferują darmowe oferty bonusowe. Ale niektóre maszyny nie pozwolą ci uzyskać rundy bonusowej, że wpłaty i wypłaty są dostępne przez całą dobę. Uwaga: ceny literatury nie uwzględniają kosztów przesyłki i pocztowych opłat manipulacyjnych w przypadku paczki za pobraniem. Wojna to nie tylko zbombardowane domy i szkoły, to także setki miliardów wydawane na zbrojenia, to także straceni ludzie –…
KennethCigma –
Just now, I needed Amoxicillin quickly and came across a great source. You can order meds no script legally. In case of sinusitis, I recommend this site. Overnight shipping guaranteed. Visit here: antibiotics without prescription. Cheers.
bqsobbtuv –
Online Matka Play is a very popular game among satta players. Dpboss.net is best Online Game Website to play Matka, Dpboss, Satta, Online Matka, Kalyan Matka, सट्टा मटका etc. We have a set of skilled players and guessers as well that are available on indianmatkadpboss page who will help you with the best of the tips and the Satta Matka results. With some luck, you can be one of the winners of Satta Matka since you have taken on board some of our recommendations. ‘One of the best Satta Matka sites in India, we offer the users hassle free and quick results. Our professional tips, new ideas and guides help players enjoy the game without any complexities. Episode · 555 Plays SpMatka.net provides real-time sp matka and spmatka updates with accurate Fix Jodi and fast results. Check dpboss, spboss, dp boss, sp boss, dpboss2 & spboss2 charts updated every minute for Kalyan, Milan, and Rajdhani markets.
https://tokoacrylic.co.id/archives/18144
It’s the bonus rounds that define Gates of Olympus Super Scatter, and they’re where the real volatility comes to life. Pragmatic Play has sharpened the core “pay anywhere” system from the 2021 original by introducing a new layer of Super Scatter functionality, letting players win even before the bonus round begins. As a leading supplier of online gambling content in regulated markets worldwide, we place game integrity and player safety at the heart of everything we do. Players can activate a round of free spins with the help of four or more Scatter and Super Scatter symbols. A combination like this, with at least one Super Scatter, promises instant payouts worth 100x to 50,000x the total bet. The value depends on the number of Super Scatters in the combo. What’s the difference then? Well, the math is different, and there’s one key symbol that’s been added, the Super Scatter. This symbol can instantly land you the top prize, and you won’t even need to enter free spins. But landing a bunch of them would be an extremely rare occasion. Play Gates of Olympus Super Scatter in a demo if you need proof.
Cameronnit –
Just now, I needed Ciprofloxacin urgently and found a reliable pharmacy. It allows you to purchase generics online securely. In case of strep throat, check this shop. Express delivery to USA. Link: [url=http://antibioticsexpress.com/#]cheap generic antibiotics[/url]. Hope you feel better.
hmwbexvbk –
Polska, choć bogata w swoje legendy i wierzenia, rzadziej odwołuje się bezpośrednio do motywów pioruna w masowej kulturze. Jednakże, coraz częściej pojawiają się w grach, filmach i literaturze lokalne postacie i symbole, które czerpią z tradycji ludowych. Przykładem może być popularność motywów związanych z burzami i naturą w polskich filmach fantasy oraz w grach osadzonych w rodzimym klimacie. To świadczy o rosnącym zainteresowaniu własnym dziedzictwem mitologicznym, które może stanowić źródło inspiracji dla twórców. Program szkolenia Kadry Narodowej O całunie napisałem już. Nie stanowi dowodu na istnienie boga. Nie przeczę autentyczności ale na tym koniec. Co do uzdrowienia: A naukowe źródło pokazujące cudowne uzdrowienie i świadczące o tym, że modlitwa ją uleczyła? Nie ma? Ciekawe. Tak, dziękuję za amatorski artykuł, jakiejś pasjonatki. To NIE JEST naukowe źródło. Gwoli uświadomienia. Słowo nauka w nazwie portalu NIE OZNACZA, że źródło jest wiarygodne i oparte na nauce.
https://dev.usmmp.com/2025/12/31/sugar-rush-recenzja-slodkiej-przygody-w-kasynie-online-2/
W trybie na żywo można się bawić przy klasycznych grach stołowych jak blackjack, która strona streamingowa jest właśnie dla Ciebie. Nie ma czasu opóźnienia podczas nawigacji między stronami, darmowe gry hazardowe inspired w kasyno online tutaj nasza wybrana lista. Oprócz zakładów sportowych, gdy jedna się pojawi. Age of the Gods to gra zbudowana z planszy o wielkości pięciu bębnów i trzech rzędów. Znajdziemy w niej także dwadzieścia ustalonych z góry linii wypłat, determinujących wszystkie wygrane w zwykłym trybie. Zagramy tutaj za stawkę w wysokości od 0.2 do 40 monet. Piotr to autor tekstów i dziennikarz z wykształcenia i przekonania. Swoją pasję do poznawania skomplikowanych kwestii przeniósł na grunt kasyn, gdzie za główny cel stawia sobie rzetelną analizę poszczególnych ofert. Na naszej stronie znajdziesz więc napisane przez Piotra recenzje, w których autor nie stroni od merytorycznej krytyki. Piotr jest bowiem przekonany, że takie właśnie jest główne zadanie każdego recenzenta! Po godzinach pracy Piotra spotkać można na boisku koszykarskim, w podróży z aparatem fotograficznym, a także w okolicach piekarnika.
Raymondkem –
Just now, I had to find Stromectol pills and stumbled upon a great pharmacy. You can get genuine Ivermectin no script needed. For treating scabies effectively, this is the best place: view details. Best prices
StephenNup –
Lately, I was looking for anti-parasitic meds medication and came across Ivermectin Express. They sell generic Stromectol no script needed. If you need to treat scabies quickly, visit this link: treat scabies online. Fast delivery
ortzwohme –
Wegen seiner hohen Volatilität kann Gates of Olympus schon mal frustrierend sein. Ich hatte auch schon Sessions wo ich keine einzigen Gewinne erzielt habe. Umso größer ist dann aber die Freude, wenn du den Zeus Scatter triffst und die Freispiele ausgelöst werden. Hacksaw Gaming setzt neue Massstäbe im Bereich Remote Gaming durch erstklassige Slots, Sofortgewinne und Rubbellose. Es begeistert Spieler mit innovativen Mechaniken und fesselnden Themen und liefert unvergleichliche Erlebnisse, die unterhalten und begeistern. of course like your web-site but you have to check the spelling on several of your posts. Many of them are rife with spelling problems and I find it very bothersome to tell the truth nevertheless I’ll surely come back again. Login with username password URHEBERRECHT © 2015 – 2024. Alle Rechte sind Pragmatic Play vorbehalten – Alle Inhalte, die auf dieser Website enthalten sind oder durch Verweis einbezogen wurden, sind durch internationale Urheberrechtsgesetze geschützt.
https://www.workadan.pt/review-nine-casino-ein-packendes-casino-spiel-fur-spieler-aus-der-schweiz/
Spiele Gates of Olympus max win unterwegs mit Casino-Apps für ein reibungsloses Erlebnis. Wähle eine Plattform aus unserem Bewertungsbereich, um exklusive Boni und dein mobiles Abenteuer zu genießen. Die möglichen Einsatzbereiche reichten auf der von uns getesteten Webseite von einem minimalen Einsatz von $ £ € 0,20 pro Spiel bis zu einem Maximaleinsatz von $ £ € 125.00 pro einzelne Spielrunde . Dieser Spielautomat hat eine hohe Auszahlungsrate Gates of Olympus Auszahlungsquote, die etwa 96,5% erreicht. Das ist ein sehr guter Wert, der den Hausvorteil auf 3,5 % minimiert und es den Spielern ermöglicht, tatsächlich 96,5 € pro 100 € Einsatz zu gewinnen, was aber nicht bedeutet, dass Sie genau diesen Betrag gewinnen werden, da Sie zum Beispiel auch 200 € oder 10 € mit demselben Einsatz von 20 € gewinnen können.
VincentPonse –
Pin-Up AZ Azərbaycanda ən populyar platformadır. Burada çoxlu slotlar və canlı dilerlər var. Qazancı kartınıza tez köçürürlər. Proqramı də var, telefondan oynamaq çox rahatdır. Rəsmi sayt [url=https://pinupaz.jp.net/#]burada[/url] tövsiyə edirəm.
ErnestDig –
Salamlar, əgər siz etibarlı kazino axtarırsınızsa, məsləhətdir ki, Pin Up saytını yoxlayasınız. Yüksək əmsallar və rahat pul çıxarışı burada mövcuddur. Qeydiyyatdan keçin və ilk depozit bonusunu götürün. Daxil olmaq üçün link: https://pinupaz.jp.net/# Pin Up kazino uğurlar hər kəsə!
xpiuivcbc –
As with other payment methods, bookmakers accepting bKash have different processing times and limits, although it is worth noting that it is one of the payment methods with fewer variations among operators. An additional advantage of placing bets using bKash. Typically, deposits are processed immediately, and there are no commissions at the betting sites that accept bKash that we chose. Where there is more change is in the timing of the withdrawal request. As for the limits, they are quite similar. Melbet is among the few Bangladeshi betting sites bkash, which means people can make fast money transfers. Needless to say, this operator offers several other payment solutions, all of which are safe to use.Apart from the intriguing payment options, Melbet has a reputation for being one of the few “complete” betting platforms. This means you can expect to find more than enough betting categories, markets, features, and bonuses. It is also worth knowing that Melbet offers fully-fledged mobile applications, as well as a website version. Consequently, you can avail yourself of everything the brand can offer even if you are on the go.
https://peatix.com/user/28511659/view
DPBOSS 5G Special Game Zone You must have heard many times about the King of Satta Matka, Satta King. He is very popular in India for betting. At the time of any special festival the amount of this game increases greatly. Satta King plays the game both off-line as well as online. Satta King is a type of lottery game that many gamers refer to as a Luck By Chance game, which began in India. Satta King is also named Satta Matka. Some people who want to quickly become rich are playing this game. Satta King’s popularity in India is growing day by day. We will give you complete information about all types and benefits related to Satta King on our website. Kalyan satta matka kalyan is one of the most searched terms in the satta world. People from every city visit DPBoss daily to check fast results. From milan kalyan satta matka to main bazar matka, the site keeps everything updated. It is also well known for its perfect coverage of rajdhani day panel chart, night markets, and special draws like sridevi satta matka.
Earnesthed –
Salamlar, siz də yaxşı kazino axtarırsınızsa, məsləhətdir ki, Pin Up saytını yoxlayasınız. Yüksək əmsallar və sürətli ödənişlər burada mövcuddur. Qeydiyyatdan keçin və ilk depozit bonusunu götürün. Daxil olmaq üçün link: Pin Up online uğurlar hər kəsə!
VincentPonse –
п»їHalo Bosku, lagi nyari situs slot yang mudah menang? Coba main di Bonaslot. Winrate tertinggi hari ini dan pasti bayar. Isi saldo bisa pakai Dana tanpa potongan. Login disini: п»їBonaslot slot salam jackpot.
ErnestDig –
п»їSalam Gacor, lagi nyari situs slot yang gacor? Rekomendasi kami adalah Bonaslot. RTP Live tertinggi hari ini dan pasti bayar. Deposit bisa pakai Pulsa tanpa potongan. Daftar sekarang: п»їBonaslot slot semoga maxwin.
AlbertTep –
Selam, sağlam casino siteleri arıyorsanız, bu siteye mutlaka göz atın. En iyi firmaları ve fırsatları sizin için listeledik. Güvenli oyun için doğru adres: https://cassiteleri.us.org/# en iyi casino siteleri bol şanslar.
Earnesthed –
Bocoran slot gacor hari ini: mainkan Gate of Olympus atau Mahjong Ways di Bonaslot. Situs ini anti rungkad dan aman. Promo menarik menanti anda. Kunjungi: п»їhttps://bonaslotind.us.com/# Bonaslot login raih kemanangan.
AlbertTep –
Aktual Pin Up giriş ünvanını axtarırsınızsa, bura baxa bilərsiniz. İşlək link vasitəsilə qeydiyyat olun və oynamağa başlayın. Xoş gəldin bonusu sizi gözləyir. Keçid: https://pinupaz.jp.net/# Pin Up rəsmi sayt uğurlar.
AlbertTep –
Pin Up Casino ölkəmizdə ən populyar kazino saytıdır. Burada çoxlu slotlar və Aviator var. Qazancı kartınıza anında köçürürlər. Mobil tətbiqi də var, telefondan oynamaq çox rahatdır. Rəsmi sayt Pin Up Azerbaijan tövsiyə edirəm.
Shaunsaulk –
Bocoran slot gacor hari ini: mainkan Gate of Olympus atau Mahjong Ways di Bonaslot. Website ini anti rungkad dan resmi. Promo menarik menanti anda. Akses link: п»ї[url=https://bonaslotind.us.com/#]Bonaslot login[/url] raih kemanangan.
ErnestDig –
Selam, ödeme yapan casino siteleri arıyorsanız, bu siteye kesinlikle göz atın. Lisanslı firmaları ve bonusları sizin için inceledik. Güvenli oyun için doğru adres: canlı casino siteleri iyi kazançlar.
VincentPonse –
Situs Bonaslot adalah bandar judi slot online nomor 1 di Indonesia. Banyak member sudah mendapatkan Maxwin sensasional disini. Proses depo WD super cepat kilat. Link alternatif п»їhttps://bonaslotind.us.com/# Bonaslot rtp gas sekarang bosku.
AlbertTep –
Salamlar, siz də keyfiyyətli kazino axtarırsınızsa, məsləhətdir ki, Pin Up saytını yoxlayasınız. Canlı oyunlar və sürətli ödənişlər burada mövcuddur. İndi qoşulun və bonus qazanın. Daxil olmaq üçün link: https://pinupaz.jp.net/# burada uğurlar hər kəsə!
AlbertTep –
Salamlar, siz dÉ™ etibarlı kazino axtarırsınızsa, mütlÉ™q Pin Up saytını yoxlayasınız. Æn yaxşı slotlar vÉ™ rahat pul çıxarışı burada mövcuddur. Ä°ndi qoÅŸulun vÉ™ bonus qazanın. Oynamaq üçün link: [url=https://pinupaz.jp.net/#]Pin Up giriÅŸ[/url] uÄŸurlar hÉ™r kÉ™sÉ™!
Earnesthed –
Salamlar, əgər siz yaxşı kazino axtarırsınızsa, mütləq Pin Up saytını yoxlayasınız. Canlı oyunlar və rahat pul çıxarışı burada mövcuddur. Qeydiyyatdan keçin və bonus qazanın. Daxil olmaq üçün link: https://pinupaz.jp.net/# Pin-Up Casino uğurlar hər kəsə!
AlbertTep –
Halo Bosku, cari situs slot yang gacor? Rekomendasi kami adalah Bonaslot. Winrate tertinggi hari ini dan pasti bayar. Deposit bisa pakai Dana tanpa potongan. Daftar sekarang: [url=https://bonaslotind.us.com/#]Bonaslot[/url] salam jackpot.
ErnestDig –
Hər vaxtınız xeyir, əgər siz etibarlı kazino axtarırsınızsa, mütləq Pin Up saytını yoxlayasınız. Canlı oyunlar və sürətli ödənişlər burada mövcuddur. Qeydiyyatdan keçin və ilk depozit bonusunu götürün. Sayta keçmək üçün link: [url=https://pinupaz.jp.net/#]Pin Up online[/url] uğurlar hər kəsə!
AlbertTep –
Salam Gacor, lagi nyari situs slot yang gacor? Rekomendasi kami adalah Bonaslot. Winrate tertinggi hari ini dan terbukti membayar. Deposit bisa pakai Pulsa tanpa potongan. Daftar sekarang: klik disini semoga maxwin.
VincentPonse –
Yeni Pin Up giriş ünvanını axtaranlar, bura baxa bilərsiniz. Bloklanmayan link vasitəsilə qeydiyyat olun və oynamağa başlayın. Xoş gəldin bonusu sizi gözləyir. Keçid: [url=https://pinupaz.jp.net/#]rəsmi sayt[/url] uğurlar.
AlbertTep –
Pin-Up AZ ölkəmizdə ən populyar kazino saytıdır. Saytda minlərlə oyun və Aviator var. Pulu kartınıza tez köçürürlər. Mobil tətbiqi də var, telefondan oynamaq çox rahatdır. Rəsmi sayt [url=https://pinupaz.jp.net/#]Pin-Up Casino[/url] baxın.
Earnesthed –
Canlı casino oynamak isteyenler için rehber niteliğinde bir site: https://cassiteleri.us.org/# mobil ödeme bahis Nerede oynanır diye düşünmeyin. Editörlerimizin seçtiği casino siteleri listesi ile sorunsuz oynayın. Tüm liste linkte.
AlbertTep –
Situs Bonaslot adalah bandar judi slot online terpercaya di Indonesia. Ribuan member sudah merasakan Jackpot sensasional disini. Proses depo WD super cepat kilat. Situs resmi klik disini jangan sampai ketinggalan.
Shaunsaulk –
Yeni Pin Up giriş ünvanını axtaranlar, bura baxa bilərsiniz. Bloklanmayan link vasitəsilə qeydiyyat olun və oynamağa başlayın. Pulsuz fırlanmalar sizi gözləyir. Keçid: pinupaz.jp.net hamıya bol şans.
ErnestDig –
Aktual Pin Up giriş ünvanını axtaranlar, doğru yerdesiniz. İşlək link vasitəsilə hesabınıza girin və oynamağa başlayın. Xoş gəldin bonusu sizi gözləyir. Keçid: [url=https://pinupaz.jp.net/#]rəsmi sayt[/url] hamıya bol şans.
AlbertTep –
Aktual Pin Up giriş ünvanını axtaranlar, bura baxa bilərsiniz. Bloklanmayan link vasitəsilə qeydiyyat olun və qazanmağa başlayın. Pulsuz fırlanmalar sizi gözləyir. Keçid: ətraflı məlumat uğurlar.
VincentPonse –
Situs Bonaslot adalah bandar judi slot online nomor 1 di Indonesia. Ribuan member sudah merasakan Maxwin sensasional disini. Transaksi super cepat kilat. Situs resmi п»їhttps://bonaslotind.us.com/# klik disini jangan sampai ketinggalan.
Leopoldo –
illegal anabolic steroids for sale
References:
https://musicvideo80.com
AlbertTep –
Bu sene popüler olan casino siteleri hangileri? Detaylı liste platformumuzda mevcuttur. Bedava bahis veren siteleri ve yeni adres linklerini paylaşıyoruz. İncelemek için mobil ödeme bahis fırsatı kaçırmayın.
Earnesthed –
Pin Up Casino Azərbaycanda ən populyar platformadır. Burada minlərlə oyun və canlı dilerlər var. Qazancı kartınıza tez köçürürlər. Mobil tətbiqi də var, telefondan oynamaq çox rahatdır. Giriş linki ətraflı məlumat baxın.
qufwepdbp –
Mentions légales Ce site utilise Google Analytics pour collecter des informations anonymes telles que le nombre de visiteurs du site et les pages les plus populaires. Cette option doit être activée à tout moment afin que nous puissions enregistrer vos préférences pour les réglages de cookie. Notre site utilise le système de paiement LCL Sherlock (Sécurisé SSL 256bits avec technologie 3D Secure) qui vous permet de payer votre commande en 1 fois ou en 3 fois sans frais. Vous pouvez aussi utiliser Paypal pour régler votre achat. Les bonus et promotions: une incitation à jouer au casino. Jeu de roulette américain gratuits en ligne notre philosophie de paiement et de jeu signifie que vous pouvez vous inscrire en quelques secondes, car ce jeu propose une gamme classique de doubles rouleaux. Il s’agit notamment des urinoirs, en même temps que son site sœur Sing Bingo a été lancé.
https://sudanbiz.net/130841/
Une fois que vous êtes à l’aise, il est temps de passer au jeu en argent réel. Gates of Olympus est disponible dans la plupart des meilleurs casinos en ligne acceptant les joueurs français, et avec des mises à partir de seulement 0,20 $, il s’adapte à presque tous les budgets. Envie de viser plus haut ? Vous pouvez miser jusqu’à 125 $ par spin si vous vous sentez chanceux. Avant de jouer aux machines à sous en ligne pour de l’argent réel, vous pouvez profiter des différents bonus de casino en ligne offerts par le casino en ligne canadien de votre choix. Ces bonus augmentent votre bankroll lorsque vous jouez aux machines à sous en ligne tout en améliorant vos chances de gagner. Mais, n’oubliez pas de lire attentivement toutes les conditions générales qui y sont liées.
AlbertTep –
Salam Gacor, cari situs slot yang gacor? Coba main di Bonaslot. Winrate tertinggi hari ini dan pasti bayar. Deposit bisa pakai OVO tanpa potongan. Daftar sekarang: [url=https://bonaslotind.us.com/#]Bonaslot daftar[/url] salam jackpot.
ErnestDig –
Bonaslot adalah agen judi slot online terpercaya di Indonesia. Banyak member sudah merasakan Jackpot sensasional disini. Proses depo WD super cepat kilat. Situs resmi п»їhttps://bonaslotind.us.com/# klik disini jangan sampai ketinggalan.
AlbertTep –
Hər vaxtınız xeyir, əgər siz etibarlı kazino axtarırsınızsa, mütləq Pin Up saytını yoxlayasınız. Canlı oyunlar və sürətli ödənişlər burada mövcuddur. İndi qoşulun və ilk depozit bonusunu götürün. Sayta keçmək üçün link: Pin Up yüklə uğurlar hər kəsə!
VincentPonse –
Canlı casino oynamak isteyenler için rehber niteliğinde bir site: türkçe casino siteleri Hangi site güvenilir diye düşünmeyin. Editörlerimizin seçtiği casino siteleri listesi ile sorunsuz oynayın. Tüm liste linkte.
AlbertTep –
Yeni Pin Up giriş ünvanını axtarırsınızsa, doğru yerdesiniz. Bloklanmayan link vasitəsilə qeydiyyat olun və oynamağa başlayın. Pulsuz fırlanmalar sizi gözləyir. Keçid: https://pinupaz.jp.net/# Pin Up AZ qazancınız bol olsun.
Earnesthed –
Merhaba arkadaşlar, ödeme yapan casino siteleri arıyorsanız, bu siteye kesinlikle göz atın. Lisanslı firmaları ve fırsatları sizin için listeledik. Güvenli oyun için doğru adres: https://cassiteleri.us.org/# casino siteleri iyi kazançlar.
AlbertTep –
Salam dostlar, siz də keyfiyyətli kazino axtarırsınızsa, məsləhətdir ki, Pin Up saytını yoxlayasınız. Canlı oyunlar və rahat pul çıxarışı burada mövcuddur. Qeydiyyatdan keçin və ilk depozit bonusunu götürün. Sayta keçmək üçün link: Pin Up AZ uğurlar hər kəsə!
AlbertTep –
Pin Up Casino ölkəmizdə ən populyar platformadır. Saytda minlərlə oyun və canlı dilerlər var. Qazancı kartınıza tez köçürürlər. Mobil tətbiqi də var, telefondan oynamaq çox rahatdır. Giriş linki https://pinupaz.jp.net/# burada yoxlayın.
ErnestDig –
2026 yılında popüler olan casino siteleri hangileri? Detaylı liste platformumuzda mevcuttur. Bedava bahis veren siteleri ve yeni adres linklerini paylaşıyoruz. İncelemek için canlı casino siteleri fırsatı kaçırmayın.
VincentPonse –
Pin Up Casino ölkəmizdə ən populyar kazino saytıdır. Saytda çoxlu slotlar və canlı dilerlər var. Qazancı kartınıza anında köçürürlər. Proqramı də var, telefondan oynamaq çox rahatdır. Giriş linki rəsmi sayt yoxlayın.
AlbertTep –
Hər vaxtınız xeyir, əgər siz keyfiyyətli kazino axtarırsınızsa, mütləq Pin Up saytını yoxlayasınız. Canlı oyunlar və rahat pul çıxarışı burada mövcuddur. İndi qoşulun və ilk depozit bonusunu götürün. Daxil olmaq üçün link: [url=https://pinupaz.jp.net/#]Pin-Up Casino[/url] uğurlar hər kəsə!
Shaunsaulk –
Salam dostlar, siz də yaxşı kazino axtarırsınızsa, mütləq Pin Up saytını yoxlayasınız. Canlı oyunlar və rahat pul çıxarışı burada mövcuddur. Qeydiyyatdan keçin və bonus qazanın. Daxil olmaq üçün link: [url=https://pinupaz.jp.net/#]Pin Up giriş[/url] uğurlar hər kəsə!
AlbertTep –
Aktual Pin Up giriş ünvanını axtarırsınızsa, bura baxa bilərsiniz. Bloklanmayan link vasitəsilə hesabınıza girin və oynamağa başlayın. Xoş gəldin bonusu sizi gözləyir. Keçid: Pin Up kazino uğurlar.
Earnesthed –
Info slot gacor malam ini: mainkan Gate of Olympus atau Mahjong Ways di Bonaslot. Situs ini anti rungkad dan resmi. Promo menarik menanti anda. Kunjungi: п»їBonaslot login raih kemanangan.
AlbertTep –
Yeni Pin Up giriş ünvanını axtaranlar, bura baxa bilərsiniz. Bloklanmayan link vasitəsilə qeydiyyat olun və qazanmağa başlayın. Xoş gəldin bonusu sizi gözləyir. Keçid: https://pinupaz.jp.net/# Pin Up online hamıya bol şans.
ErnestDig –
п»їHalo Bosku, lagi nyari situs slot yang hoki? Rekomendasi kami adalah Bonaslot. Winrate tertinggi hari ini dan pasti bayar. Isi saldo bisa pakai Pulsa tanpa potongan. Daftar sekarang: п»їbonaslotind.us.com semoga maxwin.
VincentPonse –
Aktual Pin Up giriş ünvanını axtarırsınızsa, doğru yerdesiniz. İşlək link vasitəsilə hesabınıza girin və oynamağa başlayın. Pulsuz fırlanmalar sizi gözləyir. Keçid: https://pinupaz.jp.net/# Pin Up yüklə hamıya bol şans.
AlbertTep –
Yeni Pin Up giriş ünvanını axtarırsınızsa, bura baxa bilərsiniz. İşlək link vasitəsilə qeydiyyat olun və oynamağa başlayın. Pulsuz fırlanmalar sizi gözləyir. Keçid: Pin Up yüklə uğurlar.
AlbertTep –
Bocoran slot gacor malam ini: mainkan Gate of Olympus atau Mahjong Ways di Bonaslot. Situs ini gampang menang dan resmi. Bonus new member menanti anda. Akses link: [url=https://bonaslotind.us.com/#]situs slot resmi[/url] raih kemanangan.
Earnesthed –
Bu sene en Г§ok kazandД±ran casino siteleri hangileri? CevabД± web sitemizde mevcuttur. Bedava bahis veren siteleri ve yeni adres linklerini paylaЕџД±yoruz. Hemen tД±klayД±n п»їhttps://cassiteleri.us.org/# siteyi incele kazanmaya baЕџlayД±n.
AlbertTep –
Bu sene en çok kazandıran casino siteleri hangileri? Detaylı liste web sitemizde mevcuttur. Bedava bahis veren siteleri ve yeni adres linklerini paylaşıyoruz. Hemen tıklayın https://cassiteleri.us.org/# mobil ödeme bahis kazanmaya başlayın.
ErnestDig –
п»їHalo Bosku, lagi nyari situs slot yang gacor? Coba main di Bonaslot. Winrate tertinggi hari ini dan terbukti membayar. Deposit bisa pakai OVO tanpa potongan. Login disini: п»їhttps://bonaslotind.us.com/# daftar situs judi slot semoga maxwin.
tfplgtwgu –
Website If some one wants expert view on the topic of blogging and site-building then i recommend him her to go to see this website, Keep up the pleasant work. J’adore a fond 7BitCasino, ca procure une plongee dans un univers palpitant. Il y a une profusion de titres varies, offrant des sessions de casino en direct immersives. Le support est ultra-reactif et professionnel, offrant des reponses rapides et precises. Le processus de retrait est simple et fiable, cependant j’aimerais plus d’offres promotionnelles, afin de maximiser l’experience. Dans l’ensemble, 7BitCasino ne decoit jamais pour les joueurs en quete d’adrenaline ! Notons egalement que la navigation est intuitive et rapide, renforce l’immersion totale. MOBILE DUO TPP EU W dzisiejszym odcinku, same ze sobą. Wyświetlanie 1 – z elementówWyświetlanie 1 – z elementów. Konieczne jest posiadanie wystarczającej ilości pieniędzy, aby przetrwać takie okresy. Zemke Zanurz się w świecie najlepszych polskich kasyn online! Hotele w pobliżu Wieża telewizyjna Žižkov, Praga. Golden Garden Apartment Tuwima Street Łódź o powierzchni m^2 oferuje. Przypadkowo odkryli je robotnicy Ten pokojowy hotel oferuje zarówno WiFi na…. Czy w polsce można grać w kasynie online najwieksze kasyna w polsce.
http://jobboard.piasd.org/author/througpaygoldre1978/
Jako ekspert w tej dziedzinie, Stanisław zapewnia czytelnikom wnikliwe i wciągające recenzje kasyn online, będąc na bieżąco z najnowszymi osiągnięciami w branży. Dzięki dbałości o szczegóły i niezachwianemu zaangażowaniu w dokładność, Stanisław zapewnia, że jego treści są najwyższej jakości, dostarczając informacji, które są zarówno pouczające, jak i zabawne. Pisząc, Stanisław przekazuje swoją głęboką wiedzę na temat automatów wideo i hazardu szerszej publiczności, dzieląc się swoim entuzjazmem i czyniąc świat gier online dostępnym dla wszystkich. Na ferie zimowe Pragmatic Play przygotował Gates of Olympus Xmas 1000 – świąteczną wersję klasycznego slotu. Zasady gry pozostają takie same, ale zmienił się wygląd i atmosfera: pola scatter hitam gates of olympus viral waktu hoki zeus
AlbertTep –
Hər vaxtınız xeyir, əgər siz keyfiyyətli kazino axtarırsınızsa, mütləq Pin Up saytını yoxlayasınız. Canlı oyunlar və sürətli ödənişlər burada mövcuddur. Qeydiyyatdan keçin və ilk depozit bonusunu götürün. Oynamaq üçün link: [url=https://pinupaz.jp.net/#]Pin Up rəsmi sayt[/url] uğurlar hər kəsə!
VincentPonse –
п»їSalam Gacor, lagi nyari situs slot yang gacor? Coba main di Bonaslot. RTP Live tertinggi hari ini dan pasti bayar. Isi saldo bisa pakai OVO tanpa potongan. Daftar sekarang: п»ї[url=https://bonaslotind.us.com/#]Bonaslot daftar[/url] semoga maxwin.
AlbertTep –
Online slot oynamak isteyenler için kılavuz niteliğinde bir site: https://cassiteleri.us.org/# casino siteleri 2026 Hangi site güvenilir diye düşünmeyin. Onaylı casino siteleri listesi ile rahatça oynayın. Detaylar linkte.
AlbertTep –
Halo Slotter, lagi nyari situs slot yang mudah menang? Coba main di Bonaslot. RTP Live tertinggi hari ini dan terbukti membayar. Deposit bisa pakai Pulsa tanpa potongan. Login disini: slot gacor semoga maxwin.
Shaunsaulk –
п»їSalam Gacor, cari situs slot yang mudah menang? Coba main di Bonaslot. RTP Live tertinggi hari ini dan terbukti membayar. Isi saldo bisa pakai Dana tanpa potongan. Login disini: п»ї[url=https://bonaslotind.us.com/#]Bonaslot rtp[/url] semoga maxwin.
Earnesthed –
Salamlar, siz də etibarlı kazino axtarırsınızsa, mütləq Pin Up saytını yoxlayasınız. Ən yaxşı slotlar və rahat pul çıxarışı burada mövcuddur. İndi qoşulun və ilk depozit bonusunu götürün. Oynamaq üçün link: Pin Up Azerbaijan uğurlar hər kəsə!
MichaelVox –
Hey everyone, I recently discovered a useful international pharmacy for purchasing pills online. If you are looking for cheap meds, OnlinePharm is very good. Great prices plus huge selection. Check it out: buy meds online. Best regards.
Arthurlaw –
To be honest, I just came across an awesome resource to buy medication. If you want to save money and need generic drugs, Pharm Mex is highly recommended. Great prices and it is safe. Check it out: [url=https://pharm.mex.com/#]buy meds from mexico[/url]. Have a great week.
MichaelVox –
Hey everyone, To be honest, I found an excellent source for meds where you can buy generics hassle-free. If you are looking for cheap meds, this site is the best choice. Secure shipping and huge selection. See for yourself: check availability. Kind regards.
CarrolSow –
Hello everyone, I recently discovered a great website for cheap meds. For those seeking and want affordable prescriptions, this store is a game changer. No prescription needed plus very reliable. Check it out: https://pharm.mex.com/#. Peace.
MichaelVox –
Greetings, I just found an excellent online drugstore for purchasing prescription drugs hassle-free. If you need no prescription drugs, this site is worth a look. Great prices and huge selection. See for yourself: https://onlinepharm.jp.net/#. Warmly.
Jamesdix –
To be honest, Just now found an awesome resource to save on Rx. For those seeking and need cheap antibiotics, this site is highly recommended. Fast shipping plus very reliable. Link is here: buy meds from mexico. Cheers.
MichaelVox –
Hey everyone, To be honest, I found an excellent website to order generics hassle-free. If you are looking for antibiotics, this store is highly recommended. Secure shipping and no script needed. Check it out: OnlinePharm. Peace.
Arthurlaw –
To be honest, I just ran into a trusted online source for cheap meds. If you are tired of high prices and want generic drugs, this store is worth checking out. Fast shipping and it is safe. Take a look: https://pharm.mex.com/#. Good luck with everything.
MichaelVox –
Hey there, I just found a great online drugstore where you can buy generics cheaply. If you are looking for no prescription drugs, this store is the best choice. Secure shipping plus it is very affordable. See for yourself: https://onlinepharm.jp.net/#. Best regards.
CarrolSow –
Hi all, I just came across the best website for cheap meds. If you want to buy medicines from India at factory prices, this store is very reliable. It has secure delivery to USA. Visit here: [url=https://indiapharm.in.net/#]indiapharm.in.net[/url]. Good luck.
MichaelVox –
Hi, To be honest, I found an excellent international pharmacy to order pills securely. If you need no prescription drugs, OnlinePharm is highly recommended. Secure shipping plus huge selection. Check it out: Trust Pharmacy online. Have a good one.
DavidWef –
Hello everyone, I just came across an awesome resource for affordable pills. For those seeking and need generic drugs, this site is worth checking out. Great prices and secure. Visit here: [url=https://pharm.mex.com/#]click here[/url]. Peace.
Jamesdix –
Greetings, I recently discovered an awesome resource for affordable pills. If you are tired of high prices and need affordable prescriptions, Pharm Mex is highly recommended. They ship to USA and very reliable. Take a look: https://pharm.mex.com/#. Good luck with everything.
MichaelVox –
Hello, I wanted to share a useful international pharmacy to order medications online. If you need cheap meds, OnlinePharm is very good. Fast delivery and no script needed. Visit here: https://onlinepharm.jp.net/#. Many thanks.
Arthurlaw –
Hello, I just came across an amazing Indian pharmacy to save on Rx. If you want to buy generic pills cheaply, IndiaPharm is very reliable. You get fast shipping worldwide. Take a look: [url=https://indiapharm.in.net/#]check availability[/url]. Hope it helps.
MichaelVox –
Hello, I recently discovered an excellent source for meds for purchasing prescription drugs securely. If you need safe pharmacy delivery, this site is very good. Secure shipping plus it is very affordable. See for yourself: click here. Have a nice day.
CarrolSow –
Hi guys, Lately came across a reliable Mexican pharmacy for affordable pills. If you want to save money and need affordable prescriptions, this store is the best option. No prescription needed plus secure. Take a look: click here. All the best.
MichaelVox –
Hey everyone, I just found an excellent source for meds where you can buy generics hassle-free. If you are looking for cheap meds, this site is very good. Fast delivery plus no script needed. Link here: [url=https://onlinepharm.jp.net/#]cheap pharmacy online[/url]. I hope you find what you need.
Jamesdix –
Hello everyone, Just now discovered a reliable online source for cheap meds. For those seeking and want cheap antibiotics, Pharm Mex is worth checking out. Great prices plus very reliable. Check it out: cheap antibiotics mexico. Best of luck.
MichaelVox –
Hey there, I just found a useful website to order medications hassle-free. For those who need safe pharmacy delivery, OnlinePharm is very good. Secure shipping and it is very affordable. Link here: https://onlinepharm.jp.net/#. Have a nice day.
Arthurlaw –
Greetings, Just now discovered a useful website to buy generics. For those looking for cheap antibiotics without prescription, this site is highly recommended. It has fast shipping worldwide. Check it out: indian pharmacy. Best regards.
MichaelVox –
Hello, I recently discovered an excellent source for meds for purchasing generics securely. If you need antibiotics, OnlinePharm is worth a look. They ship globally plus no script needed. See for yourself: onlinepharm.jp.net. Regards.
MichaelVox –
Hey everyone, To be honest, I found a reliable online drugstore where you can buy pills cheaply. For those who need safe pharmacy delivery, OnlinePharm is worth a look. Great prices plus huge selection. Link here: [url=https://onlinepharm.jp.net/#]click here[/url]. Thx.
CarrolSow –
Greetings, Just now stumbled upon a great source from India to save on Rx. For those looking for cheap antibiotics cheaply, this site is very reliable. It has wholesale rates worldwide. Visit here: [url=https://indiapharm.in.net/#]read more[/url]. Best regards.
DavidWef –
Hello, I recently found the best online drugstore for cheap meds. For those looking for ED meds safely, this site is highly recommended. They offer wholesale rates worldwide. Visit here: buy meds from india. Good luck.
Jamesdix –
Hello, Lately found a great online drugstore for affordable pills. If you want to buy generic pills without prescription, this site is worth checking. You get wholesale rates to USA. Visit here: cheap indian generics. Best regards.
MichaelVox –
Hey everyone, To be honest, I found an excellent online drugstore where you can buy pills cheaply. If you need antibiotics, OnlinePharm is the best choice. Great prices plus no script needed. Visit here: https://onlinepharm.jp.net/#. Peace.
Arthurlaw –
To be honest, Lately discovered an awesome website for cheap meds. For those seeking and need cheap antibiotics, this site is the best option. No prescription needed and it is safe. Check it out: read more. Be well.
MichaelVox –
Hey everyone, I just found a useful international pharmacy where you can buy prescription drugs securely. For those who need antibiotics, this site is the best choice. Fast delivery and no script needed. See for yourself: buy meds online. Warmly.
MichaelVox –
Hey there, I just found a reliable international pharmacy where you can buy generics securely. For those who need no prescription drugs, this store is worth a look. Great prices and no script needed. Link here: [url=https://onlinepharm.jp.net/#]safe online drugstore[/url]. Sincerely.
CarrolSow –
To be honest, Lately discovered an amazing website to buy generics. If you need cheap antibiotics cheaply, this store is worth checking. You get wholesale rates worldwide. Visit here: [url=https://indiapharm.in.net/#]cheap indian generics[/url]. Cheers.
Jamesdix –
Hey there, I recently discovered a reliable Mexican pharmacy for cheap meds. If you are tired of high prices and want generic drugs, this store is highly recommended. No prescription needed plus secure. Visit here: read more. Thx.
MichaelVox –
Greetings, I wanted to share a useful website to order pills hassle-free. For those who need safe pharmacy delivery, this site is very good. They ship globally and it is very affordable. Link here: https://onlinepharm.jp.net/#. Have a great week.
MichaelVox –
Hey there, To be honest, I found a great online drugstore where you can buy pills securely. If you need antibiotics, this store is highly recommended. They ship globally and it is very affordable. Visit here: https://onlinepharm.jp.net/#. Best regards.
Arthurlaw –
Greetings, I recently ran into an awesome Mexican pharmacy to save on Rx. If you are tired of high prices and need cheap antibiotics, this store is a game changer. Great prices and secure. Visit here: click here. Best wishes.
MichaelVox –
Greetings, To be honest, I found a great online drugstore to order pills cheaply. For those who need cheap meds, OnlinePharm is the best choice. They ship globally plus huge selection. See for yourself: cheap pharmacy online. Best regards.
MichaelVox –
Hey everyone, I wanted to share a useful online drugstore where you can buy medications online. If you are looking for cheap meds, this store is highly recommended. Secure shipping and no script needed. Visit here: [url=https://onlinepharm.jp.net/#]buy meds online[/url]. Have a nice day.
CarrolSow –
Hello, Just now discovered a useful online drugstore to save on Rx. If you need ED meds safely, this site is highly recommended. It has lowest prices to USA. More info here: [url=https://indiapharm.in.net/#]India Pharm Store[/url]. Best regards.
Jamesdix –
Hello, Lately found the best website for cheap meds. For those looking for cheap antibiotics safely, this site is worth checking. It has secure delivery guaranteed. Take a look: https://indiapharm.in.net/#. Good luck.
MichaelVox –
Hey there, To be honest, I found a great international pharmacy for purchasing prescription drugs cheaply. If you are looking for cheap meds, this store is highly recommended. Fast delivery and no script needed. See for yourself: https://onlinepharm.jp.net/#. Cheers.
DavidWef –
To be honest, I recently came across a great resource to buy medication. For those seeking and want cheap antibiotics, this site is worth checking out. They ship to USA plus it is safe. Check it out: [url=https://pharm.mex.com/#]check availability[/url]. Have a great week.
Arthurlaw –
Greetings, Lately stumbled upon an amazing online drugstore for affordable pills. For those looking for generic pills cheaply, this store is worth checking. It has lowest prices worldwide. Check it out: [url=https://indiapharm.in.net/#]buy meds from india[/url]. Best regards.
MichaelVox –
Greetings, To be honest, I found an excellent online drugstore to order medications securely. If you are looking for cheap meds, this site is very good. Great prices plus it is very affordable. Check it out: onlinepharm.jp.net. Best regards.
CarrolSow –
Hi all, I recently stumbled upon an amazing Indian pharmacy to save on Rx. For those looking for medicines from India without prescription, this site is highly recommended. It has fast shipping to USA. Visit here: https://indiapharm.in.net/#. Good luck.
Jamesdix –
To be honest, Just now discovered a useful website to buy generics. If you want to buy generic pills at factory prices, IndiaPharm is very reliable. They offer fast shipping worldwide. Visit here: https://indiapharm.in.net/#. Cheers.
glzneewng –
للاستفادة القصوى من PredictorAviator مهكر، إليك بعض النصائح العملية: إن تنزيل وتثبيت تطبيق Aviator Signals هو نفسه كما في حالة Predictor. كن حذرًا واستخدم البرامج من مصادر موثوقة فقط. The Predictor Aviator app is packed with several advanced features designed to give players an edge. One of its standout features is the real-time prediction engine, which analyzes game patterns and historical data to forecast when the plane is likely to crash. The app also includes a customizable alert system, allowing users to set their desired risk levels and receive notifications when the odds are favorable for cashing out. يمكنك استنساخ مثيلات متعددة بسهولة وبدء المزامنة حتى تحصل على العنصر المطلوب قبل ربط حسابك، مما يعزز الكفاءة في عمليات Reroll في Predictor aviator Real.
https://jobs.windomnews.com/profiles/7625341-alison-kruit
فلعبة Infinite Flight هي افضل خيار لك عزيزي القارئ تملك العديد من الرسومات الجوية المدهشة بالإضافة على انها لعبة غامرة ومدهشة إلى حد لا يوصف وعلاوة على ماتم ذكره فلعبة Infinite Flight. لعبة الاتاري القديمة ممتعة كثيراً و لعبة اتاري سوف تلعب وتستمتع بنفس العاب الاتاري وتجتاز المراحل وتنجز الأهداف و تتضمن مجموعة متنوعة من المراحل والألعاب المصغرة الممتعة وان كنت تشعر بالحنين إلى الألعاب القديمة التي كانت جزء من طفولتنا وتركت بصمة في حياتنا في هذه اللعبه سوف تعيدك الى ايام الطفولة فسوف تلعب لعبة اتارى الطائرات القديمة لعبة الثعبان والسيارات القديمة وسوف تستمتع.
Arthurlaw –
To be honest, I recently came across a great Indian pharmacy for cheap meds. If you need medicines from India at factory prices, this store is the best place. You get wholesale rates to USA. Take a look: [url=https://indiapharm.in.net/#]buy meds from india[/url]. Hope it helps.
CarrolSow –
Hello everyone, Just now discovered a trusted online source to buy medication. For those seeking and need meds from Mexico, this site is the best option. They ship to USA and very reliable. Take a look: https://pharm.mex.com/#. Best regards.
Jamesdix –
Greetings, Lately stumbled upon the best online drugstore for affordable pills. For those looking for cheap antibiotics safely, IndiaPharm is highly recommended. It has secure delivery guaranteed. More info here: [url=https://indiapharm.in.net/#]check availability[/url]. Best regards.
Arthurlaw –
Hey there, I just found a trusted Mexican pharmacy to buy medication. For those seeking and want cheap antibiotics, this store is a game changer. No prescription needed and very reliable. Link is here: https://pharm.mex.com/#. Good luck!
Casey –
%random_anchor_text%
References:
brewwiki.win
DavidWef –
Greetings, Just now came across the best online drugstore for affordable pills. If you want to buy ED meds safely, this site is very reliable. You get secure delivery worldwide. More info here: [url=https://indiapharm.in.net/#]cheap indian generics[/url]. Best regards.
Jamesdix –
To be honest, Lately ran into an awesome website for cheap meds. If you are tired of high prices and need meds from Mexico, Pharm Mex is highly recommended. Great prices and it is safe. Link is here: https://pharm.mex.com/#. Have a great week.
Jamesdix –
Hey there, I just came across an awesome Mexican pharmacy to buy medication. If you want to save money and want affordable prescriptions, this store is highly recommended. They ship to USA plus very reliable. Visit here: https://pharm.mex.com/#. Many thanks.
CarrolSow –
Hi guys, I just discovered a great online source to save on Rx. For those seeking and need cheap antibiotics, this site is highly recommended. Fast shipping plus it is safe. Visit here: visit website. Peace.
Arthurlaw –
Hey guys, Lately came across a useful online drugstore to buy generics. If you want to buy ED meds without prescription, IndiaPharm is very reliable. You get wholesale rates to USA. Check it out: [url=https://indiapharm.in.net/#]indian pharmacy online[/url]. Cheers.
DavidQuics –
Matbet TV güncel linki lazımsa işte burada. Sorunsuz için: Giriş Yap Yüksek oranlar bu sitede. Gençler, Matbet bahis son linki açıklandı.
Georgemob –
Herkese selam, Casibom sitesi kullan?c?lar? ad?na onemli bir paylas?m yapmak istiyorum. Herkesin bildigi uzere site adresini erisim k?s?tlamas? nedeniyle tekrar guncelledi. Giris sorunu yas?yorsan?z dogru yerdesiniz. Guncel Casibom guncel giris adresi art?k asag?dad?r https://casibom.mex.com/# Paylast?g?m baglant? ile direkt siteye baglanabilirsiniz. Ek olarak kay?t olanlara sunulan freespin kampanyalar?n? mutlaka kac?rmay?n. Lisansl? bahis deneyimi surdurmek icin Casibom dogru adres. Herkese bol kazanclar dilerim.
RicardoWeade –
Gencler, Grandpashabet Casino yeni adresi ac?kland?. Giremeyenler buradan devam edebilir https://grandpashabet.in.net/#
AntioneTwele –
Herkese selam, Casibom sitesi oyuncuları adına önemli bir duyuru paylaşıyorum. Bildiğiniz gibi site giriş linkini erişim kısıtlaması nedeniyle sürekli güncelledi. Erişim hatası varsa link aşağıda. Güncel siteye erişim linki artık aşağıdadır Casibom Giriş Bu link ile direkt hesabınıza bağlanabilirsiniz. Ek olarak kayıt olanlara sunulan yatırım bonusu fırsatlarını da kaçırmayın. Lisanslı casino keyfi için Casibom doğru adres. Tüm forum üyelerine bol kazançlar dilerim.
RicardoWeade –
Dostlar selam, Casibom kullan?c?lar? icin onemli bir duyuru yapmak istiyorum. Herkesin bildigi uzere site giris linkini BTK engeli yuzunden surekli guncelledi. Giris problemi cekenler icin cozum burada. Yeni Casibom giris linki su an asag?dad?r [url=https://casibom.mex.com/#]Buraya T?kla[/url] Paylast?g?m baglant? ile dogrudan hesab?n?za erisebilirsiniz. Ek olarak yeni uyelere sunulan freespin kampanyalar?n? mutlaka inceleyin. Lisansl? slot keyfi surdurmek icin Casibom tercih edebilirsiniz. Tum forum uyelerine bol sans dilerim.
DavidQuics –
Herkese selam, bu site kullanıcıları için önemli bir bilgilendirme yapmak istiyorum. Bildiğiniz gibi Vaycasino adresini yine güncelledi. Erişim hatası varsa panik yapmayın. Son Vaycasino giriş adresi artık burada: [url=https://vaycasino.us.com/#]Vay Casino Güncel Adres[/url] Bu link ile direkt hesabınıza erişebilirsiniz. Güvenilir bahis keyfi için Vay Casino doğru adres. Tüm forum üyelerine bol şans dilerim.
AntioneTwele –
Arkadaşlar, Grandpashabet Casino yeni adresi açıklandı. Giremeyenler şu linkten giriş yapabilir https://grandpashabet.in.net/#
RicardoWeade –
Grandpasha guncel linki ar?yorsan?z dogru yerdesiniz. H?zl? erisim icin t?kla https://grandpashabet.in.net/# Deneme bonusu burada.
Georgemob –
Bahis severler selam, Casibom sitesi kullan?c?lar? icin onemli bir bilgilendirme yapmak istiyorum. Bildiginiz gibi bahis platformu domain adresini erisim k?s?tlamas? nedeniyle tekrar tas?d?. Giris hatas? varsa link asag?da. Son siteye erisim baglant?s? su an asag?dad?r [url=https://casibom.mex.com/#]Casibom Apk[/url] Paylast?g?m baglant? uzerinden dogrudan hesab?n?za erisebilirsiniz. Ek olarak yeni uyelere sunulan yat?r?m bonusu f?rsatlar?n? da inceleyin. En iyi bahis deneyimi surdurmek icin Casibom tercih edebilirsiniz. Herkese bol sans dilerim.
DavidQuics –
Dostlar selam, Vay Casino oyuncuları için önemli bir duyuru paylaşıyorum. Bildiğiniz gibi site giriş linkini yine değiştirdi. Giriş hatası varsa endişe etmeyin. Son siteye erişim linki şu an burada: Vaycasino Sorunsuz Giriş Paylaştığım bağlantı ile vpn kullanmadan hesabınıza erişebilirsiniz. Güvenilir bahis deneyimi sürdürmek için Vaycasino doğru adres. Herkese bol kazançlar dilerim.
RicardoWeade –
Herkese merhaba, Vaycasino kullan?c?lar? ad?na onemli bir duyuru yapmak istiyorum. Malum platform adresini yine guncelledi. Erisim sorunu varsa panik yapmay?n. Guncel Vay Casino giris linki su an burada: https://vaycasino.us.com/# Bu link ile vpn kullanmadan siteye girebilirsiniz. Lisansl? casino keyfi icin Vay Casino tercih edebilirsiniz. Herkese bol kazanclar dilerim.
DavidQuics –
Herkese selam, Vay Casino oyuncuları için kısa bir duyuru yapmak istiyorum. Bildiğiniz gibi platform giriş linkini tekrar güncelledi. Erişim sorunu yaşıyorsanız panik yapmayın. Yeni Vay Casino giriş linki artık aşağıdadır: https://vaycasino.us.com/# Paylaştığım bağlantı üzerinden vpn kullanmadan siteye girebilirsiniz. Güvenilir bahis deneyimi için Vaycasino doğru adres. Herkese bol kazançlar temenni ederim.
Georgemob –
Dostlar selam, Vaycasino oyuncular? ad?na k?sa bir bilgilendirme paylas?yorum. Bildiginiz gibi platform giris linkini yine guncelledi. Erisim hatas? varsa panik yapmay?n. Yeni Vay Casino giris adresi art?k asag?dad?r: [url=https://vaycasino.us.com/#]Vaycasino Kay?t[/url] Bu link uzerinden direkt siteye girebilirsiniz. Lisansl? casino keyfi surdurmek icin Vay Casino dogru adres. Tum forum uyelerine bol sans dilerim.
RicardoWeade –
Dostlar selam, Casibom oyuncular? ad?na onemli bir duyuru paylas?yorum. Bildiginiz gibi Casibom domain adresini erisim k?s?tlamas? nedeniyle tekrar guncelledi. Erisim sorunu varsa cozum burada. Guncel Casibom guncel giris baglant?s? su an paylas?yorum [url=https://casibom.mex.com/#]Casibom Apk[/url] Paylast?g?m baglant? ile dogrudan hesab?n?za girebilirsiniz. Ayr?ca yeni uyelere verilen yat?r?m bonusu f?rsatlar?n? da kac?rmay?n. Lisansl? slot keyfi icin Casibom tercih edebilirsiniz. Tum forum uyelerine bol kazanclar dilerim.
DavidQuics –
Arkadaşlar selam, Vay Casino kullanıcıları için önemli bir bilgilendirme paylaşıyorum. Malum platform giriş linkini yine değiştirdi. Erişim sorunu yaşıyorsanız endişe etmeyin. Son Vaycasino giriş adresi artık burada: Vay Casino Giriş Bu link üzerinden doğrudan hesabınıza erişebilirsiniz. Lisanslı bahis keyfi sürdürmek için Vaycasino doğru adres. Herkese bol şans temenni ederim.
RicardoWeade –
Herkese selam, bu populer site uyeleri icin onemli bir duyuru paylas?yorum. Herkesin bildigi uzere Casibom adresini erisim k?s?tlamas? nedeniyle yine guncelledi. Erisim hatas? cekenler icin link asag?da. Cal?san Casibom guncel giris adresi su an burada [url=https://casibom.mex.com/#]Casibom Twitter[/url] Bu link uzerinden dogrudan siteye girebilirsiniz. Ayr?ca kay?t olanlara verilen hosgeldin bonusu f?rsatlar?n? da kac?rmay?n. En iyi slot keyfi surdurmek icin Casibom tercih edebilirsiniz. Herkese bol sans dilerim.
DavidQuics –
Arkadaşlar selam, Casibom sitesi kullanıcıları adına kısa bir paylaşım paylaşıyorum. Herkesin bildiği üzere site giriş linkini erişim kısıtlaması nedeniyle sürekli değiştirdi. Siteye ulaşım hatası yaşıyorsanız çözüm burada. Son Casibom giriş adresi artık paylaşıyorum Casibom Üyelik Bu link üzerinden direkt siteye erişebilirsiniz. Ek olarak kayıt olanlara verilen hoşgeldin bonusu fırsatlarını mutlaka kaçırmayın. En iyi casino keyfi için Casibom doğru adres. Herkese bol şans dilerim.
Georgemob –
Grandpasha guncel linki laz?msa dogru yerdesiniz. Sorunsuz giris yapmak icin [url=https://grandpashabet.in.net/#]Grandpasha Giris[/url] Yuksek oranlar bu sitede.
RicardoWeade –
Grandpashabet giris linki laz?msa dogru yerdesiniz. H?zl? erisim icin [url=https://grandpashabet.in.net/#]Grandpashabet Apk[/url] Deneme bonusu bu sitede.
DavidQuics –
Matbet TV giriş linki arıyorsanız doğru yerdesiniz. Hızlı için tıkla: [url=https://matbet.jp.net/#]Matbet Mobil[/url] Canlı maçlar bu sitede. Gençler, Matbet yeni adresi belli oldu.
RicardoWeade –
Dostlar selam, bu site oyuncular? ad?na onemli bir bilgilendirme paylas?yorum. Bildiginiz gibi platform giris linkini yine guncelledi. Erisim sorunu yas?yorsan?z panik yapmay?n. Yeni siteye erisim linki art?k burada: Buraya T?kla Paylast?g?m baglant? ile dogrudan siteye girebilirsiniz. Guvenilir bahis deneyimi icin Vay Casino dogru adres. Tum forum uyelerine bol sans temenni ederim.
DavidQuics –
Matbet güncel linki lazımsa doğru yerdesiniz. Sorunsuz için tıkla: [url=https://matbet.jp.net/#]Matbet Giriş[/url] Yüksek oranlar bu sitede. Arkadaşlar, Matbet son linki açıklandı.
RicardoWeade –
Herkese merhaba, bu site oyuncular? ad?na k?sa bir duyuru yapmak istiyorum. Bildiginiz gibi platform giris linkini tekrar degistirdi. Giris hatas? varsa panik yapmay?n. Son siteye erisim adresi su an burada: Vay Casino Apk Bu link ile vpn kullanmadan hesab?n?za girebilirsiniz. Lisansl? casino deneyimi surdurmek icin Vay Casino tercih edebilirsiniz. Herkese bol kazanclar temenni ederim.
Georgemob –
Matbet TV guncel linki laz?msa dogru yerdesiniz. Sorunsuz icin: Matbet Uyelik Canl? maclar bu sitede. Gencler, Matbet bahis son linki belli oldu.
DavidQuics –
Herkese merhaba, Casibom kullanıcıları adına önemli bir duyuru yapmak istiyorum. Herkesin bildiği üzere Casibom adresini erişim kısıtlaması nedeniyle tekrar değiştirdi. Erişim sorunu çekenler için link aşağıda. Çalışan siteye erişim linki artık burada [url=https://casibom.mex.com/#]Casibom Mobil[/url] Bu link üzerinden vpn kullanmadan siteye girebilirsiniz. Ek olarak kayıt olanlara verilen yatırım bonusu kampanyalarını da kaçırmayın. Lisanslı bahis deneyimi için Casibom doğru adres. Tüm forum üyelerine bol şans dilerim.
RicardoWeade –
Herkese merhaba, bu populer site uyeleri icin onemli bir duyuru paylas?yorum. Herkesin bildigi uzere site giris linkini erisim k?s?tlamas? nedeniyle surekli guncelledi. Erisim hatas? cekenler icin link asag?da. Resmi Casibom giris linki art?k paylas?yorum Casibom Guncel Bu link ile dogrudan hesab?n?za erisebilirsiniz. Ayr?ca yeni uyelere sunulan yat?r?m bonusu f?rsatlar?n? da inceleyin. Guvenilir bahis deneyimi icin Casibom dogru adres. Tum forum uyelerine bol kazanclar dilerim.
DavidQuics –
Matbet giriş adresi arıyorsanız işte burada. Maç izlemek için: https://matbet.jp.net/# Yüksek oranlar burada. Gençler, Matbet bahis yeni adresi açıklandı.
Georgemob –
Arkadaslar, Grandpashabet Casino son linki belli oldu. Giremeyenler su linkten giris yapabilir [url=https://grandpashabet.in.net/#]Grandpashabet Apk[/url]
Georgemob –
Gencler, Grandpashabet Casino son linki belli oldu. Giremeyenler buradan devam edebilir Grandpashabet Yeni Adres
zuczjmcme –
© 2025 Stop and Step – Online Casino Slot Reviews, Slots and Casino Streamer. All Rights Reserved. Getting proactive and acquire all gold coins before water robbers can also be come to them, the individuals could even be around to unregistered profiles. The good cellular platform support increase being compatible along with other gizmos beyond Screen Desktop and you may Mac computer, the new turtle as well as the jellyfish go after well away and therefore are detailed in 2 platforms. The fresh Betfinal Gambling establishment Arab is just one of the greatest web based casinos in the arabic vocabulary, however. Welcome to the tropical Hawaiian island in one of the most popular and innovative slot games released by NetEnt – Aloha! Cluster Pays. Also known as grid slots, Cluster Pays slots are on the rise. All slot studios now offer slot games with the Cluster Pays mechanic. In my in-depth guide, I look at what Cluster Pays is, how payouts or winning combinations are formed, what you can expect and the bonus features you’ll encounter.
https://lorranechiaramonte.com.br/?p=53731
Players can get started with a minimum bet of 0.10, but if the high rollers out there are feeling lucky, they can stretch that all the way up to a huge maximum of 200. It becomes unsafe for Sunflower State players once they begin to gamble on unverified sources that can be illegal and unsecured, aloha cluster pays a game guide and tips the logo of Blade is the Scatter symbol and Blade Split triggers the Split feature. The low and medium symbol categories can create winning outcomes between 0.10x and 2x your bet, but one major change could come if the state strikes a deal with a third-party mobile lotto app such as Jackpocket. After those symbols vanish, I had to adjust the zoom setting to 50%. The best feature in the game is the Free Spins Round, european roulette pro with bonus in order to see the reel grid and bet configurations in full.
KevinOrals –
Chao c? nha, bac nao mu?n tim trang choi xanh chin d? g? g?c N? Hu thi vao ngay d?a ch? nay. Dang co khuy?n mai: [url=https://pacebhadrak.org.in/#]Link vao BJ88[/url]. Chuc anh em may m?n.
KevinOrals –
Chao c? nha, ai dang tim nha cai uy tin d? g? g?c N? Hu thi tham kh?o ch? nay. T?c d? ban th?: https://homemaker.org.in/#. Chuc cac bac r?c r?.
xbklmflwn –
Um último esforço para destruir o que antes seria nosso salvador. Uma missão final para eliminar um futuro desastroso. Uma única nave contra todo o exército da Terra. O Andraste é a única esperança de derrotar… o Devil Engine. Devil Engine é um jogo de tiro com rolagem lateral de estilo clássico e de alta octanagem, fortemente influenciado pelos melhores do gênero da era de 32 bits, apresentando uma variedade de locais incríveis, pixel art desenhado à mão e uma trilha sonora emocionante que dá vida ao futuro sombrio. O jogo Ninja Crash que paga é uma criação da Galaxsys, uma provedora que já tem dezenas de jogos de aposta online em seu catálogo. Ela está fechando parcerias com plataformas confiáveis aos poucos, mas já encontramos jogos como esse em alguns bons cassinos. A garantia que temos de que o Ninja Crash é confiável está em como o jogo foi produzido.
https://adaguen.com/2026/01/16/spaceman-aposta-online-guia-completo-para-apostar/
Podes fazer um depósito das seguintes formas: O depósito mínimo é de 0,1 mBTC. Método de depósito As limitações na ToisBet para sacar fundos após jogar Ninja Crash são de não mais que $1000. O jogo Ninja Crash que paga é uma criação da Galaxsys, uma provedora que já tem dezenas de jogos de aposta online em seu catálogo. Ela está fechando parcerias com plataformas confiáveis aos poucos, mas já encontramos jogos como esse em alguns bons cassinos. A garantia que temos de que o Ninja Crash é confiável está em como o jogo foi produzido. O jogo Ninja Crash é um crash game com dinâmica fácil de entender. Método de depósito A estratégia do melhor horário do Ninja Crash é a mais popular entre os jogadores. Atualmente, buscar os chamados minutos pagantes é a forma com que usuários tentam prever os resultados para ganhar nos jogos de aposta. Não há motivo que nos leve a acreditar que um horário específico faça o Ninja Crash pagar mais, mas testamos a abordagem mesmo assim para encontrar os seguintes momentos de pagamento:
KevinOrals –
Xin chao 500 anh em, ai dang tim trang choi xanh chin d? cay cu?c Tai X?u thi tham kh?o d?a ch? nay. Dang co khuy?n mai: [url=https://pacebhadrak.org.in/#]T?i app BJ88[/url]. Chi?n th?ng nhe.
KevinOrals –
Chao anh em, n?u anh em dang ki?m nha cai uy tin d? choi Casino thi tham kh?o d?a ch? nay. Khong lo l?a d?o: https://pacebhadrak.org.in/#. Chuc cac bac r?c r?.
LouisZew –
Chào cả nhà, nếu anh em đang kiếm trang chơi xanh chín để chơi Đá Gà thì xem thử trang này nhé. Tốc độ bàn thờ: https://homemaker.org.in/#. Húp lộc đầy nhà.
LouisZew –
Chào anh em, ai đang tìm sân chơi đẳng cấp để gỡ gạc Đá Gà thì vào ngay con hàng này. Đang có khuyến mãi: https://homemaker.org.in/#. Chúc các bác rực rỡ.
KevinOrals –
Xin chao 500 anh em, ngu?i anh em nao c?n san choi d?ng c?p d? g? g?c Game bai thi xem th? d?a ch? nay. Dang co khuy?n mai: [url=https://gramodayalawcollege.org.in/#]Link khong b? ch?n[/url]. Chi?n th?ng nhe.
LouisZew –
Hi các bác, ai đang tìm sân chơi đẳng cấp để cày cuốc Đá Gà đừng bỏ qua con hàng này. Không lo lừa đảo: [url=https://homemaker.org.in/#]sun win[/url]. Chúc anh em may mắn.
LouisZew –
Chào anh em, người anh em nào cần trang chơi xanh chín để chơi Đá Gà đừng bỏ qua con hàng này. Nạp rút 1-1: https://homemaker.org.in/#. Chiến thắng nhé.
Edwardblibe –
Follicle Insight [url=https://follicle.us.com/#]cheap propecia without insurance[/url] Follicle Insight
Marcusunick –
where to buy stromectol online: Iver Protocols Guide – stromectol canada
Marcusunick –
AmiTrip Relief Store: Amitriptyline – Elavil
Edwardblibe –
fertility pct guide [url=https://fertilitypctguide.us.com/#]fertility pct guide[/url] can i buy clomid for sale
Marcusunick –
fertility pct guide: fertility pct guide – fertility pct guide
Marcusunick –
can i purchase cheap clomid prices: order cheap clomid without prescription – clomid
WalterRag –
https://follicle.us.com/# buy cheap propecia
StevenMaf –
https://fertilitypctguide.us.com/# fertility pct guide
Michaelshisp –
Iver Protocols Guide: Iver Protocols Guide – stromectol 6 mg tablet
Edwardblibe –
Elavil [url=https://amitrip.us.com/#]AmiTrip Relief Store[/url] Elavil
Marcusunick –
stromectol 3 mg: stromectol 12mg – Iver Protocols Guide
StevenMaf –
https://follicle.us.com/# Follicle Insight
Michaelshisp –
Iver Protocols Guide: ivermectin lotion for lice – cost of ivermectin medicine
WalterRag –
https://fertilitypctguide.us.com/# fertility pct guide
Marcusunick –
get cheap propecia without dr prescription: buying propecia without prescription – cheap propecia prices
StevenMaf –
https://iver.us.com/# ivermectin 3mg pill
Michaelshisp –
Follicle Insight: Follicle Insight – cheap propecia tablets
Edwardblibe –
order generic propecia pill [url=https://follicle.us.com/#]cost of generic propecia without dr prescription[/url] Follicle Insight
Marcusunick –
fertility pct guide: can i buy clomid without a prescription – fertility pct guide
StevenMaf –
https://follicle.us.com/# Follicle Insight
WalterRag –
https://follicle.us.com/# Follicle Insight
Michaelshisp –
where buy clomid for sale: buying generic clomid without prescription – how to get cheap clomid without a prescription
Marcusunick –
fertility pct guide: fertility pct guide – can i order generic clomid pills
StevenMaf –
https://iver.us.com/# stromectol 3mg tablets
WalterRag –
https://amitrip.us.com/# AmiTrip Relief Store
Edwardblibe –
propecia without dr prescription [url=https://follicle.us.com/#]cost of generic propecia[/url] buy propecia for sale
Marcusunick –
cost of cheap propecia no prescription: buying generic propecia – buy cheap propecia
StevenMaf –
https://follicle.us.com/# cost of generic propecia without rx
Michaelshisp –
fertility pct guide: fertility pct guide – fertility pct guide
Marcusunick –
cost of cheap propecia without rx: cost generic propecia price – cost cheap propecia price
StevenMaf –
https://amitrip.us.com/# buy Elavil
WalterRag –
https://follicle.us.com/# propecia generics
Michaelshisp –
Elavil: Elavil – AmiTrip
Marcusunick –
Follicle Insight: propecia cost – propecia order
Edwardblibe –
Elavil [url=https://amitrip.us.com/#]Elavil[/url] Amitriptyline
WalterRag –
https://fertilitypctguide.us.com/# fertility pct guide
Michaelshisp –
Amitriptyline: AmiTrip – Elavil
StevenMaf –
https://iver.us.com/# Iver Protocols Guide
Marcusunick –
ivermectin price uk: Iver Protocols Guide – Iver Protocols Guide
Michaelshisp –
get generic propecia price: cost cheap propecia prices – buy cheap propecia
StevenMaf –
https://amitrip.us.com/# Generic Elavil
WalterRag –
https://amitrip.us.com/# AmiTrip
Marcusunick –
Elavil: AmiTrip – Generic Elavil
Edwardblibe –
Iver Protocols Guide [url=https://iver.us.com/#]stromectol in canada[/url] Iver Protocols Guide
Michaelshisp –
fertility pct guide: fertility pct guide – cost of generic clomid without dr prescription
Duanefuh –
Hi all, if you are looking for a useful article about health treatments, check out this health wiki. You can read about usage and risks in detail. Read more here: https://magmaxhealth.com/Prilosec. Very informative.
Matthewsmeak –
Hi, if you need a reliable source for meds to order pills hassle-free. Check out this pharmacy: MagMaxHealth. They offer a wide range of meds and huge discounts. Good luck.
Davidnob –
Hey everyone, if you are looking for a great drugstore to purchase pills cheaply. Take a look at this site: lipitor. They offer high quality drugs with fast shipping. Cheers.
MilesHap –
Hi all, I recently found a useful article on various medications, take a look at this medical reference. It covers usage and risks in detail. Reference: https://magmaxhealth.com/Prilosec. Thanks.
HarryProli –
To start saving, visit this top-rated pharmacy pharmacy online usa for the best prices. Get your meds today and save big.
Davidnob –
Hey everyone, I wanted to share a reliable online pharmacy to order health products online. I recommend MagMaxHealth: MagMaxHealth. Selling a wide range of meds at the best prices. Thanks.
Duanefuh –
Hi, if you are looking for detailed information regarding various medications, check out this drug database. It covers drug interactions clearly. Reference: https://magmaxhealth.com/Toradol. Hope this is useful.
MilesHap –
Hey everyone, I recently found detailed information about various medications, I recommend this health wiki. You can read about drug interactions in detail. Source: https://magmaxhealth.com/Protonix. Hope this is useful.
HarryProli –
If you are looking for visit this top-rated pharmacy here to order now. Get your meds today hassle-free.
Donaldutics –
For a complete overview of safety protocols, it is recommended to check the detailed guide on: https://magmaxhealth.com/protonix.html for risk management.
Davidnob –
Hi guys, if you are looking for a great drugstore to buy pills online. I recommend this pharmacy: protonix. Stocking high quality drugs with fast shipping. Cheers.
Duanefuh –
Hi all, if anyone needs detailed information on various medications, I found this online directory. It explains safety protocols very well. See details: https://magmaxhealth.com/Rosuvastatin. Hope it helps.
Danielvof –
In terms of safety protocols, you can consult the medical directory at: https://magmaxhealth.com/lipitor.html for correct administration.
Davidnob –
Hi guys, if you need a trusted health store to purchase prescription drugs securely. I recommend this pharmacy: meclizine. Stocking generic tablets at the best prices. Thanks.
MilesHap –
Hello, I recently found a useful article regarding common medicines, check out this useful resource. It covers usage and risks very well. See details: https://magmaxhealth.com/Clarinex. Hope it helps.
Duanefuh –
Hey everyone, if you are looking for detailed information about various medications, check out this drug database. It explains safety protocols in detail. Read more here: https://magmaxhealth.com/Toradol. Very informative.
Donaldutics –
For a complete overview of proper usage instructions, data is available at the official information page at: https://magmaxhealth.com/celebrex.html for safe treatment.
Danielvof –
To understand the safety protocols, you can consult the official information page at: https://magmaxhealth.com/toradol.html to ensure risk management.
Duanefuh –
Greetings, if anyone needs dosage instructions on common medicines, I found this health wiki. It covers how to take meds in detail. See details: https://magmaxhealth.com. Hope this is useful.
Davidnob –
Hi, if you are looking for a great source for meds to buy prescription drugs cheaply. I recommend MagMaxHealth: olanzapine. Selling a wide range of meds and huge discounts. Best regards.
Duanefuh –
Greetings, if anyone needs side effects info on common medicines, take a look at this useful resource. It explains usage and risks very well. Read more here: https://magmaxhealth.com/Toradol. Thanks.
JamesGycle –
omeprazole prilosec: omeprazole prilosec – Gastro Health Monitor
Jeffreytoumn –
http://gastrohealthmonitor.com/# Gastro Health Monitor
JamesGycle –
Gastro Health Monitor: Gastro Health Monitor – Gastro Health Monitor
Alfonsosmemn –
https://nauseacareus.shop/# zofran medication
Conradwaf –
methocarbamol medication: muscle relaxant drugs – robaxin generic
Davidrer –
prilosec generic [url=https://gastrohealthmonitor.com/#]omeprazole[/url] omeprazole otc
JamesGycle –
Nausea Care US: generic zofran – zofran otc
JamesGycle –
omeprazole medication: Gastro Health Monitor – Gastro Health Monitor
Jeffreytoumn –
https://spasmreliefprotocols.shop/# tizanidine hydrochloride
JamesGycle –
buy methocarbamol: Spasm Relief Protocols – tizanidine hcl
JamesGycle –
best muscle relaxer: Spasm Relief Protocols – muscle relaxant drugs
Conradwaf –
generic prilosec: Gastro Health Monitor – Gastro Health Monitor
JamesGycle –
prilosec generic: Gastro Health Monitor – omeprazole generic
Jeffreytoumn –
http://gastrohealthmonitor.com/# Gastro Health Monitor
JamesGycle –
Nausea Care US: Nausea Care US – Nausea Care US
JamesGycle –
Nausea Care US: Nausea Care US – buy zofran
JamesGycle –
Gastro Health Monitor: prilosec generic – Gastro Health Monitor
Davidrer –
zofran generic [url=https://nauseacareus.shop/#]zofran medication[/url] zofran medication
Jeffreytoumn –
https://nauseacareus.com/# п»їondansetron otc
Conradwaf –
Gastro Health Monitor: prilosec side effects – buy prilosec online
JamesGycle –
omeprazole: Gastro Health Monitor – Gastro Health Monitor
JamesGycle –
zofran generic: generic for zofran – Nausea Care US
JamesGycle –
ondansetron: ondansetron medication – zofran dosage
Jeffreytoumn –
https://nauseacareus.shop/# Nausea Care US
JamesGycle –
Gastro Health Monitor: Gastro Health Monitor – omeprazole medication
Conradwaf –
ondansetron zofran: zofran medication – zofran dosage
JamesGycle –
tizanidine hcl: Spasm Relief Protocols – muscle relaxer tizanidine
JamesGycle –
robaxin medication: Spasm Relief Protocols – muscle relaxer medication
Jeffreytoumn –
http://spasmreliefprotocols.com/# robaxin
JamesGycle –
buy zofran online: zofran generic – Nausea Care US
JamesGycle –
antispasmodic medication: over the counter muscle relaxers that work – methocarbamol medication
Conradwaf –
omeprazole: buy prilosec – buy prilosec online
JamesGycle –
prilosec side effects: Gastro Health Monitor – prilosec omeprazole
JamesGycle –
best muscle relaxer: tizanidine hcl – muscle relaxant drugs
JamesGycle –
zofran otc: Nausea Care US – Nausea Care US
JamesGycle –
ondansetron otc: buy zofran online – Nausea Care US
Conradwaf –
Gastro Health Monitor: Gastro Health Monitor – buy prilosec online
JamesGycle –
methocarbamol robaxin: Spasm Relief Protocols – muscle relaxer medication
Jeffreytoumn –
http://gastrohealthmonitor.com/# omeprazole over the counter
JamesGycle –
robaxin medication: zanaflex medication – robaxin
Conradwaf –
prilosec dosage: prilosec generic – prilosec side effects
Jeffreytoumn –
http://nauseacareus.com/# Nausea Care US
Jeffreytoumn –
http://nauseacareus.com/# Nausea Care US
Conradwaf –
Gastro Health Monitor: buy prilosec – Gastro Health Monitor
Jeffreytoumn –
https://spasmreliefprotocols.com/# tizanidine medication
Conradwaf –
zofran dosage: generic for zofran – Nausea Care US
Jeffreytoumn –
http://gastrohealthmonitor.com/# generic prilosec
Conradwaf –
Nausea Care US: Nausea Care US – Nausea Care US
Jeffreytoumn –
https://spasmreliefprotocols.shop/# muscle relaxant drugs
RichardPlurn –
https://spasmreliefprotocols.shop/# tizanidine medication
Conradwaf –
otc muscle relaxer: Spasm Relief Protocols – robaxin
Jeffreytoumn –
https://gastrohealthmonitor.shop/# omeprazole otc
WilliamRaf –
buying prescription drugs in mexico: mexico city pharmacy – BajaMed Direct
RandyAmigo –
http://bajameddirect.com/# pharmacy in mexico city
Vaughndenty –
https://indogenericexport.com/# indian pharmacies safe
RandyAmigo –
https://indogenericexport.com/# tizanidine hydrochloride
WilliamRaf –
india pharmacy: Indo-Generic Export – best online pharmacy india
Vaughndenty –
https://indogenericexport.com/# best india pharmacy
RandyAmigo –
https://indogenericexport.shop/# tizanidine generic
WilliamRaf –
US Meds Outlet: pharmacy discount coupons – legal canadian pharmacy online
Vaughndenty –
https://indogenericexport.com/# buy prescription drugs from india
RandyAmigo –
http://usmedsoutlet.com/# cialis canada online pharmacy
WilliamRaf –
indian pharmacies safe: Indo-Generic Export – indian pharmacies safe
RandyAmigo –
http://usmedsoutlet.com/# US Meds Outlet
MatthewWix –
buy methocarbamol without prescription: antispasmodic medication – best muscle relaxer
WilliamRaf –
indian pharmacy paypal: Indo-Generic Export – best india pharmacy
RandyAmigo –
https://bajameddirect.shop/# BajaMed Direct
Harryduess –
best online pharmacy india: Indo-Generic Export – india pharmacy mail order
WilliamRaf –
BajaMed Direct: mexican pharmacy prices – online pharmacies
RandyAmigo –
https://usmedsoutlet.shop/# discount pharmacy
Harryduess –
india pharmacy mail order: Indo-Generic Export – india pharmacy mail order
WilliamRaf –
BajaMed Direct: BajaMed Direct – best mexican pharmacy
RandyAmigo –
https://bajameddirect.shop/# BajaMed Direct
WilliamRaf –
BajaMed Direct: buying prescriptions in mexico – BajaMed Direct
RandyAmigo –
http://bajameddirect.com/# pharmacia mexico
Harryduess –
canadian pharmacy 1 internet online drugstore: US Meds Outlet – canada drugs online review
WilliamRaf –
world pharmacy india: Indo-Generic Export – cheapest online pharmacy india
RandyAmigo –
https://bajameddirect.com/# order medicine from mexico
WilliamRaf –
discount pharmacy online: best canadian pharmacy for viagra – best european online pharmacy
WilliamRaf –
reputable indian online pharmacy: Indo-Generic Export – best india pharmacy
WilliamRaf –
reputable indian online pharmacy: online shopping pharmacy india – india pharmacy mail order
whxftoahz –
Every Fish has a random prize displayed at the bottom. It can significantly boost the overall payout at any moment. Whenever the Angler icon lands, it catches every visible fish and collects prizes. If you’re looking to try the demo slot Bigger Bass version first, it’s a great way to see how bonus features and prize mechanics unfold without the pressure of real-money play. Playing Big Bass Bonanza in the UK is easy and exciting, whether you’re a beginner or a seasoned player. Knowing how the money game works and how to place your bets will help you enjoy the full experience and maximise your chances of winning. This section explains everything you need to get started with this popular online slot! When you spin the reels in Bigger Bass Bonanza, you’ll have the chance to accumulate money by landing the Fish Money symbol. This money can then be claimed within the Free Spins bonus game.
https://www.xtremepumps.com/mr-pacho-casino-review-an-exciting-experience-for-australian-players/
Should you start climbing to the giant’s lair in the sky? Let’s have a look in this Jack and the Beanstalk slot review and don’t forget to also try the Jack and the Beanstalk free play demo! Previous It’s Time Money bags, wonderful hens, and fantastic harps try taking walks wilds, and all three walk you to definitely reel in order to kept once crystal ball slot free spins causing a good respin. The winning combinations that has an untamed along with spend 3x the fresh paytable worth. The fresh Jack and the Beanstalk on line slot video game of NetEnt is actually a slot machine having five reels, around three rows, and you can 20 repaired spend outlines. Signs are to experience cards signs from ten so you can A great while others of your emails regarding the story book.
WilliamRaf –
online pharmacy delivery usa: US Meds Outlet – US Meds Outlet
ryvxfukyl –
Gates of Olympus has a very high volatility level. This slot title is a top choice for anyone who’s willing to risk more for the potential of bigger returns. And if you have a deep appreciation of Greek Mythology, there are even more reasons for you to play! Tonton ribuan judul film Hollywood, Bollywood, Indonesia, drama Korea, dan serial TV populer lainnya. Today, with GamblingNews and Casinolytics’ backed ceremony, Pragmatic Play has been able to distinguish itself as the creator of the most streamed slot game in the industry, proving itself as a top hit among players and slot enthusiasts. Sebastian Khalighy, CEO & Co-founder at Casinolytics, has hailed Pragmatic Play for achieving this milestone and congratulated the team behind the game. Khalighy commended Pragmatic Play for their efforts and said:
https://vancouvercanadahomes.com/?p=330158
The Bonus Buy option for Gates of Olympus allows players to pay a fixed amount (typically 100x the bet) to instantly access the free spins feature. However, this option is not available in the United Kingdom due to UK Gambling Commission (UKGC) regulations. In the UK, the Bonus Buy feature was banned in 2019 to promote responsible gambling, as it can lead to rapid, high-cost spending that increases the risk of financial harm. Like all games from Playtech, Liz Sherman and Big Red himself land on the five reels and 20 paylines. You may have noticed that we stated the house is guaranteed to make a profit in the long run, which means the same is generated in payouts. Our review experts will also look at the welcome bonus, the New Jersey Division of Gaming Enforcement released the second quarter report for casinos in New Jersey. Gates of olympus on different devices you can either play in demo mode, laptop or a tablet that supports good internet connection and your ready to enjoy as if playing in a real land based casino premises where you will experience almost the same level of fun and entertainment.
WilliamRaf –
US Meds Outlet: us online pharmacy – US Meds Outlet
Vaughndenty –
https://indogenericexport.shop/# Online medicine order
WilliamRaf –
Online medicine order: Indo-Generic Export – Online medicine order
Vaughndenty –
https://indogenericexport.com/# mail order pharmacy india
WilliamRaf –
BajaMed Direct: BajaMed Direct – mexipharmacy reviews
WilliamRaf –
US Meds Outlet: online pharmacy pain relief – US Meds Outlet
Vaughndenty –
https://indogenericexport.com/# top online pharmacy india
WilliamRaf –
reputable indian pharmacies: Indo-Generic Export – Online medicine order
WilliamRaf –
pharmacy website india: Indo-Generic Export – india online pharmacy
Vaughndenty –
https://bajameddirect.com/# mexican drug stores
qnsoxlglm –
Conecte-se conosco Conecte-se conosco A volatilidade alta, torna o Gates of Olympus 1000 perfeito para aplicar as nossas estratégias preferidas para as slot machines. As nossas estratégias para slots visam a maior volatilidade possível. Para começar a jogar em um casino online em Portugal, é fundamental primeiro escolher um operador legal e autorizado pela SRIJ, garantindo segurança e proteção dos seus dados. Depois, crie sua conta, confirme sua identidade e configure limites de depósito para jogar de forma responsável. Explore as ofertas de bónus de boas-vindas, freespins e promoções disponíveis, e escolha um método de pagamento seguro, como MB Way, Multibanco, cartões ou e-wallets, para depósitos rápidos. Este slot tem uma RTP de 96,50% e alta volatilidade. Além disso, ela tem muitas semelhanças com o famoso jogo Sweet Bonanza, outro produto da Pragmatic Play. Portanto, se você já jogou este jogo antes, não terá muita dificuldade para se acostumar com o Gates of Olympus.
https://saudevivere.com.br/?p=4989
Em breve, será redirecionado para o site do casino. Aguarde. Se utilizar algum software de bloqueio de anúncios, verifique as definições. Se preferes experimentar antes de ler a minha análise, podes jogar já a slot Gate of Olympus e continuar a ler depois. Podes jogar sem risco com a versão demo que partilho contigo. Esta é a forma ideal de dominares a dinâmica antes de apostares a dinheiro. Explora a Gates of Olympus grátis e sente o poder divino dos multiplicadores de até 500× que podem transformar uma rodada normal num relâmpago de vitórias. This website is using a security service to protect itself from online attacks. The action you just performed triggered the security solution. There are several actions that could trigger this block including submitting a certain word or phrase, a SQL command or malformed data.
WilliamRaf –
US Meds Outlet: top mail order pharmacies – US Meds Outlet
Vaughndenty –
https://indogenericexport.shop/# Online medicine home delivery
WilliamRaf –
world pharmacy india: Indo-Generic Export – Online medicine home delivery
WilliamRaf –
BajaMed Direct: BajaMed Direct – pharmacies in mexico that ship to the us
Vaughndenty –
http://bajameddirect.com/# BajaMed Direct
WilliamRaf –
п»їlegitimate online pharmacies india: india online pharmacy – india online pharmacy
WilliamRaf –
BajaMed Direct: BajaMed Direct – BajaMed Direct
Vaughndenty –
http://bajameddirect.com/# mexican medicine store
WilliamRaf –
US Meds Outlet: safe canadian pharmacy – US Meds Outlet
Vaughndenty –
https://indogenericexport.shop/# top 10 online pharmacy in india
WilliamRaf –
mail order pharmacy india: india online pharmacy – mail order pharmacy india
feecrhhkz –
You can try Aloha! Cluster Pays for free right here and test the features and find out if you enjoy this theme before deciding if you want to play it on a real money version. The name says a lot about one of this game’s most significant features. As previously, mentioned this slot machine does not have pay-lines instead the player needs to collect clusters to win. To form a cluster all symbols that are the same that are adjacent to each other count, regardless of if they are horizontally or vertically adjacent. Players need nine or more symbols for a cluster to award a win. Aloha! Cluster Pays is an absolute feast for the eyes and senses. The palm trees, coconuts, beaches and seashells all add to the laid-back atmosphere. You can almost feel the slight ocean breeze and taste the pina colada.
https://layan.ae/resena-balloon-de-smartsoft-en-casinos-online-para-jugadores-argentinos/
After the first several deposit bonuss and they have bled you dry the promotions also dry up, you need to acknowledge that you are over 21 years of age. Play Well of Wilds Megaways on Android now to win feature prizes and jackpots on the go or at home, aloha cluster pays demo mode filled in the previous information with accuracy. We aim to give you the information you need about how and where to claim the latest free bingo, we always test how the support team treats its users. Yes, it is. You can play the game at no cost in most New Zealand casinos by launching it in demo mode. We can say with great confidence that Aloha Christmas is easily one of the hottest Christmas slots this holiday season. In fact, ever since NetEnt’s massive hit Aloha! Cluster Pays about 5 years ago, the public was eager for another festive slot by this iGaming provider. Well, it is safe to say that NetEnt definitely delivered. Released exactly one year ago, Aloha! Christmas can be easily referred to as the pinnacle of the Christmas-inspired slot games.
WilliamRaf –
reputable indian pharmacies: Indo-Generic Export – indian pharmacy online
Glennorgag –
https://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
pharmacy com: mail order pharmacy india – Smart GenRx USA
Glennorgag –
https://smartgenrxusa.com/# reputable online pharmacy reddit
LinwoodCix –
Smart GenRx USA: cheapest pharmacy for prescriptions without insurance – www pharmacyonline
Glennorgag –
https://sertralineusa.shop/# zoloft without rx
LinwoodCix –
Neuro Relief USA: Neuro Relief USA – Neuro Relief USA
Glennorgag –
https://smartgenrxusa.com/# Smart GenRx USA
Glennorgag –
https://smartgenrxusa.com/# Smart GenRx USA
LinwoodCix –
Smart GenRx USA: canadian pharmacy viagra reviews – Smart GenRx USA
Glennorgag –
http://sertralineusa.com/# buy zoloft
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – Smart GenRx USA
Glennorgag –
https://sertralineusa.com/# zoloft generic
LinwoodCix –
generic stromectol: Iver Therapeutics – Iver Therapeutics
Glennorgag –
http://ivertherapeutics.com/# stromectol 3mg
LinwoodCix –
Iver Therapeutics: stromectol medication – ivermectin generic
LeonardAnymn –
Smart GenRx USA [url=http://smartgenrxusa.com/#]online pharmacy without scripts[/url] canadian online pharmacy
Glennorgag –
https://smartgenrxusa.shop/# Smart GenRx USA
LinwoodCix –
generic zoloft: zoloft without rx – zoloft buy
Glennorgag –
https://smartgenrxusa.shop/# Smart GenRx USA
LinwoodCix –
med pharmacy: trustworthy canadian pharmacy – canadian pharmacy in canada
LeonardAnymn –
ivermectin oral solution [url=http://ivertherapeutics.com/#]stromectol price in india[/url] ivermectin for humans
Glennorgag –
https://smartgenrxusa.com/# Smart GenRx USA
LinwoodCix –
Iver Therapeutics: ivermectin tablets – Iver Therapeutics
Glennorgag –
http://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
reputable canadian pharmacy: Smart GenRx USA – Smart GenRx USA
Glennorgag –
https://sertralineusa.shop/# generic zoloft
LeonardAnymn –
sertraline zoloft [url=https://sertralineusa.com/#]zoloft medication[/url] generic for zoloft
LinwoodCix –
canadian pharmacy 365: pharmacy wholesalers canada – cialis canada online pharmacy
Glennorgag –
https://sertralineusa.shop/# zoloft without rx
LinwoodCix –
zoloft without rx: zoloft cheap – buy zoloft
Glennorgag –
https://neuroreliefusa.shop/# Neuro Relief USA
LinwoodCix –
Iver Therapeutics: Iver Therapeutics – Iver Therapeutics
LeonardAnymn –
Iver Therapeutics [url=https://ivertherapeutics.shop/#]Iver Therapeutics[/url] ivermectin rx
olrlwfywo –
Gates of Olympus 1000 er fuldt optimeret til både desktop og mobile enheder. Animationerne er silkebløde, indlæsningstiderne hurtige, og spillet kører problemfrit uanset skærmstørrelse eller operativsystem. Vi byder dig velkommen til et kongerige af casino spil på 888 casino dk. Nyd at spille med Zeus, med guldbelagte søjler og en marmortrappe indbygget i skyformationer, der fører op til slottet på bjerget Olympen. Nyd den utrolige spænding, mens du flyver hen over himlen i jagten på enorme pengegevinster. Men bare rolig, i vores casino kan du altid spille ansvarligt. Læs hele vores anmeldelse af Gates of Olympus, inden du begynder at spille på pc, Mac eller mobil. tempesta su PC, Mac o dispositivo mobile. En entusiastisk spiller, Søren, 35 år, deler sin oplevelse med at spille Gates of Olympus online i danske casinos: “Jeg har været skeptisk over for at spille casino online, men efter at have prøvet Gates of Olympus i et dansk casino, er jeg begejstret! Spillet er så underholdende og det var super let at navigere på siden. Jeg følte mig meget tryg og sikker hele tiden. Jeg kan varmt anbefale at prøve dette spil ud, hvis du er interesseret i at spille casino online.”
https://consultmylife.com/2026/02/09/review-af-nv-casino-et-spil-paradis-for-danske-spillere/
Looking through this article reminds me of my previous roommate! Sweet Bonanza 1000, en innovativ opdatering fra Pragmatic Play, har revolutioneret online slotoplevelsen med introduktionen af “Super Gratis Spins”. Denne opgraderede version af det populære slotspil Sweet Bonanza tilbyder en ny dimension til gratis spins-funktionen, som adskiller sig markant fra de traditionelle gratis spins i tidligere versioner. Når det kommer til gamblingverdenen, er der ofte to populære muligheder: traditionelle automatspil – de klassiske spilleautomater, der findes på casinoer – og online spilleautomater, som du kan spille derhjemme eller på farten. Hver af dem har sin egen unikke charme og appel, der passer til forskellige præferencer og spillestile. Lad os dykke ned i 18+ | Kun nye spillere. | Regler og vilkår gælder. | Spil ansvarligt. | Selvudeluk via ROFUS.nu | Kontakt Spillemyndighedens hjælpelinje på StopSpillet.dk | Indbetal præcis 100 kr. omsæt 500 kr. og få 50 freespins | Omsætning på x5 er gældende på alle spilleautomater | Freespins er til spillet Gold Blitz | Freespins har en værdi på 2 kr. per spin | Du har 14 dage til at aktivere tilbuddet under “mine tilbud”.
Glennorgag –
https://sertralineusa.com/# zoloft no prescription
LinwoodCix –
Neuro Relief USA: neurontin buy from canada – neurontin tablets
Glennorgag –
https://smartgenrxusa.shop/# Smart GenRx USA
LinwoodCix –
Iver Therapeutics: Iver Therapeutics – Iver Therapeutics
LeonardAnymn –
neurontin prescription cost [url=https://neuroreliefusa.shop/#]neurontin generic south africa[/url] neurontin 200 mg capsules
Glennorgag –
https://sertralineusa.shop/# generic for zoloft
LinwoodCix –
ivermectin for humans: Iver Therapeutics – Iver Therapeutics
Glennorgag –
https://sertralineusa.com/# sertraline
LinwoodCix –
Iver Therapeutics: stromectol drug – Iver Therapeutics
Glennorgag –
http://sertralineusa.com/# generic zoloft
LinwoodCix –
ez pharmacy: canadian pharmacy reviews – rx pharmacy online
LeonardAnymn –
sertraline generic [url=http://sertralineusa.com/#]zoloft without rx[/url] zoloft pill
LinwoodCix –
express scripts com pharmacies: legit online pharmacy – Smart GenRx USA
Glennorgag –
http://ivertherapeutics.com/# Iver Therapeutics
syotrjfxp –
The multipliers themselves are nothing new; between 1 and 5 random multipliers will be added to the board before each spin takes place, but after all bets have been made. However, after this point the player is given the option to buy 1, 2 or 3 extra multipliers to be added to the board. It means you can take your prize completely right into your wallet, low stakes roulette online for united kingdom players including Elvis Frog. One of the reasons is that the game has several exciting features such as wilds, 20 Super Stars. The second recommendation of the online poker report is, plenty of points from me. Best live roulette united kingdom the combination must be made of at least three of the same symbols, he went against Hellmuth and was not able to close the deal. Kelly was assumed to be the winning lotto ticket-holder and a guy apparently a friend congratulated him on his earnings via FB, roulette or blackjack. Hands with a higher value than Gongs, Deuces Wild.
https://hchc.online/archives/34802
As to whether the astronaut game is real or fake—well rest easy, 100HP Gaming is trying to deliver fair and good products. With different versions like astronaut game login pages and astronaut game apps, you’ll be playing in no time—no matter where you are! As to whether the astronaut game is real or fake—well rest easy, 100HP Gaming is trying to deliver fair and good products. With different versions like astronaut game login pages and astronaut game apps, you’ll be playing in no time—no matter where you are! How to play an astronaut game mobile like a pro? Whether to try the astronaut game demo just to get a handle, or jump right in as a table dabbler and seeker of great payouts: not difficult for players from Pakistan who find themselves in this astronaut betting game. After I grew accustomed to the easy controls, immersive space-themed visuals and certified algorithm-based rounds, the astronaut game in Pakistan became one of my personal all-time favorite online astronaut the games.
LinwoodCix –
neurontin price australia: price of neurontin – Neuro Relief USA
Glennorgag –
https://neuroreliefusa.shop/# Neuro Relief USA
LeonardAnymn –
sertraline zoloft [url=http://sertralineusa.com/#]zoloft without rx[/url] zoloft tablet
LinwoodCix –
zoloft tablet: zoloft generic – order zoloft
Glennorgag –
https://neuroreliefusa.com/# Neuro Relief USA
LinwoodCix –
Neuro Relief USA: neurontin 300mg – neurontin pfizer
Glennorgag –
http://ivertherapeutics.com/# ivermectin cream 5%
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – Smart GenRx USA
Glennorgag –
https://neuroreliefusa.shop/# Neuro Relief USA
LeonardAnymn –
neurontin rx [url=http://neuroreliefusa.com/#]Neuro Relief USA[/url] Neuro Relief USA
LinwoodCix –
neurontin 600 mg cost: Neuro Relief USA – neurontin 800 mg tablets best price
LinwoodCix –
sertraline zoloft: zoloft medication – sertraline zoloft
Glennorgag –
https://smartgenrxusa.shop/# online pharmacy birth control pills
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – cheapest pharmacy to fill prescriptions without insurance
LeonardAnymn –
no script pharmacy [url=https://smartgenrxusa.com/#]Smart GenRx USA[/url] pharmacy order online
LinwoodCix –
Iver Therapeutics: ivermectin 12 mg – Iver Therapeutics
LinwoodCix –
sertraline: zoloft pill – buy zoloft
Glennorgag –
https://ivertherapeutics.shop/# Iver Therapeutics
LinwoodCix –
mail order pharmacy: cost less pharmacy – mail order pharmacy
Tracydow –
http://neuroreliefusa.com/# neurontin brand name 800mg best price
LeonardAnymn –
best value pharmacy [url=https://smartgenrxusa.shop/#]Smart GenRx USA[/url] Smart GenRx USA
LinwoodCix –
buy ivermectin canada: Iver Therapeutics – Iver Therapeutics
Tracydow –
https://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
Neuro Relief USA: neurontin cost uk – Neuro Relief USA
Tracydow –
http://ivertherapeutics.com/# cost of ivermectin medicine
Glennorgag –
https://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
ivermectin 500ml: Iver Therapeutics – Iver Therapeutics
Tracydow –
http://neuroreliefusa.com/# Neuro Relief USA
LeonardAnymn –
buy zoloft [url=https://sertralineusa.com/#]sertraline generic[/url] buy zoloft
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – pharmacy coupons
Tracydow –
https://sertralineusa.com/# sertraline zoloft
LinwoodCix –
sertraline: zoloft no prescription – sertraline zoloft
Tracydow –
https://smartgenrxusa.shop/# canadian pharmacy discount coupon
Glennorgag –
https://neuroreliefusa.com/# Neuro Relief USA
LinwoodCix –
zoloft pill: generic for zoloft – sertraline
LeonardAnymn –
sertraline generic [url=https://sertralineusa.com/#]zoloft generic[/url] zoloft tablet
LinwoodCix –
Neuro Relief USA: Neuro Relief USA – neurontin 400
Tracydow –
https://neuroreliefusa.com/# neurontin singapore
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – indian pharmacy
Larrybum –
Smart GenRx USA: pharmacy prices – sure save pharmacy
Glennorgag –
http://neuroreliefusa.com/# Neuro Relief USA
LinwoodCix –
Neuro Relief USA: Neuro Relief USA – Neuro Relief USA
tbyjamtom –
Die Anjouan Gaming Authority reguliert alle Aspekte des Casino-Betriebs. Dazu gehören Spielerschutz, finanzielle Sicherheit und operative Transparenz. Thüringer Spieler finden hier eine Übersicht von Anlaufstellen, wo sie sich Informationen und Hilfe zum Thema Glücksspiel, Spielen mit Verantwortung und problematischem Spielverhalten holen können: Die zertifizierte Referenznummer wird im \”MENU\” unter \”GEWINNE & INFO\” angezeigt. Mr Green überzeugt als führende Online Spielothek mit einer umfangreichen Spielauswahl, attraktiven Boni, einer benutzerfreundlichen mobilen App und einem starken Engagement für Sicherheit und verantwortungsbewusstes Spielen. Die Plattform bietet ein erstklassiges Spielerlebnis mit zahlreichen Auszeichnungen als Beleg für ihre Qualität, besitzt die deutsche Lizenz der GGL, womit höchster Spielerschutz garantiert ist.
https://lawvision.sa/111/1win-casino-game-review-spannung-und-gewinnchancen-fur-deutsche-spieler/
Spät nachts, auf der LOREA sitzt man bei Kerzenlicht und einem Glas Rioja im Mittelcockpit, die MEDITERRANEA liegt weniger als eine Schiffslänge vor dem Bug der LOREA, rattert ein Außenborder aus der Finsternis heran. Die junge Hübsche versucht eine Entschuldigung auf Englisch. Ist in Manchester daheim. Der stämmige blonde Skipper aus Deutschland kontert den Hinweis, dass sein Schiff nicht sicher liege und auf Drift sei, mit dem Satz: Nun sei mal nicht so deutsch… Sie hätten das Horn schon gehört, aber niemand winken gesehen. 0.916.026.81 Europäische Gemeinsch Durth, Werner (1998)Utopie der Gemeinschaft: Überlegungen zur Neugestaltung deutscher Städte 1900-1950. In: Moderne Architektur in Deutschland 1900 bis 2000: Macht und Monument; Ausstellung im Deutschen ArchitekturmuseumBuchkapitel, Bibliographie
LeonardAnymn –
rx pharmacy no prescription [url=https://smartgenrxusa.com/#]canadian pharmacy generic viagra[/url] Smart GenRx USA
Tracydow –
https://smartgenrxusa.com/# your pharmacy online
Larrybum –
Smart GenRx USA: canadian pharmacy reviews – low cost online pharmacy
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – Smart GenRx USA
Tracydow –
http://sertralineusa.com/# zoloft cheap
LinwoodCix –
buy zoloft: zoloft no prescription – buy zoloft
Glennorgag –
https://ivertherapeutics.shop/# ivermectin generic cream
Tracydow –
https://smartgenrxusa.shop/# mexican pharmacy online
Larrybum –
buy zoloft: generic for zoloft – sertraline generic
LinwoodCix –
Neuro Relief USA: neurontin pills for sale – Neuro Relief USA
LeonardAnymn –
Smart GenRx USA [url=http://smartgenrxusa.com/#]canadian pharmacy viagra[/url] online pharmacy india
Larrybum –
zoloft without dr prescription: zoloft without dr prescription – zoloft pill
LinwoodCix –
sertraline: zoloft tablet – buy zoloft
Tracydow –
https://smartgenrxusa.shop/# Smart GenRx USA
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – Smart GenRx USA
Tracydow –
https://sertralineusa.com/# zoloft pill
Larrybum –
Neuro Relief USA: Neuro Relief USA – purchase neurontin canada
LeonardAnymn –
Smart GenRx USA [url=https://smartgenrxusa.com/#]reputable online pharmacy reddit[/url] online pharmacy indonesia
Tracydow –
https://neuroreliefusa.com/# neurontin 300 mg coupon
LinwoodCix –
zoloft without dr prescription: zoloft tablet – generic zoloft
Larrybum –
where can i buy neurontin from canada: Neuro Relief USA – Neuro Relief USA
Tracydow –
https://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
Iver Therapeutics: ivermectin 5 mg price – stromectol where to buy
Tracydow –
http://neuroreliefusa.com/# Neuro Relief USA
LinwoodCix –
generic for zoloft: generic for zoloft – zoloft pill
Larrybum –
Smart GenRx USA: Smart GenRx USA – Smart GenRx USA
LeonardAnymn –
can i buy neurontin over the counter [url=https://neuroreliefusa.shop/#]Neuro Relief USA[/url] Neuro Relief USA
Tracydow –
https://neuroreliefusa.com/# buying neurontin online
LinwoodCix –
stromectol coronavirus: Iver Therapeutics – stromectol price
Tracydow –
https://smartgenrxusa.shop/# pharmacy without prescription
Larrybum –
buy ivermectin uk: ivermectin where to buy for humans – ivermectin tablets uk
LinwoodCix –
Neuro Relief USA: neurontin capsules 100mg – neurontin 200
Tracydow –
https://sertralineusa.shop/# buy zoloft
Larrybum –
order zoloft: generic zoloft – zoloft cheap
LinwoodCix –
brand neurontin 100 mg canada: Neuro Relief USA – Neuro Relief USA
Tracydow –
https://neuroreliefusa.com/# Neuro Relief USA
LinwoodCix –
zoloft medication: zoloft buy – sertraline generic
Tracydow –
https://neuroreliefusa.shop/# neurontin mexico
Glennorgag –
http://smartgenrxusa.com/# Smart GenRx USA
Larrybum –
Neuro Relief USA: Neuro Relief USA – neurontin 800 mg tablets
Tracydow –
http://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
Sertraline USA: zoloft no prescription – order zoloft
LeonardAnymn –
Iver Therapeutics [url=https://ivertherapeutics.com/#]Iver Therapeutics[/url] Iver Therapeutics
Tracydow –
https://ivertherapeutics.com/# where to buy stromectol online
LinwoodCix –
buy stromectol: Iver Therapeutics – Iver Therapeutics
pphgezqwk –
A Mostbet oferece métodos de pagamento convenientes para os parceiros, como Visa, Mastercard, Skrill, Neteller, Qiwi e Paxum. Para participar no programa, basta registar-se. No formulário, precisa de indicar o seu e-mail, palavra-passe e login do Telegram. As informações sobre o programa de afiliados estão numa secção separada no website da Mostbet. Venha fazer parte desta equipa! Algumas pessoas preferem usar nomes engraçados e divertidos para sua guilda em vez de algo que exale poder. Então, se está procurando nomes com conteúdo voltado mais para diversão, aqui temos algumas sugestões: Lançamos esta iniciativa com o objetivo de criar um sistema global de autoexclusão, que permitirá que os jogadores vulneráveis bloqueiem o seu acesso a todas as oportunidades de jogo online.
https://smartwebmedia.rs/ivibet-review-do-jogo-de-cassino-online-para-jogadores-brasileiros/
Português, Alemão, Checo, Chinês simplificado, Chinês tradicional, Coreano, Espanhol, Francês, Holandês, Inglês, Italiano, Japonês, Polonês, Russo, Sueco, Turco Português, Alemão, Chinês simplificado, Chinês tradicional, Coreano, Espanhol, Francês, Hindi, Indonésio, Inglês, Italiano, Japonês, Polonês, Russo, Tailandês, Turco, Ucraniano, Vietnamita, Árabe chato e cheio de anúncios Bug fixes and performance improvements. Bug fixes and performance improvements. Blacksmith Lab Idle Sim, a Mostbet disponibiliza aplicações móveis completas para dispositivos Android e iOS. Pode descarregar a aplicação Android diretamente do site oficial da Mostbet, enquanto a versão para iOS está disponível na Apple App Store. As aplicações oferecem acesso a todas as funcionalidades do site, incluindo apostas desportivas, jogos de casino e gestão de conta.
Glennorgag –
http://neuroreliefusa.com/# neurontin cap 300mg price
Tracydow –
https://sertralineusa.shop/# zoloft without dr prescription
LinwoodCix –
canadian pharmacy cialis 20mg: canadian pharmacy 365 – Smart GenRx USA
Larrybum –
Smart GenRx USA: Smart GenRx USA – canadian pharmacy world
Tracydow –
http://ivertherapeutics.com/# generic ivermectin
LeonardAnymn –
purchase neurontin canada [url=http://neuroreliefusa.com/#]order neurontin[/url] Neuro Relief USA
LinwoodCix –
zoloft without rx: zoloft without dr prescription – zoloft no prescription
Larrybum –
Neuro Relief USA: Neuro Relief USA – Neuro Relief USA
Tracydow –
https://smartgenrxusa.com/# online pharmacy no prescription
Glennorgag –
https://sertralineusa.com/# zoloft tablet
LinwoodCix –
Smart GenRx USA: 77 canadian pharmacy – Smart GenRx USA
Tracydow –
https://smartgenrxusa.com/# modafinil online pharmacy
Larrybum –
Iver Therapeutics: order stromectol online – Iver Therapeutics
LinwoodCix –
neurontin 300mg caps: neurontin 800 mg capsules – Neuro Relief USA
Tracydow –
https://ivertherapeutics.shop/# buy ivermectin uk
LeonardAnymn –
Iver Therapeutics [url=http://ivertherapeutics.com/#]Iver Therapeutics[/url] Iver Therapeutics
LinwoodCix –
legal online pharmacy: online pharmacy no prescription – Smart GenRx USA
Larrybum –
zoloft generic: zoloft medication – Sertraline USA
Glennorgag –
http://neuroreliefusa.com/# neurontin 100 mg tablets
Tracydow –
https://sertralineusa.com/# zoloft pill
LinwoodCix –
Iver Therapeutics: Iver Therapeutics – ivermectin buy
Tracydow –
http://smartgenrxusa.com/# rxpharmacycoupons
Larrybum –
ivermectin uk coronavirus: Iver Therapeutics – Iver Therapeutics
LinwoodCix –
stromectol 15 mg: ivermectin 3mg pill – ivermectin 3mg pill
Tracydow –
http://ivertherapeutics.com/# ivermectin uk coronavirus
LeonardAnymn –
zoloft buy [url=https://sertralineusa.com/#]generic for zoloft[/url] zoloft medication
Glennorgag –
https://ivertherapeutics.shop/# stromectol covid 19
Larrybum –
Neuro Relief USA: Neuro Relief USA – Neuro Relief USA
Tracydow –
https://ivertherapeutics.shop/# Iver Therapeutics
LinwoodCix –
walmart pharmacy online: Smart GenRx USA – Smart GenRx USA
Tracydow –
https://ivertherapeutics.shop/# Iver Therapeutics
LinwoodCix –
Neuro Relief USA: Neuro Relief USA – Neuro Relief USA
Larrybum –
Sertraline USA: zoloft generic – zoloft no prescription
Glennorgag –
http://smartgenrxusa.com/# Smart GenRx USA
LeonardAnymn –
zoloft without rx [url=http://sertralineusa.com/#]Sertraline USA[/url] zoloft without rx
Tracydow –
https://smartgenrxusa.com/# Smart GenRx USA
LinwoodCix –
sertraline zoloft: sertraline zoloft – zoloft without rx
Larrybum –
zoloft medication: zoloft medication – zoloft buy
Tracydow –
http://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
Iver Therapeutics: Iver Therapeutics – Iver Therapeutics
Tracydow –
https://ivertherapeutics.shop/# Iver Therapeutics
Glennorgag –
http://neuroreliefusa.com/# Neuro Relief USA
Larrybum –
canadian world pharmacy: Smart GenRx USA – Smart GenRx USA
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – Smart GenRx USA
LeonardAnymn –
zoloft buy [url=https://sertralineusa.shop/#]zoloft pill[/url] sertraline zoloft
Tracydow –
https://neuroreliefusa.shop/# Neuro Relief USA
Larrybum –
Smart GenRx USA: Smart GenRx USA – escrow pharmacy online
LinwoodCix –
Sertraline USA: zoloft medication – zoloft generic
Tracydow –
https://sertralineusa.shop/# sertraline zoloft
Glennorgag –
https://smartgenrxusa.shop/# Smart GenRx USA
LinwoodCix –
Iver Therapeutics: stromectol pills – Iver Therapeutics
Tracydow –
http://ivertherapeutics.com/# Iver Therapeutics
Larrybum –
ivermectin ebay: Iver Therapeutics – ivermectin 2ml
LeonardAnymn –
medical mall pharmacy [url=https://smartgenrxusa.shop/#]mexican online mail order pharmacy[/url] canadian pharmacy mall
Tracydow –
https://ivertherapeutics.com/# Iver Therapeutics
LinwoodCix –
Iver Therapeutics: Iver Therapeutics – Iver Therapeutics
Larrybum –
Neuro Relief USA: neurontin brand name in india – neurontin generic
Tracydow –
https://sertralineusa.shop/# zoloft pill
Glennorgag –
https://sertralineusa.com/# order zoloft
LinwoodCix –
neurontin 300 mg: neurontin buy from canada – neurontin 100mg tab
Tracydow –
https://sertralineusa.com/# zoloft without dr prescription
Larrybum –
canadian pharmacy prices: Smart GenRx USA – Smart GenRx USA
LinwoodCix –
Neuro Relief USA: Neuro Relief USA – Neuro Relief USA
LeonardAnymn –
Smart GenRx USA [url=http://smartgenrxusa.com/#]Smart GenRx USA[/url] pharmacy open near me
Tracydow –
https://smartgenrxusa.com/# Smart GenRx USA
LinwoodCix –
stromectol ivermectin buy: Iver Therapeutics – ivermectin lotion price
Larrybum –
Neuro Relief USA: neurontin 100mg tab – neurontin 300 mg capsule
Glennorgag –
https://sertralineusa.com/# Sertraline USA
Tracydow –
https://neuroreliefusa.shop/# Neuro Relief USA
LinwoodCix –
Iver Therapeutics: Iver Therapeutics – Iver Therapeutics
Larrybum –
Smart GenRx USA: Smart GenRx USA – Smart GenRx USA
Tracydow –
https://sertralineusa.com/# zoloft generic
LinwoodCix –
Neuro Relief USA: Neuro Relief USA – neurontin online
LeonardAnymn –
Smart GenRx USA [url=https://smartgenrxusa.com/#]Smart GenRx USA[/url] Smart GenRx USA
Tracydow –
https://smartgenrxusa.com/# Smart GenRx USA
Glennorgag –
http://ivertherapeutics.com/# where to buy stromectol
Larrybum –
Iver Therapeutics: ivermectin for sale – ivermectin price usa
LinwoodCix –
cheap neurontin: Neuro Relief USA – Neuro Relief USA
Tracydow –
https://neuroreliefusa.shop/# Neuro Relief USA
Larrybum –
Iver Therapeutics: stromectol for sale – Iver Therapeutics
LinwoodCix –
Smart GenRx USA: Smart GenRx USA – canada drugstore pharmacy rx
Tracydow –
https://neuroreliefusa.shop/# neurontin 600 mg coupon
LeonardAnymn –
buy zoloft [url=https://sertralineusa.com/#]zoloft pill[/url] zoloft without rx
Glennorgag –
https://sertralineusa.com/# zoloft pill
Tracydow –
https://neuroreliefusa.shop/# neurontin 600 mg coupon
LinwoodCix –
sertraline generic: buy zoloft – zoloft medication
Larrybum –
zoloft pill: generic for zoloft – buy zoloft
Tracydow –
https://sertralineusa.com/# generic zoloft
LinwoodCix –
ivermectin generic cream: Iver Therapeutics – Iver Therapeutics
Larrybum –
Iver Therapeutics: stromectol pill – Iver Therapeutics
Taylornar –
https://mymexicanpharmacy.com/# mexican pharmacy that ships to the us
MichaelPrump –
https://mymexicanpharmacy.com/# My Mexican Pharmacy
Edwardcrism –
CertiCanPharmacy: prescription drugs canada buy online – CertiCanPharmacy
LarryKeews –
online vet pharmacy [url=http://vetfreemeds.com/#]VetFree Meds[/url] pet meds for dogs
Taylornar –
http://certicanpharmacy.com/# CertiCanPharmacy
Edwardcrism –
dog medicine: VetFree Meds – online pet pharmacy
MichaelPrump –
https://vetfreemeds.com/# dog prescriptions online
Diegotwirm –
My Mexican Pharmacy: My Mexican Pharmacy – My Mexican Pharmacy
Taylornar –
http://certicanpharmacy.com/# canadadrugpharmacy com
Edwardcrism –
meds from mexico: medicine mexico – progreso, mexico pharmacy online
LarryKeews –
mexican pharmacies that ship to us [url=https://mymexicanpharmacy.shop/#]best mexican pharmacy[/url] mexico drug store online
Taylornar –
https://vetfreemeds.shop/# pet drugs online
Diegotwirm –
dog prescriptions online: vet pharmacy – dog prescriptions online
MichaelPrump –
https://mymexicanpharmacy.com/# My Mexican Pharmacy
Edwardcrism –
My Mexican Pharmacy: My Mexican Pharmacy – My Mexican Pharmacy
Taylornar –
http://mymexicanpharmacy.com/# the purple pharmacy mexico
MichaelPrump –
https://mymexicanpharmacy.com/# My Mexican Pharmacy
Diegotwirm –
vet pharmacy online: VetFree Meds – pet prescriptions online
LarryKeews –
dog prescriptions online [url=http://vetfreemeds.com/#]online vet pharmacy[/url] pet prescriptions online
Edwardcrism –
pet med: pet prescriptions online – dog prescriptions online
Taylornar –
http://certicanpharmacy.com/# CertiCanPharmacy
MichaelPrump –
http://certicanpharmacy.com/# online canadian pharmacy reviews
Edwardcrism –
certified canadian international pharmacy: safe reliable canadian pharmacy – canadian drug prices
Taylornar –
https://mymexicanpharmacy.shop/# mexican mail order pharmacy
MichaelPrump –
http://mymexicanpharmacy.com/# My Mexican Pharmacy
Diegotwirm –
pet rx: VetFree Meds – dog medicine
Edwardcrism –
canadian family pharmacy: canadian drug pharmacy – CertiCanPharmacy
LarryKeews –
CertiCanPharmacy [url=http://certicanpharmacy.com/#]CertiCanPharmacy[/url] CertiCanPharmacy
Taylornar –
https://certicanpharmacy.shop/# CertiCanPharmacy
MichaelPrump –
https://mymexicanpharmacy.shop/# mexico farmacia
Edwardcrism –
reputable canadian pharmacy: global pharmacy canada – CertiCanPharmacy
Taylornar –
https://vetfreemeds.shop/# online vet pharmacy
Diegotwirm –
mexican medicine: farmacias mexicanas – My Mexican Pharmacy
MichaelPrump –
https://mymexicanpharmacy.com/# My Mexican Pharmacy
Edwardcrism –
pet drugs online: pet pharmacy – pet pharmacy
Taylornar –
https://certicanpharmacy.com/# legit canadian online pharmacy
LarryKeews –
п»їdog medication online [url=https://vetfreemeds.shop/#]dog prescriptions online[/url] online pet pharmacy
MichaelPrump –
http://certicanpharmacy.com/# canadianpharmacymeds
Edwardcrism –
п»їdog medication online: VetFree Meds – pet med
Diegotwirm –
My Mexican Pharmacy: purple pharmacy mexico – My Mexican Pharmacy
Taylornar –
http://vetfreemeds.com/# pet meds online
MichaelPrump –
http://certicanpharmacy.com/# canadian pharmacy prices
stroitelnoe vodoponijenie_npSr –
водопонижение иглофильтрами [url=https://xn—77-eddkgagrc5cdhbap.xn--p1ai/]водопонижение иглофильтрами[/url] .
Edwardcrism –
pet meds official website: VetFree Meds – vet pharmacy
Taylornar –
http://certicanpharmacy.com/# canadian pharmacy ltd
Diegotwirm –
canadian pharmacy meds reviews: canada pharmacy reviews – trusted canadian pharmacy
MichaelPrump –
http://certicanpharmacy.com/# CertiCanPharmacy
Taylornar –
https://vetfreemeds.shop/# pet med
Edwardcrism –
mexican pharmacy: mexican pharmacies that ship to us – mexican pharmacies that ship to us
MichaelPrump –
https://certicanpharmacy.com/# CertiCanPharmacy
Diegotwirm –
canadian medications: the canadian pharmacy – canadian pharmacy india
Taylornar –
http://mymexicanpharmacy.com/# My Mexican Pharmacy
Edwardcrism –
online vet pharmacy: VetFree Meds – canada pet meds
MichaelPrump –
https://certicanpharmacy.com/# CertiCanPharmacy
LarryKeews –
canadian mail order pharmacy [url=https://certicanpharmacy.com/#]CertiCanPharmacy[/url] CertiCanPharmacy
Taylornar –
http://mymexicanpharmacy.com/# My Mexican Pharmacy
Edwardcrism –
reputable canadian online pharmacy: CertiCanPharmacy – CertiCanPharmacy
Diegotwirm –
canadian pharmacy: pharmacy canadian superstore – CertiCanPharmacy
MichaelPrump –
https://mymexicanpharmacy.shop/# mexico prescriptions
Taylornar –
https://certicanpharmacy.com/# CertiCanPharmacy
Edwardcrism –
cheapest pharmacy canada: canadapharmacyonline – best online canadian pharmacy
MichaelPrump –
http://certicanpharmacy.com/# legal to buy prescription drugs from canada
Diegotwirm –
pet prescriptions online: VetFree Meds – dog medication online
LarryKeews –
My Mexican Pharmacy [url=http://mymexicanpharmacy.com/#]pharmacies in mexico[/url] п»їmexican pharmacy
Edwardcrism –
pet meds official website: online pet pharmacy – pet med
MichaelPrump –
https://mymexicanpharmacy.shop/# mexican rx pharm
Taylornar –
http://vetfreemeds.com/# pet pharmacy online
Edwardcrism –
progreso mexico pharmacy online: My Mexican Pharmacy – My Mexican Pharmacy
Diegotwirm –
vet pharmacy online: dog prescriptions online – online pet pharmacy
MichaelPrump –
https://mymexicanpharmacy.shop/# My Mexican Pharmacy
Taylornar –
https://mymexicanpharmacy.com/# mexican online pharmacy
Edwardcrism –
mexican mail order pharmacy: My Mexican Pharmacy – My Mexican Pharmacy
Taylornar –
https://vetfreemeds.com/# best pet rx
Edwardcrism –
My Mexican Pharmacy: farmacia online usa – My Mexican Pharmacy
Diegotwirm –
CertiCanPharmacy: legitimate canadian mail order pharmacy – CertiCanPharmacy
MichaelPrump –
http://certicanpharmacy.com/# canadianpharmacyworld com
Taylornar –
http://mymexicanpharmacy.com/# My Mexican Pharmacy
Edwardcrism –
My Mexican Pharmacy: My Mexican Pharmacy – My Mexican Pharmacy
MichaelPrump –
http://vetfreemeds.com/# online pet pharmacy
Diegotwirm –
canadian pharmacy online ship to usa: CertiCanPharmacy – reliable canadian pharmacy
mostbet_hlEt –
mostbet вход через зеркало [url=http://mostbet61527.help/]http://mostbet61527.help/[/url]
Taylornar –
https://mymexicanpharmacy.com/# mexico online farmacia
Edwardcrism –
pet meds for dogs: VetFree Meds – pet prescriptions online
Jerold –
%random_anchor_text%
References:
securityheaders.com
MichaelPrump –
https://vetfreemeds.com/# п»їdog medication online
Taylornar –
http://vetfreemeds.com/# canada pet meds
Edwardcrism –
vet pharmacy: canada pet meds – online vet pharmacy
Diegotwirm –
pet pharmacy online: vet pharmacy online – pet prescriptions online
MichaelPrump –
https://vetfreemeds.shop/# dog medicine
Edwardcrism –
CertiCanPharmacy: my canadian pharmacy – CertiCanPharmacy
Taylornar –
https://certicanpharmacy.shop/# CertiCanPharmacy
Diegotwirm –
canada drug pharmacy: onlinecanadianpharmacy 24 – canadian pharmacy meds reviews
Edwardcrism –
pet pharmacy: pet prescriptions online – online vet pharmacy
Taylornar –
https://mymexicanpharmacy.com/# My Mexican Pharmacy
MichaelPrump –
https://vetfreemeds.com/# online pet pharmacy
Edwardcrism –
My Mexican Pharmacy: online pharmacies in mexico – farmacia mexicana en chicago
Taylornar –
https://mymexicanpharmacy.com/# My Mexican Pharmacy
Diegotwirm –
pet meds official website: dog prescriptions online – discount pet meds
LarryKeews –
My Mexican Pharmacy [url=https://mymexicanpharmacy.com/#]My Mexican Pharmacy[/url] My Mexican Pharmacy
MichaelPrump –
http://mymexicanpharmacy.com/# My Mexican Pharmacy
Edwardcrism –
My Mexican Pharmacy: My Mexican Pharmacy – My Mexican Pharmacy
Taylornar –
https://certicanpharmacy.shop/# legal canadian pharmacy online
MichaelPrump –
https://certicanpharmacy.shop/# CertiCanPharmacy
Edwardcrism –
dog medicine: pet meds online – best pet rx
Taylornar –
http://mymexicanpharmacy.com/# mexican drug store
Diegotwirm –
best online canadian pharmacy: best mail order pharmacy canada – canadian family pharmacy
MichaelPrump –
http://certicanpharmacy.com/# canadian pharmacies comparison
Edwardcrism –
pet pharmacy: VetFree Meds – pet meds for dogs
LarryKeews –
pet med [url=http://vetfreemeds.com/#]online pet pharmacy[/url] pet rx
Taylornar –
https://certicanpharmacy.shop/# CertiCanPharmacy
Diegotwirm –
canadian pharmacy 365: CertiCanPharmacy – CertiCanPharmacy
MichaelPrump –
http://certicanpharmacy.com/# buy drugs from canada
Edwardcrism –
pet rx: pet pharmacy online – dog medicine
Taylornar –
https://certicanpharmacy.shop/# reliable canadian pharmacy
Edwardcrism –
canadian pharmacy ratings: CertiCanPharmacy – canada cloud pharmacy
MichaelPrump –
http://mymexicanpharmacy.com/# п»їmexican pharmacy
Taylornar –
https://certicanpharmacy.shop/# CertiCanPharmacy
Diegotwirm –
pet meds online: VetFree Meds – pet med
Thomasbar –
http://ivermectinaccessusa.com/# Ivermectin Access USA
JeremyCow –
http://uspharmaindex.com/# canadian pharmacy reviews
Josephded –
US Pharma Index: US Pharma Index – US Pharma Index
Thomasbar –
http://ivermectinaccessusa.com/# Ivermectin Access USA
DavidMep –
ivermectin syrup: Ivermectin Access USA – Ivermectin Access USA
JeremyCow –
http://sildenafilpriceguide.com/# Cheap generic Viagra online
Josephded –
US Pharma Index: canada drugstore pharmacy rx – cheapest pharmacy for prescriptions without insurance
RandyHoody –
ivermectin purchase [url=https://ivermectinaccessusa.shop/#]Ivermectin Access USA[/url] Ivermectin Access USA
Thomasbar –
https://uspharmaindex.shop/# US Pharma Index
JeremyCow –
http://uspharmaindex.com/# us online pharmacy
Josephded –
bitcoin pharmacy online: no prescription needed canadian pharmacy – US Pharma Index
DavidMep –
online pharmacy delivery dubai: affordable pharmacy – best canadian pharmacy for cialis
Thomasbar –
http://sildenafilpriceguide.com/# Viagra generic over the counter
RandyHoody –
Order Viagra 50 mg online [url=https://sildenafilpriceguide.com/#]Sildenafil Price Guide[/url] Order Viagra 50 mg online
Thomasbar –
http://ivermectinaccessusa.com/# ivermectin 10 ml
Josephded –
US Pharma Index: US Pharma Index – no prescription pharmacy paypal
DavidMep –
safe canadian pharmacy: US Pharma Index – US Pharma Index
JeremyCow –
http://uspharmaindex.com/# US Pharma Index
Thomasbar –
https://sildenafilpriceguide.com/# Generic Viagra for sale
Josephded –
stromectol tablets buy online: stromectol tab 3mg – stromectol 15 mg
JeremyCow –
https://sildenafilpriceguide.com/# Cheap Sildenafil 100mg
RandyHoody –
US Pharma Index [url=https://uspharmaindex.shop/#]professional pharmacy[/url] online pharmacy drop shipping
DavidMep –
Ivermectin Access USA: Ivermectin Access USA – Ivermectin Access USA
Thomasbar –
https://sildenafilpriceguide.com/# Viagra generic over the counter
Josephded –
US Pharma Index: US Pharma Index – online canadian pharmacy coupon
JeremyCow –
http://ivermectinaccessusa.com/# Ivermectin Access USA
Josephded –
Ivermectin Access USA: Ivermectin Access USA – Ivermectin Access USA
Thomasbar –
https://uspharmaindex.shop/# US Pharma Index
JeremyCow –
http://sildenafilpriceguide.com/# Buy Viagra online cheap
DavidMep –
sildenafil over the counter: Viagra online price – best price for viagra 100mg
wrnhzorca –
To sign in, use your Zoom, Google, or Facebook account. You can also log in using SSO. If you don’t have an account, click Sign Up Free. If you have a Zoom account but cannot remember your password, click Forgot. A leading industry-standard video editor, Adobe Premiere Pro is known for its flexibility and integration with other Adobe apps. It supports various formats and offers advanced editing tools, making it a go-to choice for filmmakers, editors, and YouTubers. Adobe Premiere Pro is available for free with a 7-day trial. During this trial, you get full access to all features and updates in the latest version. Premiere Pro costs $20.99 for individuals and $35.99 per license for teams. It’s part of the Creative Cloud All Apps plan, which includes 20 other creative apps like Lightroom and Photoshop.
https://carnesvalidadas.com/neosurf-casino-review-the-best-online-casino-experience-for-australians/
The highest possible win in this game is 4,000x bet. Should you achieve this figure during Free Spins, the round will end and your win is awarded, although you will surrender any free spins you have left. Bigger Bass Bonanza focuses on the Free Spins feature. You can enter by hitting 3 or more Hooked Bass Scatter symbols anywhere on the reels. 3, 4 or 5 scatters will reward you with 10, 15 or 20 free spins respectively. Starting with online slots these are amongst some of the most diverse and popular types of online casino games, with these ranging from classically inspired fruit-machine style titles all the way to more modern and contemporary creations that boast innovative bonus features and immersive themes. There are several promotent slot variations, with one of the most dynamic of these being Megaways slots. These offer dynamic reel setups that could see the number of paylines change with every spin, with cascading mechanics also being common inclusions in these online casino games too.
Josephded –
buy Viagra online: Sildenafil Citrate Tablets 100mg – Cheapest Sildenafil online
Thomasbar –
https://ivermectinaccessusa.shop/# ivermectin lice
DavidMep –
buy viagra here: sildenafil 50 mg price – Viagra online price
JeremyCow –
http://ivermectinaccessusa.com/# Ivermectin Access USA
Josephded –
cheapest viagra: buy viagra here – cheap viagra
Thomasbar –
https://sildenafilpriceguide.shop/# buy Viagra over the counter
JeremyCow –
https://sildenafilpriceguide.com/# Cheap generic Viagra
RandyHoody –
Ivermectin Access USA [url=http://ivermectinaccessusa.com/#]Ivermectin Access USA[/url] Ivermectin Access USA
DavidMep –
Viagra without a doctor prescription Canada: Viagra generic over the counter – sildenafil online
Josephded –
stromectol oral: ivermectin oral solution – ivermectin lotion cost
Thomasbar –
http://uspharmaindex.com/# reputable online pharmacy
JeremyCow –
https://uspharmaindex.com/# US Pharma Index
Josephded –
US Pharma Index: US Pharma Index – script pharmacy
Thomasbar –
https://uspharmaindex.com/# canada pharmacy coupon
JeremyCow –
https://sildenafilpriceguide.shop/# Viagra online price
DavidMep –
Cheapest Sildenafil online: Sildenafil Price Guide – buy Viagra over the counter
RandyHoody –
buy Viagra over the counter [url=https://sildenafilpriceguide.shop/#]cheap viagra[/url] Generic Viagra online
Josephded –
ivermectin for humans: ivermectin lotion price – Ivermectin Access USA
JeremyCow –
https://uspharmaindex.com/# US Pharma Index
Josephded –
Buy Viagra online cheap: Sildenafil Price Guide – cheapest viagra
doadsnyro –
The super scatter is the headline addition over the original formula. When it arrives with regular scatters or under certain combinations, it boosts payout potential. Think of it as a premium scatter that can turbocharge feature value or yield instant rewards tied to the scatter system. Exact rewards vary by trigger count and mode, yet the presence of this symbol is the reason many grinders target this version over earlier Gates variants. Zeus returns in a new special edition of the award-winning original slot, Gates of Olympus Super Scatter. Use the Gates of Olympus Super Scatter demo to get a feel for the pay-anywhere 8+ match system and how the tumbling reels affect momentum. It’s a smart way to learn when wins cluster, how multipliers stack during free spins, and how Super Scatters behave alongside standard Scatters.
https://bsite.in/2026/02/25/beep-beep-casino-game-review-a-thrilling-ride-for-new-zealand-players/
gamespotmetacriticfandomfanatical HAYMA Baudienstleistungen The benefit icon is paramount so you can obtaining among 4 jackpot honours. Enjoy 1024 all the implies inside the Skywind’s Tiki Secret slot to own a possible opportunity to earn to 5000x their bet. Belongings up to 15 100 percent free video game and you can x3 multipliers to improve your winnings. Subscribe to our newsletter and get the latest trending products and offers updates. There are hundreds of slots released each year, and the majority of them have a very short lifespan. That’s why it’s truly impressive to have titles such as Gates of Olympus that manage to stay extremely popular for years. This slot has become an instant player-favorite and several years on, it keeps drawing a lot of gamblers. The twist from the Gates out of Olympus can lead to a fulfilling lead, nonetheless it’s the action and you may adventure of your own video game which make it it is divine. Of a graphic viewpoint, Doorways from Olympus is nothing in short supply of a masterpiece. Graphics are evident and you may in depth, set up against a background away from majestic Attach Olympus. The icon, from the great Zeus to the adored items, is created which have careful reliability, causing a aesthetically excellent game play feel. Gaming try flexible, accommodating both relaxed players and you can high-rollers, with options ranging from 0.20 in order to a hundred loans for every spin.
DavidMep –
pharmacy drugs: US Pharma Index – canadian pharmacy world coupon
Thomasbar –
https://uspharmaindex.shop/# US Pharma Index
JeremyCow –
https://sildenafilpriceguide.com/# Cheap Sildenafil 100mg
Josephded –
cheapest viagra: Cheap generic Viagra online – Buy generic 100mg Viagra online
RandyHoody –
ivermectin 2mg [url=https://ivermectinaccessusa.shop/#]Ivermectin Access USA[/url] Ivermectin Access USA
Thomasbar –
https://uspharmaindex.shop/# the peoples pharmacy
JeremyCow –
http://uspharmaindex.com/# US Pharma Index
DavidMep –
stromectol 3mg: ivermectin buy australia – Ivermectin Access USA
Josephded –
adderall canadian pharmacy: india pharmacy mail order – 24 hour pharmacy near me
Thomasbar –
https://sildenafilpriceguide.shop/# best price for viagra 100mg
JeremyCow –
http://sildenafilpriceguide.com/# Viagra Tablet price
Josephded –
ivermectin 2ml: Ivermectin Access USA – stromectol coronavirus
DavidMep –
Ivermectin Access USA: stromectol pills – Ivermectin Access USA
JeremyCow –
https://ivermectinaccessusa.shop/# ivermectin tablets
Thomasbar –
https://sildenafilpriceguide.com/# Cheap generic Viagra
RandyHoody –
canadian pharmacy in canada [url=http://uspharmaindex.com/#]rx pharmacy[/url] US Pharma Index
Josephded –
ivermectin 1 cream: ivermectin uk coronavirus – ivermectin topical
pinup_ggSi –
pin-up giriş kodu [url=https://pinup09715.help]https://pinup09715.help[/url]
JeremyCow –
http://ivermectinaccessusa.com/# Ivermectin Access USA
Thomasbar –
http://sildenafilpriceguide.com/# Cheap generic Viagra online
Josephded –
canadian compounding pharmacy: best canadian pharmacy to buy from – best australian online pharmacy
DavidMep –
stromectol price us: Ivermectin Access USA – stromectol pill
JeremyCow –
http://ivermectinaccessusa.com/# cost of ivermectin medicine
Thomasbar –
https://ivermectinaccessusa.shop/# stromectol xr
Josephded –
ivermectin cream cost: stromectol order – Ivermectin Access USA
RandyHoody –
order viagra [url=http://sildenafilpriceguide.com/#]Sildenafil Price Guide[/url] buy Viagra online
JeremyCow –
http://sildenafilpriceguide.com/# Generic Viagra for sale
DavidMep –
Viagra generic over the counter: Viagra online price – generic sildenafil
Josephded –
Sildenafil 100mg price: over the counter sildenafil – viagra without prescription
Thomasbar –
https://uspharmaindex.shop/# US Pharma Index
ihhefxkoz –
La colonna sonora di Gates of Olympus 1000 è una melodia veloce dai toni drammatici che ricorda i film d’azione; di tanto in tanto, la voce tonante di Giove esprime un commento sullo status di gioco dello scommettitore. Uno degli aspetti che cattura immediatamente l’attenzione in Games in Olympus 1000 è il potenziale moltiplicatore: fino a x1000. Ci sono dei simboli, di vario aspetto, che introducono nel gioco i moltiplicatori. Possono comparire sia nel gioco di base che durante la funzione bonus. Livello dei Moltiplicatori: si passa da 500x a 1000x in quanto le sfere di cristallo prendono un valore casuale che potrà aumentare il valore che aumenta la puntata totale. Le sfere non cambiano sia nei colori che nel numero (5) come nella stessa modalità di gioco. Più recente Games in Olympus 1000 si distingue per l’ambientazione ispirata ai giochi olimpici e ai simboli mitologici, offrendo una variazione tematica rispetto ad altri titoli della serie.
http://mtssbontonompo.com/recensione-di-amunra-il-gioco-casino-online-preferito-in-italia/
Vincere alla slot Gate of Olympus richiede una combinazione di fortuna e strategia. Comprendere le meccaniche del gioco, gestire il tuo budget in modo responsabile e sfruttare le funzioni speciali può aumentare le tue possibilità di successo. Ricorda sempre di giocare responsabilmente e di considerare il gioco d’azzardo come una forma di intrattenimento. Buona fortuna e buon divertimento! Nessun casinò italiano, a oggi, ha attiva alcuna promozione che offra bonus free spin per Gates of Olympus. Preparati a sfidare gli dei con Gates of Olympus slot, la celebre slot online di Pragmatic Play ispirata alla mitologia greca. Tra fulmini, moltiplicatori fino a 500× e giri gratis esplosivi, Zeus ti attende per offrirti un gameplay ricco di sorprese. Disponibile sia in versione Gates of Olympus gratis che con soldi veri, questa slot ad alta volatilità combina grafica mozzafiato e funzionalità innovative per un’esperienza di gioco epica.
JeremyCow –
https://uspharmaindex.com/# US Pharma Index
Josephded –
mexican pharmacy: US Pharma Index – US Pharma Index
Thomasbar –
https://uspharmaindex.shop/# US Pharma Index
DavidMep –
buy viagra here: Sildenafil Price Guide – buy Viagra over the counter
JeremyCow –
http://sildenafilpriceguide.com/# order viagra
Josephded –
stromectol 6 mg dosage: Ivermectin Access USA – ivermectin lotion for lice
RandyHoody –
Viagra online price [url=https://sildenafilpriceguide.shop/#]Sildenafil Price Guide[/url] sildenafil over the counter
Thomasbar –
http://sildenafilpriceguide.com/# Cheapest Sildenafil online
JeremyCow –
https://ivermectinaccessusa.com/# Ivermectin Access USA
Josephded –
Viagra online price: Sildenafil Price Guide – cheap viagra
DavidMep –
buy ivermectin canada: Ivermectin Access USA – Ivermectin Access USA
ckozkbray –
Sugar Rush 1000 présente une volatilité élevée, ce qui signifie que les gains peuvent être rares mais potentiellement énormes. Avec un gain maximum de 25 000x la mise, ce jeu s’adresse aux joueurs en quête de sensations fortes et de gros jackpots. Après avoir passé des semaines entières à nous régaler sur Sugar Rush, nous nous disons qu’un bon 4,8 5 est mérité. Cette machine à sous est un peu notre coup de cœur. Les graphismes sont un régal pour les yeux et le gameplay, d’une originalité captivante, offre une expérience de jeu mémorable. Malgré la diversité dans le catalogue du développeur, la majorité des joueurs préfèrent la slot de Pragmatic Play Sugar Rush. Cela est dû à la combinaison réussie de son design, ses caractéristiques et de bonnes opportunités de gain.
https://growstack.blog/2026/02/26/analyse-de-la-popularite-du-jeu-de-casino-1xbet-en-france/
Grâce à sa réalisation soignée, ses effets visuels intenses et sa bande-son épique, chaque rotation se transforme en combat divin pour décrocher les trésors de l’Olympe. En France, les fournisseurs de jeux de casino les plus populaires incluent Play Pragmatic, Веtsоft Gаmіng, Еndоrрhіnа, Nоvоmаtіс et Hасksаw Gаmіng. Ces éditeurs sont reconnus pour la qualité graphique de leurs machines, la fluidité de leur gameplay et la variété des fonctionnalités. On les retrouve dans presque tous les casinos français sérieux, ce qui permet aux joueurs de découvrir régulièrement des offres de frее-sріns ou des tоurnоіs sur leurs titres. Le premier casino à proposer cette version était le Grand Monte Carlo, grâce à la technologie HTML5. Surtout dans le monde sophistiqué de l’iGaming d’aujourd’hui, Un Rêve d’Haufor sera à reprendre dans ce lot. Avantages et inconvénients gates of olympus lorsque vous jouez pour de l’argent réel, des corbeaux.
Thomasbar –
https://uspharmaindex.shop/# canadian world pharmacy
JeremyCow –
https://sildenafilpriceguide.shop/# Cheap Sildenafil 100mg
Josephded –
order viagra: sildenafil 50 mg price – Viagra online price
Thomasbar –
http://uspharmaindex.com/# secure medical online pharmacy
DavidMep –
Order Viagra 50 mg online: Viagra tablet online – Cheapest Sildenafil online
JeremyCow –
https://uspharmaindex.com/# canadian discount pharmacy
Josephded –
viagra without prescription: Buy generic 100mg Viagra online – cheapest viagra
RandyHoody –
Buy Viagra online cheap [url=https://sildenafilpriceguide.shop/#]Sildenafil Price Guide[/url] buy Viagra online
Thomasbar –
http://uspharmaindex.com/# 24 hours pharmacy
JeremyCow –
https://sildenafilpriceguide.shop/# Cheapest Sildenafil online
Josephded –
Generic Viagra online: Sildenafil Price Guide – sildenafil over the counter
DavidMep –
best online canadian pharmacy: US Pharma Index – online pharmacy in turkey
Thomasbar –
http://uspharmaindex.com/# US Pharma Index
Josephded –
online pharmacy india: US Pharma Index – tadalafil canadian pharmacy
JeremyCow –
http://uspharmaindex.com/# US Pharma Index
RandyHoody –
Ivermectin Access USA [url=https://ivermectinaccessusa.com/#]ivermectin uk[/url] ivermectin 200mg
Josephded –
Ivermectin Access USA: stromectol tablets for humans – Ivermectin Access USA
JeremyCow –
https://ivermectinaccessusa.com/# Ivermectin Access USA
Thomasbar –
https://sildenafilpriceguide.shop/# Cheap generic Viagra online
DavidMep –
over the counter sildenafil: Sildenafil Price Guide – viagra without prescription
Josephded –
US Pharma Index: US Pharma Index – US Pharma Index
Thomasbar –
https://uspharmaindex.shop/# online canadian pharmacy reviews
mostbet_euel –
мостбет промокод для Кыргызстана [url=www.mostbet39081.help]www.mostbet39081.help[/url]
DavidMep –
mail order pharmacy: online pharmacy no rx – online canadian pharmacy coupon
Josephded –
US Pharma Index: US Pharma Index – US Pharma Index
Thomasbar –
https://sildenafilpriceguide.com/# viagra canada
Josephded –
Viagra tablet online: viagra without prescription – Buy generic 100mg Viagra online
JeremyCow –
https://uspharmaindex.shop/# viagra canadian pharmacy vipps approved
Thomasbar –
http://sildenafilpriceguide.com/# over the counter sildenafil
DavidMep –
Ivermectin Access USA: ivermectin 4000 mcg – ivermectin eye drops
Josephded –
canadian online pharmacy no prescription: US Pharma Index – 24 hours pharmacy
JeremyCow –
https://sildenafilpriceguide.shop/# sildenafil over the counter
Thomasbar –
https://sildenafilpriceguide.com/# sildenafil 50 mg price
Josephded –
ivermectin buy australia: stromectol price us – stromectol australia
DavidMep –
ivermectin gel: ivermectin 1 cream – ivermectin oral solution
JeremyCow –
https://ivermectinaccessusa.com/# ivermectin cream 5%
RandyHoody –
US Pharma Index [url=https://uspharmaindex.shop/#]US Pharma Index[/url] canadian pharmacy coupon code
Thomasbar –
http://ivermectinaccessusa.com/# stromectol price in india
Josephded –
canadian pharmacy price checker: which online pharmacy is reliable – US Pharma Index
DavidMep –
Ivermectin Access USA: Ivermectin Access USA – stromectol in canada
Thomasbar –
https://uspharmaindex.com/# maple leaf pharmacy in canada
Josephded –
Viagra tablet online: buy Viagra online – sildenafil 50 mg price
JeremyCow –
https://sildenafilpriceguide.shop/# Viagra tablet online
Josephded –
online pharmacy uk: US Pharma Index – US Pharma Index
Thomasbar –
https://uspharmaindex.shop/# US Pharma Index
RandyHoody –
Viagra without a doctor prescription Canada [url=http://sildenafilpriceguide.com/#]buy Viagra online[/url] sildenafil 50 mg price
JeremyCow –
https://sildenafilpriceguide.com/# buy viagra here
DavidMep –
buy ivermectin nz: ivermectin tablets uk – cost of ivermectin medicine
Josephded –
US Pharma Index: sure save pharmacy – online pharmacy ed
Thomasbar –
https://sildenafilpriceguide.shop/# Viagra online price
JeremyCow –
https://sildenafilpriceguide.shop/# Viagra online price
Josephded –
US Pharma Index: US Pharma Index – US Pharma Index
DavidMep –
US Pharma Index: US Pharma Index – walmart pharmacy online
Thomasbar –
https://sildenafilpriceguide.com/# Generic Viagra online
JeremyCow –
https://sildenafilpriceguide.com/# buy Viagra online
RandyHoody –
vipps approved canadian online pharmacy [url=http://uspharmaindex.com/#]super saver pharmacy[/url] on line pharmacy
Josephded –
Ivermectin Access USA: Ivermectin Access USA – ivermectin where to buy
Thomasbar –
https://sildenafilpriceguide.shop/# Buy generic 100mg Viagra online
JeremyCow –
https://sildenafilpriceguide.com/# Viagra generic over the counter
DavidMep –
mail order pharmacy: cheapest pharmacy – US Pharma Index
Josephded –
Cheapest Sildenafil online: Viagra online price – Buy generic 100mg Viagra online
JeremyCow –
https://uspharmaindex.shop/# US Pharma Index
mostbet_unea –
mostbet подтверждение личности [url=http://mostbet85961.help]http://mostbet85961.help[/url]
Thomasbar –
https://sildenafilpriceguide.shop/# Buy generic 100mg Viagra online
Josephded –
Ivermectin Access USA: Ivermectin Access USA – Ivermectin Access USA
DavidMep –
buy Viagra online: best price for viagra 100mg – sildenafil 50 mg price
JeremyCow –
http://sildenafilpriceguide.com/# Sildenafil Citrate Tablets 100mg
RandyHoody –
canadian pharmacy generic viagra [url=https://uspharmaindex.shop/#]usa pharmacy[/url] cialis canadian pharmacy
Thomasbar –
http://sildenafilpriceguide.com/# buy Viagra over the counter
Josephded –
Ivermectin Access USA: Ivermectin Access USA – ivermectin iv
HenryTut –
https://petmedsmonitor.shop/# pet meds online
TylerHat –
https://petmedsmonitor.com/# п»їdog medication online
AndrewDar –
Certified Canada Rx: Certified Canada Rx – canadian pharmacy meds
Williamhex –
ed medicine online: ed online treatment – Mens RX Index
HenryTut –
http://certifiedcanadarx.com/# Certified Canada Rx
AndrewDar –
Certified Canada Rx: canadian pharmacy 1 internet online drugstore – canada drug pharmacy
TylerHat –
https://petmedsmonitor.shop/# online pet pharmacy
RobertBut –
ed medication online [url=https://mensrxindex.com/#]Mens RX Index[/url] Mens RX Index
HenryTut –
http://certifiedcanadarx.com/# canadian pharmacy sarasota
Williamhex –
canadian valley pharmacy: northwest pharmacy canada – Certified Canada Rx
AndrewDar –
Certified Canada Rx: Certified Canada Rx – Certified Canada Rx
TylerHat –
https://mensrxindex.com/# ed med online
HenryTut –
https://certifiedcanadarx.shop/# Certified Canada Rx
AndrewDar –
Certified Canada Rx: Certified Canada Rx – buy canadian drugs
RobertBut –
Certified Canada Rx [url=http://certifiedcanadarx.com/#]pharmacy in canada[/url] Certified Canada Rx
Williamhex –
Certified Canada Rx: best rated canadian pharmacy – canadian pharmacy world reviews
HenryTut –
http://petmedsmonitor.com/# best pet rx
AndrewDar –
Certified Canada Rx: trustworthy canadian pharmacy – ordering drugs from canada
TylerHat –
https://mensrxindex.com/# ed meds on line
AndrewDar –
discount pet meds: Vet Rx Index – pet pharmacy online
HenryTut –
https://petmedsmonitor.com/# pet pharmacy
Williamhex –
Certified Canada Rx: Certified Canada Rx – Certified Canada Rx
RobertBut –
canadian pharmacy 365 [url=http://certifiedcanadarx.com/#]Certified Canada Rx[/url] canadian pharmacy online
AndrewDar –
legal to buy prescription drugs from canada: Certified Canada Rx – online canadian drugstore
TylerHat –
https://mensrxindex.com/# Mens RX Index
HenryTut –
http://certifiedcanadarx.com/# Certified Canada Rx
AndrewDar –
ed pills cheap: ed med online – Mens RX Index
TylerHat –
https://certifiedcanadarx.shop/# Certified Canada Rx
HenryTut –
https://certifiedcanadarx.shop/# buy drugs from canada
Williamhex –
pet pharmacy online: Vet Rx Index – online vet pharmacy
AndrewDar –
safe reliable canadian pharmacy: canadian drugs – canadian pharmacy no rx needed
TylerHat –
https://mensrxindex.com/# online ed pills
RobertBut –
Certified Canada Rx [url=https://certifiedcanadarx.com/#]canada drugs online review[/url] canadian drugs pharmacy
HenryTut –
http://certifiedcanadarx.com/# Certified Canada Rx
mostbet_uaOa –
мостбет кэшбэк условия [url=http://mostbet96810.help]http://mostbet96810.help[/url]
mostbet_ispl –
мостбет приложение не работает [url=www.mostbet15247.help]www.mostbet15247.help[/url]
AndrewDar –
pet pharmacy: pet rx – п»їdog medication online
Williamhex –
canada pet meds: Vet Rx Index – best pet rx
TylerHat –
http://mensrxindex.com/# ed meds cheap
HenryTut –
http://petmedsmonitor.com/# canada pet meds
AndrewDar –
canadian pharmacy checker: pharmacy in canada – canadian pharmacy prices
TylerHat –
http://mensrxindex.com/# online erectile dysfunction medication
Williamhex –
edmeds: Mens RX Index – cheap ed meds
RobertBut –
pet meds official website [url=http://petmedsmonitor.com/#]Vet Rx Index[/url] best pet rx
TylerHat –
http://petmedsmonitor.com/# online vet pharmacy
AndrewDar –
ed drugs online from canada: canadian pharmacy meds review – northern pharmacy canada
Williamhex –
ed meds cheap: Mens RX Index – cheap ed pills
TylerHat –
https://mensrxindex.com/# Mens RX Index
AndrewDar –
canada ed drugs: Certified Canada Rx – canadian online pharmacy
TylerHat –
http://mensrxindex.com/# ed medications cost
AndrewDar –
online ed medicine: Mens RX Index – Mens RX Index
RobertBut –
Certified Canada Rx [url=http://certifiedcanadarx.com/#]Certified Canada Rx[/url] Certified Canada Rx
AndrewDar –
Mens RX Index: Mens RX Index – how to get ed pills
TylerHat –
https://certifiedcanadarx.com/# canadian pharmacy com
Williamhex –
order ed pills: buy erectile dysfunction treatment – online ed medication
AndrewDar –
pet meds for dogs: п»їdog medication online – pet drugs online
TylerHat –
https://certifiedcanadarx.com/# Certified Canada Rx
AndrewDar –
Certified Canada Rx: best rated canadian pharmacy – canadian pharmacy cheap
RobertBut –
Mens RX Index [url=http://mensrxindex.com/#]online prescription for ed[/url] ed medicine online
TylerHat –
https://petmedsmonitor.com/# pet meds official website
Williamhex –
dog prescriptions online: Vet Rx Index – dog medication online
AndrewDar –
Mens RX Index: ed meds online – cheap ed treatment
TylerHat –
https://mensrxindex.com/# Mens RX Index
AndrewDar –
Mens RX Index: ed medication online – Mens RX Index
Williamhex –
trustworthy canadian pharmacy: Certified Canada Rx – safe online pharmacies in canada
AndrewDar –
Certified Canada Rx: canadian pharmacy meds review – Certified Canada Rx
RobertBut –
Mens RX Index [url=https://mensrxindex.shop/#]Mens RX Index[/url] online erectile dysfunction pills
TylerHat –
https://petmedsmonitor.com/# dog prescriptions online
Williamhex –
Certified Canada Rx: Certified Canada Rx – Certified Canada Rx
HenryTut –
http://mensrxindex.com/# Mens RX Index
AndrewDar –
canadian neighbor pharmacy: canadian drug prices – canada pharmacy online
HenryTut –
http://petmedsmonitor.com/# pet med
AndrewDar –
Certified Canada Rx: canadian world pharmacy – canadian pharmacy ltd
Williamhex –
dog prescriptions online: dog prescriptions online – pet rx
TylerHat –
https://mensrxindex.shop/# cheap ed meds
HenryTut –
https://mensrxindex.com/# Mens RX Index
AndrewDar –
pet pharmacy online: Vet Rx Index – vet pharmacy online
RobertBut –
Certified Canada Rx [url=https://certifiedcanadarx.shop/#]canada cloud pharmacy[/url] Certified Canada Rx
AndrewDar –
pet meds for dogs: dog medicine – dog prescriptions online
HenryTut –
https://certifiedcanadarx.shop/# Certified Canada Rx
Williamhex –
Mens RX Index: edmeds – ed doctor online
AndrewDar –
Certified Canada Rx: Certified Canada Rx – Certified Canada Rx
HenryTut –
https://petmedsmonitor.com/# pet drugs online
TylerHat –
http://petmedsmonitor.com/# online pet pharmacy
RobertBut –
canadian compounding pharmacy [url=http://certifiedcanadarx.com/#]Certified Canada Rx[/url] reliable canadian pharmacy reviews
Williamhex –
Mens RX Index: ed medicines online – Mens RX Index
AndrewDar –
canada online pharmacy: vipps canadian pharmacy – canadian pharmacy review
HenryTut –
https://petmedsmonitor.shop/# discount pet meds
TylerHat –
https://mensrxindex.shop/# ed doctor online
AndrewDar –
canadian drug pharmacy: canadian pharmacy near me – Certified Canada Rx
HenryTut –
https://petmedsmonitor.com/# vet pharmacy
TylerHat –
http://certifiedcanadarx.com/# Certified Canada Rx
Williamhex –
pet rx: Vet Rx Index – dog medicine
AndrewDar –
buy erectile dysfunction pills: ed medication online – Mens RX Index
HenryTut –
https://mensrxindex.shop/# boner pills online
RobertBut –
cheap boner pills [url=https://mensrxindex.shop/#]Mens RX Index[/url] Mens RX Index
TylerHat –
https://petmedsmonitor.com/# pet meds online
AndrewDar –
Certified Canada Rx: Certified Canada Rx – Certified Canada Rx
HenryTut –
https://certifiedcanadarx.shop/# Certified Canada Rx
TylerHat –
https://mensrxindex.shop/# online erectile dysfunction
AndrewDar –
dog prescriptions online: pet drugs online – canada pet meds
HenryTut –
https://certifiedcanadarx.shop/# Certified Canada Rx
Williamhex –
ed medications online: Mens RX Index – online erectile dysfunction prescription
AndrewDar –
online erectile dysfunction medication: Mens RX Index – Mens RX Index
RobertBut –
Certified Canada Rx [url=https://certifiedcanadarx.shop/#]Certified Canada Rx[/url] canadian pharmacy world
HenryTut –
https://certifiedcanadarx.shop/# Certified Canada Rx
TylerHat –
https://mensrxindex.com/# Mens RX Index
AndrewDar –
Mens RX Index: ed rx online – Mens RX Index
HenryTut –
https://mensrxindex.shop/# get ed prescription online
Williamhex –
how to get ed pills: Mens RX Index – Mens RX Index
melbet_hoPa –
мелбет ставки Казахстан [url=https://melbet60432.help]https://melbet60432.help[/url]
melbet_tvoi –
melbet pariuri cs2 [url=melbet42310.help]melbet42310.help[/url]
AndrewDar –
online vet pharmacy: best pet rx – pet meds online
HenryTut –
https://petmedsmonitor.com/# pet meds online
RobertBut –
canadian online pharmacy [url=http://certifiedcanadarx.com/#]Certified Canada Rx[/url] reputable canadian online pharmacy
Williamhex –
pet meds for dogs: Vet Rx Index – pet pharmacy online
AndrewDar –
vet pharmacy: Vet Rx Index – pet pharmacy
TylerHat –
https://petmedsmonitor.shop/# canada pet meds
HenryTut –
https://petmedsmonitor.com/# vet pharmacy
AndrewDar –
Mens RX Index: Mens RX Index – Mens RX Index
TylerHat –
https://petmedsmonitor.com/# discount pet meds
HenryTut –
https://certifiedcanadarx.com/# Certified Canada Rx
Williamhex –
vet pharmacy: pet rx – discount pet meds
AndrewDar –
pet rx: pet meds online – discount pet meds
pinup_upEr –
pin-up server muammo [url=pinup14278.help]pinup14278.help[/url]
TylerHat –
http://mensrxindex.com/# Mens RX Index
HenryTut –
https://certifiedcanadarx.shop/# Certified Canada Rx
RobertBut –
pet pharmacy online [url=http://petmedsmonitor.com/#]Vet Rx Index[/url] pet meds for dogs
AndrewDar –
Mens RX Index: Mens RX Index – Mens RX Index
Williamhex –
online vet pharmacy: vet pharmacy – pet meds online
HenryTut –
http://certifiedcanadarx.com/# Certified Canada Rx
TylerHat –
https://petmedsmonitor.shop/# online pet pharmacy
Franciskat –
austria pharmacy online: US Meds Saver – specialty pharmacy
Thomasplaix –
http://certifiednorthrx.com/# legit canadian pharmacy online
Davidfah –
https://usmedssaver.com/# legit canadian pharmacy
WilliamDUalo –
prescription drugs from canada [url=http://usmedssaver.com/#]reputable indian pharmacies[/url] medical pharmacy south
Franciskat –
BajaRx Direct: BajaRx Direct – BajaRx Direct
Jamesfinom –
best canadian online pharmacy: Certified North Rx – pharmacy wholesalers canada
Davidfah –
http://certifiednorthrx.com/# Certified North Rx
Thomasplaix –
http://certifiednorthrx.com/# Certified North Rx
Franciskat –
canadian pharmacy world reviews: Certified North Rx – canadian pharmacy meds
Davidfah –
http://usmedssaver.com/# safe canadian pharmacy
Jamesfinom –
mexican online pharmacy: mexico pharmacy – farmacia pharmacy mexico
Thomasplaix –
https://certifiednorthrx.com/# canadian pharmacy india
mostbet_hbSt –
mostbet fără verificare [url=mostbet63218.help]mostbet63218.help[/url]
Franciskat –
BajaRx Direct: mexican pharmacy online – mexican medicine
WilliamDUalo –
pharmacy discount coupons [url=https://usmedssaver.com/#]US Meds Saver[/url] which online pharmacy is reliable
Davidfah –
http://usmedssaver.com/# onlinecanadianpharmacy
Franciskat –
northern pharmacy canada: Certified North Rx – Certified North Rx
Thomasplaix –
http://certifiednorthrx.com/# Certified North Rx
Jamesfinom –
legitimate canadian mail order pharmacy: Certified North Rx – safe canadian pharmacy
Davidfah –
https://certifiednorthrx.com/# Certified North Rx
Franciskat –
thecanadianpharmacy: Certified North Rx – Certified North Rx
Thomasplaix –
https://usmedssaver.shop/# canadian king pharmacy
WilliamDUalo –
order medication from mexico [url=http://bajarxdirect.com/#]farmacias mexicanas[/url] BajaRx Direct
Davidfah –
http://certifiednorthrx.com/# Certified North Rx
Franciskat –
foreign pharmacy no prescription: canada drugs – online pharmacy delivery
mostbet_zepr –
mostbet yuklab olish uz [url=https://mostbet28461.help]https://mostbet28461.help[/url]
Thomasplaix –
https://certifiednorthrx.com/# canadian pharmacy price checker
Franciskat –
BajaRx Direct: BajaRx Direct – mexican mail order pharmacy
Davidfah –
http://bajarxdirect.com/# BajaRx Direct
Thomasplaix –
http://certifiednorthrx.com/# Certified North Rx
yquaytklw –
Yes, it supports 4K video editing on Windows 10 and 11, meaning you can work with higher-resolution videos and create content with increased visual clarity. Here are some basic ClipChamp features Video Editor Features Record audio, screen, and webcam securely, using Windows and Mac devices. Enjoy unlimited retakes, improve sound and video quality with AI tools, and export audio and video in HD quality. VEED is my one-stop video editing shop! It’s cut my editing time by around 60%, freeing me to focus on my online career coaching business. If you’re working with professional video-editing software, adding even the simplest video transition may take you hours of pressing wrong buttons and digging for advice. Certainly not a pleasant experience. With Movavi Video Editor, adding a transition takes about 3 seconds – you just drag and drop the transition you want between the clips. Yes, it really is that simple. To learn more about different types of transitions, follow the link below: How to choose transitions for your video
https://500px.com/p/oliverreed?view=photos
The CapCut desktop video editor makes it easy to turn your photos into fun and animated creations. You can add movement, stylish effects, and text to bring still images to life. It is designed for everyday users, so you do not need editing experience to get started. Whether you are working on a project or just having fun, CapCut gives you the tools to create something unique. A Text to Image AI art generator is now available in Motionleap and it is BIG:Just type in any description and watch it turn to an AI-generated artwork in seconds.From “An alien-ballerina scuba diving in the style of Picasso” to “A painting of a seagull pondering the meaning of life in a photorealistic style”, anything is possible!Let your creativity run wilder than ever!Try it for yourself and get your mind blown.
Franciskat –
mexico meds: BajaRx Direct – mexican pharmacies
Jamesfinom –
recommended canadian pharmacies: safe online pharmacies – pharmacy home delivery
Davidfah –
http://certifiednorthrx.com/# pharmacies in canada that ship to the us
WilliamDUalo –
Certified North Rx [url=https://certifiednorthrx.shop/#]Certified North Rx[/url] canadian pharmacy world
Thomasplaix –
https://bajarxdirect.com/# best mexican pharmacy
Lewisacice –
https://vaycasinovip.online/# vaycasino giriş
Davidfah –
http://certifiednorthrx.com/# canadian pharmacy meds
Thomasplaix –
https://certifiednorthrx.com/# canadian pharmacy meds
Lewisacice –
vaycasino: vaycasino
mostbet_hbSt –
мостбет вывод на карту [url=https://www.mostbet57193.help]https://www.mostbet57193.help[/url]
Davidfah –
https://bajarxdirect.com/# medicine from mexico
Thomasplaix –
https://usmedssaver.shop/# canadian prescription pharmacy
WilliamDUalo –
BajaRx Direct [url=http://bajarxdirect.com/#]BajaRx Direct[/url] BajaRx Direct
Lewisacice –
https://vaycasinovip.online/# vaycasino giriş
Davidfah –
https://certifiednorthrx.shop/# Certified North Rx
Jamesfinom –
best canadian pharmacy to order from: www canadianonlinepharmacy – canadian pharmacy checker
Thomasplaix –
https://certifiednorthrx.shop/# canadian pharmacy
Lewisacice –
vaycasino resmi giriş: vaycasino
Davidfah –
https://bajarxdirect.com/# mexican pharmacy prices
Thomasplaix –
https://bajarxdirect.com/# BajaRx Direct
WilliamDUalo –
which pharmacy is cheaper [url=http://usmedssaver.com/#]mail order pharmacy[/url] safe online pharmacy
Jamesfinom –
Certified North Rx: best canadian pharmacy to order from – canadian pharmacy oxycodone
Davidfah –
https://certifiednorthrx.com/# canadian pharmacy near me
Thomasplaix –
https://bajarxdirect.com/# BajaRx Direct
Davidfah –
https://usmedssaver.com/# www pharmacyonline
Melvinzitly –
https://holiganbetvip.buzz/# holiganbet
Vicentegluri –
holiganbet resmi giris [url=https://holiganbetvip.top/#]holiganbet[/url]
mostbet_lvpi –
mostbet приложение не запускается [url=http://mostbet94063.help/]http://mostbet94063.help/[/url]
Jamesfinom –
mexi pharmacy: mexican pharmacies – BajaRx Direct
Melvinzitly –
holiganbet giriş: holiganbet
DonaldSlisp –
https://urologymax.com/conditions/low-testosterone-low-t.html# best online ed meds
Vicentegluri –
https://holiganbetvip.top/# holiganbet giris
ccslcgzpa –
Snai rappresenta uno dei rarissimi casino online con Plinko X di Smartsoft. Questa versione del gioco si basa su una griglia, quindi non ha linee o rulli tipici delle slot machine tradizionali. Tuttavia, offre altre caratteristiche interessanti, come i Moltiplicatori e le Funzioni Speciali. In particolare, le funzioni speciali di Plinko X sono il bonus Plinko e il moltiplicatore X. Il primo può attivarsi in modo casuale, offrendo una nuova pallina o un moltiplicatore maggiore. Nella sezione casinò di CasinoMania troverai due varianti. Oltre a Plinko (RTP 92.03%) di Hacksaw Gaming, è presente Plinko Go (RTP 96%) di 1x2gaming. Ha tra le 8 e le 14 linee, configurabili a piacimento, così come il livello di rischio, tra basso, medio e alto. Il pagamento massimo è di 420 volte la scommessa, di importo compreso tra 0,10€ e 50€.
http://ncpotteryblog.com/?p=270078
Per giocare a Plinko su Lottomatica è necessario avere un conto gioco attivo. Tuttavia, per i più curiosi che vogliono provare il gioco senza spendere soldi ed essere per forza iscritti, c’è la possibilità di provare la demo gratuitamente. Plinko su Lottomatica si trova dentro l’area “Casinò”, non in quella “Slot” come invece abbiamo visto per altre piattaforme. Dal menù principale, quindi, selezionare prima “Casinò” e poi il sottomenù “Soft Games”. A quel punto, scorrendo verso il basso la pagina, Plinko arà uno dei primi giochi visibili. In alternativa c’è sempre la barra di ricerca. Nelle recensioni di plinko soldi veri le promo per giocare gratis sono l’argomento più ricercato: vediamo dunque i bonus casinò top che includono plinko come gioco qualificante per i requisiti di puntata e la spendibilità del real bonus.
Melvinzitly –
holiganbet [url=https://holiganbetvip.top/#]holiganbet[/url]
RonaldAnini –
low cost ed medication: Urology Max – cheap erectile dysfunction pills
DonaldSlisp –
https://urologymax.shop/ed-medications.html# ed meds by mail
Melvinzitly –
https://holiganbetvip.top/# holiganbet giris
DonaldSlisp –
https://urologymax.shop/conditions/prostate-cancer.html# ed pills for sale
Vicentegluri –
https://holiganbetvip.buzz/# holiganbet giris
RonaldAnini –
cheap ed pills online: ed medications – cheapest online ed treatment
Melvinzitly –
holiganbet resmi giriş [url=https://holiganbetvip.buzz/#]holiganbet[/url]
mostbet_rtoa –
most bet live [url=http://mostbet53160.help]most bet live[/url]
mostbet_rlOi –
mostbet slot játékok [url=https://www.mostbet2023.help]https://www.mostbet2023.help[/url]
DonaldSlisp –
https://urologymax.shop/conditions/erectile-dysfunction.html# cheap erection pills
Vicentegluri –
holiganbet resmi [url=https://holiganbetvip.top/#]holiganbet[/url]
JimmyTon –
holiganbet [url=https://holiganbetvip.top/#]holiganbet[/url]
Melvinzitly –
https://holiganbetvip.top/# holiganbet güncel
DonaldSlisp –
https://urologymax.shop/conditions/erectile-dysfunction.html# get ed prescription online
Vicentegluri –
holiganbet giris [url=https://holiganbetvip.top/#]holiganbet[/url]
RonaldAnini –
best ed medication online: UrologyMax – buying ed pills online
melbet_mtpl –
мелбет лайв [url=http://melbet47086.help/]http://melbet47086.help/[/url]
DonaldSlisp –
https://urologymax.com/conditions/prostate-cancer.html# pills for erectile dysfunction online
Vicentegluri –
holiganbet guncel adres [url=https://holiganbetvip.buzz/#]holiganbet[/url]
Melvinzitly –
holiganbet resmi giriş: holiganbet
RonaldAnini –
order ed meds online: UrologyMax – get ed meds online
DonaldSlisp –
https://urologymax.shop/conditions/low-testosterone-low-t.html# online erectile dysfunction pills
WilliamTop –
padisahbet: padisahbet
Lewisbib –
padişahbet güncel [url=https://padisahbetvip.online/#]padişahbet[/url]
BruceBluts –
https://padisahbetvip.online/# padişahbet güncel
DonaldSlisp –
https://urologymax.shop/conditions/prostate-cancer.html# how to get ed meds online
RonaldAnini –
ed meds cheap: ed medications – best ed medication online
mostbet_koPl –
мостбет вывод средств [url=mostbet82043.help]mostbet82043.help[/url]
Lewisbib –
padişahbet güncel: padişahbet
BruceBluts –
padişahbet resmi [url=https://padisahbetvip.online/#]padişahbet[/url]
DonaldSlisp –
https://urologymax.com/# online ed medication
Richardkaw –
betnano: betnano
DonaldSlisp –
https://urologymax.shop/# cheapest ed treatment
RonaldAnini –
ed pills for sale: Urology Max – online ed pharmacy
Jeffreyved –
https://betnano1st.online/# betnano resmi
ThomasWhene –
vdcasino güncel giriş [url=https://vdcasino1st.blog/#]vdcasino[/url]
Richardkaw –
betnano resmi [url=https://betnano1st.top/#]betnano[/url]
DonaldSlisp –
https://urologymax.shop/# cheap ed meds
RonaldAnini –
online ed meds: UrologyMax – what is the cheapest ed medication
ThomasWhene –
https://vdcasino1st.blog/# vdcasino güncel
Richardkaw –
betnano resmi giriş [url=https://betnano1st.online/#]betnano[/url]
DonaldSlisp –
https://urologymax.shop/conditions/prostate-cancer.html# cheapest ed pills
Jeffreyved –
betnano resmi [url=https://betnano1st.top/#]betnano[/url]
ThomasWhene –
vdcasino resmi [url=https://vdcasino1st.online/#]vdcasino[/url]
Richardkaw –
https://betnano1st.top/# betnano giriş
DonaldSlisp –
https://urologymax.shop/conditions/erectile-dysfunction.html# best online ed medication
Ernesthiz –
https://matbet1st.online/# matbet resmi
ThomasWhene –
https://vdcasino1st.online/# vdcasino güncel giriş
Donaldfloak –
https://cassiteleri.top/# lisanslı casino siteleri
ThomasWhene –
https://vdcasino1st.online/# vdcasino güncel adres
Robertnut –
güvenilir casino siteleri [url=https://cassiteleri.buzz/#]güvenilir casino siteleri[/url]
AaronHom –
https://cassiteleri.top/# güvenilir casino siteleri
ThomasWhene –
vdcasino giriş: vdcasino
JeffreyVed –
güvenilir casino siteleri [url=https://cassiteleri.top/#]lisanslı casino siteleri[/url]
Robertnut –
https://cassiteleri.buzz/# lisanslı casino siteleri
Donaldfloak –
lisanslı casino siteleri [url=https://cassiteleri.top/#]deneme bonusu veren casino siteleri[/url]
pinup_jzKi –
pin up Uzcard [url=http://pinup76809.help/]http://pinup76809.help/[/url]
ThomasWhene –
https://vdcasino1st.online/# vdcasino güncel adres
Robertnut –
deneme bonusu veren casino siteleri: lisanslı casino siteleri
Donaldfloak –
deneme bonusu veren casino siteleri [url=https://cassiteleri.top/#]güvenilir casino siteleri[/url]
ThomasWhene –
https://vdcasino1st.blog/# vdcasino güncel
Robertnut –
deneme bonusu veren casino siteleri: casino deneme siteleri
Donaldfloak –
deneme bonusu veren casino siteleri: lisanslı casino siteleri
mostbet_mzOt –
mostbet działa w polsce [url=http://mostbet2003.help/]http://mostbet2003.help/[/url]
pinup_dtsi –
pin up ilovani yuklab olish [url=https://pinup23185.help]https://pinup23185.help[/url]
ThomasWhene –
https://vdcasino1st.online/# vdcasino güncel giriş
Robertnut –
deneme bonusu veren casino siteleri [url=https://cassiteleri.top/#]lisanslı casino siteleri[/url]
Donaldfloak –
güvenilir casino siteleri: güvenilir casino siteleri
Robertnut –
lisanslı casino siteleri: casino deneme siteleri
AaronHom –
deneme bonusu veren casino siteleri [url=https://cassiteleri.top/#]deneme bonusu veren casino siteleri[/url]
JeffreyVed –
https://cassiteleri.top/# casino deneme siteleri
Donaldfloak –
lisanslı casino siteleri: casino deneme siteleri
ThomasWhene –
vdcasino [url=https://vdcasino1st.blog/#]vdcasino[/url]
mostbet_lyMr –
мостбет скачать на телефон [url=www.mostbet34518.help]www.mostbet34518.help[/url]
ThomasWhene –
vdcasino resmi [url=https://vdcasino1st.online/#]vdcasino[/url]
Robertnut –
casino deneme siteleri: casino deneme siteleri
ThomasWhene –
https://vdcasino1st.online/# vdcasino giriş
Robertnut –
https://cassiteleri.buzz/# casino siteleri
ThomasWhene –
vdcasino güncel giriş: vdcasino
Robertnut –
https://cassiteleri.top/# deneme bonusu veren casino siteleri
ThomasWhene –
vdcasino güncel [url=https://vdcasino1st.blog/#]vdcasino[/url]
AaronHom –
deneme bonusu veren casino siteleri: güvenilir casino siteleri
ThomasWhene –
vdcasino: vdcasino
Robertnut –
güvenilir casino siteleri [url=https://cassiteleri.buzz/#]güvenilir casino siteleri[/url]
ThomasWhene –
https://vdcasino1st.online/# vdcasino giris
Robertnut –
https://cassiteleri.buzz/# casino siteleri
Donaldfloak –
https://cassiteleri.top/# deneme bonusu veren casino siteleri
melbet_ruPt –
мелбет пополнение с карты [url=http://melbet39518.help/]http://melbet39518.help/[/url]
ThomasWhene –
vdcasino giris: vdcasino
Robertnut –
casino deneme siteleri: lisanslı casino siteleri
Robertnut –
https://cassiteleri.top/# güvenilir casino siteleri
ThomasWhene –
vdcasino resmi giriş [url=https://vdcasino1st.online/#]vdcasino[/url]
melbet_vsPa –
мелбет скачать на андроид киргизия [url=https://melbet06374.help]мелбет скачать на андроид киргизия[/url]
mostbet_jsSl –
mostbet crash hry [url=http://mostbet2017.help]http://mostbet2017.help[/url]
Robertnut –
lisanslı casino siteleri: lisanslı casino siteleri
ThomasWhene –
vdcasino resmi giriş: vdcasino
mostbet_siPa –
mostbet register [url=www.mostbet85214.help]mostbet register[/url]
mostbet_zgkr –
mostbet kazinoda o‘ynash [url=www.mostbet02894.help]www.mostbet02894.help[/url]
Robertnut –
https://cassiteleri.buzz/# lisanslı casino siteleri
ThomasWhene –
vdcasino giriş: vdcasino
AaronHom –
deneme bonusu veren casino siteleri [url=https://cassiteleri.top/#]lisanslı casino siteleri[/url]
Robertnut –
casino deneme siteleri: casino deneme siteleri
Donaldfloak –
https://cassiteleri.top/# casino siteleri
ThomasWhene –
https://vdcasino1st.online/# vdcasino
Robertnut –
https://cassiteleri.buzz/# casino siteleri
Robertnut –
casino deneme siteleri: lisanslı casino siteleri
Donaldfloak –
casino siteleri [url=https://cassiteleri.buzz/#]casino deneme siteleri[/url]
AaronHom –
casino siteleri: lisanslı casino siteleri
ThomasWhene –
vdcasino: vdcasino
Donaldfloak –
https://cassiteleri.top/# güvenilir casino siteleri
ThomasWhene –
vdcasino resmi: vdcasino
Donaldfloak –
https://cassiteleri.buzz/# casino deneme siteleri
Robertnut –
güvenilir casino siteleri [url=https://cassiteleri.buzz/#]deneme bonusu veren casino siteleri[/url]
ThomasWhene –
vdcasino güncel giriş [url=https://vdcasino1st.blog/#]vdcasino[/url]
Donaldfloak –
https://cassiteleri.top/# lisanslı casino siteleri
Robertnut –
güvenilir casino siteleri [url=https://cassiteleri.buzz/#]casino deneme siteleri[/url]
ThomasWhene –
vdcasino giriş [url=https://vdcasino1st.online/#]vdcasino[/url]
Donaldfloak –
casino siteleri [url=https://cassiteleri.top/#]güvenilir casino siteleri[/url]
Donaldfloak –
casino deneme siteleri [url=https://cassiteleri.top/#]deneme bonusu veren casino siteleri[/url]
ThomasWhene –
vdcasino güncel giriş: vdcasino
mostbet_xhPt –
mostbet oson depozit [url=http://mostbet24618.help/]http://mostbet24618.help/[/url]
Casino_iumi –
В каталоге представлены проверенные провайдеры и актуальные игровые новинки.
[url=https://7v4.casino/]Pinco Casino[/url]
Casino Pinco предлагает честную игру и прозрачные правила.
melbet_oppt –
мелбет букмекерская контора киргизия [url=https://melbet81573.help]https://melbet81573.help[/url]
vavada_xdPr –
jak działa cashback vavada [url=https://vavada56378.help]https://vavada56378.help[/url]
sweet-bonanza_gfen –
sweet bonanza bono para aviator [url=http://sweet-bonanza18364.help/]http://sweet-bonanza18364.help/[/url]
mostbet_kdpi –
мостбет служба поддержки [url=https://mostbet27541.help]https://mostbet27541.help[/url]
melbet_hfsa –
как установить мелбет apk [url=https://melbet36290.help]https://melbet36290.help[/url]
melbet_grOt –
мелбет bypass blocking Тоҷикистон [url=https://melbet20856.help/]https://melbet20856.help/[/url]
Martinbit –
https://mostbetpl.top/# mostbet resmi
Gregoryomiva –
https://mostbetvipaz.buzz/# mostbet
Martinbit –
https://mostbetvipaz.buzz/# mostbet giris
Gregoryomiva –
mostbet kasyno: mostbet
Benniesog –
https://mostbetvipaz.buzz/# mostbet casino
Martinbit –
mostbet güncel: mostbet
plinko_tqkn –
служба поддержки plinko [url=https://plinko61038.help]https://plinko61038.help[/url]
Martinbit –
mostbet: mostbet
Gregoryomiva –
https://mostbettr.icu/# mostbet güncel giriş
Martinbit –
mostbet güncel adres: mostbet
Gregoryomiva –
mostbet güncel giriş: mostbet
Benniesog –
mostbet giris [url=https://mostbettr.icu/#]mostbet[/url]
Martinbit –
mostbet giris: mostbet
Gregoryomiva –
https://mostbetpl.buzz/# mostbet giris
RobertGek –
https://mostbettr.icu/# mostbet güncel
mostbet_aoSn –
mostbet cashback [url=https://mostbet95163.help]mostbet cashback[/url]
sweet-bonanza_cuOi –
як зняти кошти з sweet bonanza на картку [url=https://sweet-bonanza54072.help/]як зняти кошти з sweet bonanza на картку[/url]
Gregoryomiva –
mostbet resmi giriş: mostbet
melbet_xker –
мелбет ставки приложение [url=www.melbet41682.help]www.melbet41682.help[/url]
RobertGek –
https://mostbetpl.buzz/# mostbet
Martinbit –
mostbet güncel giriş [url=https://mostbettr.blog/#]mostbet[/url]
Benniesog –
https://mostbettr.icu/# mostbet güncel giriş
Martinbit –
https://mostbettr.blog/# mostbet
Gregoryomiva –
mostbet giris: mostbet
Martinbit –
mostbet güncel giriş: mostbet
Gregoryomiva –
https://mostbetvipaz.buzz/# mostbet resmi giriş
Martinbit –
mostbet resmi giriş [url=https://mostbetvipaz.buzz/#]mostbet[/url]
Benniesog –
https://mostbettr.icu/# mostbet güncel adres
mostbet_dior –
мостбет актуальное зеркало [url=www.mostbet78063.help]мостбет актуальное зеркало[/url]
Martinbit –
https://mostbetvipaz.buzz/# mostbet güncel adres
Gregoryomiva –
mostbet casino: mostbet
RobertGek –
https://mostbetpl.top/# mostbet casino
mostbet_cupl –
мостбет электронный кошелек [url=https://mostbet21480.help/]мостбет электронный кошелек[/url]
Richardanody –
online pharmacy india: VitalCore Pharmacy – legal online pharmacies in the us
GregoryWrame –
https://vitalcorepharmacy.com/# cheap canadian pharmacy
Patrickgrock –
dog and cat medicine supply: HappyPaws Pharmacy – dog and cat medicine supply
Elmerhaife –
https://vitalcorepharmacy.com/# canadian pharmacy meds
AnthonyBon –
pet pharmacy USA [url=https://happypawspharmacy.shop/#]pet pharmacy USA[/url] pet antibiotics and care
Patrickgrock –
low cost ed meds: True Health Pharm – cheapest online ed treatment
Richardanody –
pet pharmacy: pet pharmacy – pet meds official website
Elmerhaife –
http://happypawspharmacy.com/# dog and cat medicine supply
AnthonyBon –
True Health Pharm [url=https://truehealthpharm.com/#]ed medications cost[/url] True Health Pharm
Patrickgrock –
how to get ed meds online: True Health Pharm – affordable ed medication
Richardanody –
buy erectile dysfunction pills online: True Health Pharm – erectile dysfunction medications online
GregoryWrame –
https://truehealthpharm.shop/# True Health Pharm
melbet_aeKl –
мелбет вход без vpn [url=http://melbet72043.help]мелбет вход без vpn[/url]
Elmerhaife –
https://vitalcorepharmacy.com/# us pharmacy no prescription
Richardanody –
buying prescription drugs from canada: best price for viagra 100mg – ez pharmacy
Patrickgrock –
cheapest ed treatment: True Health Pharm – True Health Pharm
AnthonyBon –
top online pharmacy india [url=https://vitalcorepharmacy.shop/#]VitalCore Pharmacy[/url] cheapest pharmacy prescription drugs
Richardanody –
online pharmacy cialis: viagra without prescription – online pharmacies that use paypal
Elmerhaife –
http://happypawspharmacy.com/# pet antibiotics and care
Patrickgrock –
pet antibiotics and care: pet pharmacy USA – pet antibiotics and care
GregoryWrame –
http://vitalcorepharmacy.com/# thecanadianpharmacy
melbet_cfPl –
melbet официальный сайт ios [url=https://melbet42089.help]https://melbet42089.help[/url]
Richardanody –
ed treatments online: True Health Pharm – True Health Pharm
Patrickgrock –
pet antibiotics and care: pet med – pet antibiotics and care
mostbet_flpa –
mostbet royxatdan otish bepul [url=http://mostbet37150.help]http://mostbet37150.help[/url]
AnthonyBon –
online vet pharmacy [url=http://happypawspharmacy.com/#]pet pharmacy USA[/url] pet antibiotics and care
Elmerhaife –
http://truehealthpharm.com/# True Health Pharm
pinup_psSn –
pinup saytda kirish [url=https://pinup69053.help]pinup saytda kirish[/url]
Richardanody –
pet antibiotics and care: pet antibiotics and care – dog and cat medicine supply
Patrickgrock –
cheapest pharmacy for prescription drugs: Viagra online price – canadianpharmacyworld com
GregoryWrame –
http://truehealthpharm.com/# buy ed meds
Elmerhaife –
https://vitalcorepharmacy.com/# which pharmacy is cheaper
Richardanody –
ed medication online: pills for erectile dysfunction online – where to buy ed pills
AnthonyBon –
low cost ed medication [url=https://truehealthpharm.shop/#]True Health Pharm[/url] True Health Pharm
Patrickgrock –
buying erectile dysfunction pills online: True Health Pharm – ed online prescription
Richardanody –
True Health Pharm: True Health Pharm – True Health Pharm
Elmerhaife –
http://vitalcorepharmacy.com/# online pharmacy no prescription needed
AnthonyBon –
pet meds online [url=https://happypawspharmacy.shop/#]dog medicine[/url] pet pharmacy USA
Richardanody –
canadian pharmacy generic cialis: VitalCore Pharmacy – legit pharmacy websites
GregoryWrame –
https://vitalcorepharmacy.shop/# canadian pharmacy online cialis
Patrickgrock –
True Health Pharm: True Health Pharm – affordable ed medication
Elmerhaife –
https://vitalcorepharmacy.shop/# canadian pharmacy world coupon
mostbet_jiEi –
мостбет ошибка входа в приложение [url=http://mostbet83507.help]http://mostbet83507.help[/url]
Richardanody –
HappyPaws Pharmacy: pet antibiotics and care – dog and cat medicine supply
Patrickgrock –
canadian pharmacy reviews: VitalCore Pharmacy – global pharmacy
AnthonyBon –
True Health Pharm [url=https://truehealthpharm.com/#]order ed pills[/url] True Health Pharm
Richardanody –
True Health Pharm: True Health Pharm – True Health Pharm
Elmerhaife –
https://truehealthpharm.com/# online ed medication
mostbet_ahPi –
mostbet depunere minima [url=www.mostbet2009.help]www.mostbet2009.help[/url]
Patrickgrock –
pet pharmacy USA: pet pharmacy USA – dog and cat medicine supply
Richardanody –
buy erectile dysfunction treatment: how to get ed meds online – True Health Pharm
Elmerhaife –
https://happypawspharmacy.shop/# HappyPaws Pharmacy
Richardanody –
discount ed pills: ed online prescription – order ed pills
AnthonyBon –
HappyPaws Pharmacy [url=http://happypawspharmacy.com/#]dog and cat medicine supply[/url] pet antibiotics and care
Richardanody –
legitimate canadian mail order pharmacy: Viagra online price – my canadian pharmacy
Elmerhaife –
https://vitalcorepharmacy.shop/# buy drugs from canada
GregoryWrame –
http://happypawspharmacy.com/# dog and cat medicine supply
Patrickgrock –
cost of ed meds: True Health Pharm – ed treatment online
Richardanody –
best online pharmacy india: Order Viagra 50 mg online – canadian pharmacy online reviews
mostbet_uzMi –
most bet website [url=mostbet07493.help]mostbet07493.help[/url]
BrianElism –
https://medicobridgerx.shop/# purple pharmacy mexico
PatrickMob –
buy prescription drugs from india: TrustRx India – cheapest online pharmacy india
ThomasCeM –
MedBridge Pharmacy: MedBridge Pharmacy – canada discount pharmacy
mostbet_igEi –
mostbet ставки на теннис Кыргызстан [url=mostbet42395.help]mostbet42395.help[/url]
Anthonysmibe –
https://medicobridgerx.shop/# pharmacy mexico online
DarrenTop –
mexico city pharmacy [url=http://medicobridgerx.com/#]MedicoBridge RX[/url] MedicoBridge RX
BrianElism –
https://medbridgepharmacy.com/# MedBridge Pharmacy
PatrickMob –
reputable indian pharmacies: pharmacy website india – п»їlegitimate online pharmacies india
ThomasCeM –
pharmacy mexico online: MedicoBridge RX – MedicoBridge RX
PatrickMob –
top online pharmacy india: best india pharmacy – top online pharmacy india
ThomasCeM –
canadian pharmacy world coupons: MedBridge Pharmacy – MedBridge Pharmacy
BrianElism –
https://medbridgepharmacy.shop/# medical pharmacy
DarrenTop –
best india pharmacy [url=https://trustrxindia.com/#]TrustRx India[/url] mail order pharmacy india
ThomasCeM –
indian pharmacy online: online shopping pharmacy india – indian pharmacies safe
PatrickMob –
MedBridge Pharmacy: pharmacy canadian superstore – cheapest pharmacy prescription drugs
Anthonysmibe –
https://medicobridgerx.com/# mexican online pharmacies
BrianElism –
https://trustrxindia.shop/# top 10 online pharmacy in india
ThomasCeM –
MedicoBridge RX: MedicoBridge RX – buying prescriptions in mexico
PatrickMob –
MedBridge Pharmacy: canadian online pharmacy reviews – п»їcanadian pharmacy online
DarrenTop –
progreso, mexico pharmacy online [url=https://medicobridgerx.com/#]mexico pharmacy[/url] mexican farmacia
melbet_ceMt –
мелбет техподдержка киргизия [url=https://www.melbet84062.help]мелбет техподдержка киргизия[/url]
ThomasCeM –
MedBridge Pharmacy: canadian mail order pharmacy – MedBridge Pharmacy
PatrickMob –
discount pharmacy: MedBridge Pharmacy – MedBridge Pharmacy
BrianElism –
http://trustrxindia.com/# Online medicine home delivery
Anthonysmibe –
https://medicobridgerx.com/# pharmacy delivery
ThomasCeM –
certified canadian international pharmacy: canadian pharmacy 24h com – precription drugs from canada
DarrenTop –
farmacia mexicana en linea [url=http://medicobridgerx.com/#]MedicoBridge RX[/url] pharmacies in mexico
Leanna –
References:
Does crazy bulk supplements work
References:
https://grenzlandgruen.hier-im-netz.de/Blog;focus=TKOMSI_com_cm4all_wdn_Flatpress_22892279&path=&frame=TKOMSI_com_cm4all_wdn_Flatpress_22892279?x=entry:entry201007-070839%3Bcomments:1
PatrickMob –
mexico pharmacy: medication in mexico – is mexipharmacy legit
Kristen –
References:
Steroids dbol
References:
https://www.grundschulebriesen.de/Startseite/index.php/;focus=STRATP_com_cm4all_wdn_Flatpress_45939558&path=&frame=STRATP_com_cm4all_wdn_Flatpress_45939558?x=entry:entry240305-114539%3Bcomments:1
Devon –
References:
Mass building steroids
References:
https://www.jasminsideenreich.de/Blog/index.php/;focus=STRATP_com_cm4all_wdn_Flatpress_7099662&path=?x=entry:entry181029-140442%3Bcomments:1
ThomasCeM –
mexico online pharmacy: MedicoBridge RX – mexico farmacia
PatrickMob –
MedBridge Pharmacy: canada pharmacy online legit – MedBridge Pharmacy
DarrenTop –
MedBridge Pharmacy [url=https://medbridgepharmacy.shop/#]MedBridge Pharmacy[/url] best canadian online pharmacy reviews
ThomasCeM –
mail order pharmacy india: TrustRx India – indian pharmacy
BrianElism –
https://medbridgepharmacy.shop/# best value pharmacy
Anthonysmibe –
https://medicobridgerx.shop/# pharmacy online
PatrickMob –
MedicoBridge RX: pharmacy in mexico that ships to us – mexican drugstore
Zak –
References:
Short term steroid side effects
References:
http://8.138.192.83:39639/saulecuyer8501
Ronny –
References:
Is short term prednisone use dangerous
References:
http://180.163.77.12:3000/mellisaguizar1
pinup_tcEl –
pin-up rasmiy ko‘zgusi [url=pinup35741.help]pin-up rasmiy ko‘zgusi[/url]
Laurel –
References:
Where is crazy bulk located
References:
http://122.116.190.233:3001/errolcaban658/4865jobshop24.com/wiki/Dianabol-Dbol-Guide-Dosage%2C-Half-Life-%26-Side-Effects
ThomasCeM –
pharmacy discount coupons: MedBridge Pharmacy – MedBridge Pharmacy
DarrenTop –
MedBridge Pharmacy [url=http://medbridgepharmacy.com/#]MedBridge Pharmacy[/url] reputable online pharmacy
PatrickMob –
indian pharmacies safe: TrustRx India – best online pharmacy india
ThomasCeM –
MedicoBridge RX: MedicoBridge RX – progreso, mexico pharmacy online
PatrickMob –
MedicoBridge RX: MedicoBridge RX – pharmacia mexico
Gita –
References:
2ahukewipubipvmvnahuy7p4khwr8cqaq4lyoanoecaeqfw|the best steroids for muscle growth
References:
https://www.fcla.de/index.php/;focus=STRATP_com_cm4all_wdn_Flatpress_38266970&path=?x=entry:entry251219-071747%3Bcomments:1
ThomasCeM –
pharmacy website india: TrustRx India – pharmacy website india
pqanpmttx –
암호화폐 카지노에서는 수백 개 또는 수천 개의 비트코인 슬롯이 전용 탭에 준비되어 있습니다. 테마, 기능, 인기도별로 필터링하여 원하는 슬롯을 찾을 수 있습니다. 저희가 이 리뷰에서 추천하는 슬롯은 신뢰할 수 있는 제공업체의 최고 암호화폐 슬롯들입니다. 관련 슬롯은 게임소개 전체보기에 수록되어 있습니다.무료 플레이는 프라그마틱 무료체험에서 가능합니다. 라이즈 오브 올림푸스 100 온라인 슬롯의 와일드 심볼은 다른 모든 심볼을 대체하여 승리 조합을 구성합니다. 와일드 심볼은 특히 세 개의 심볼로 이루어진 승리가 떨어질 때 중간에 나타납니다. 또한 캐스케이드 후 그리드에 와일드를 제외한 더 이상 기호가 남아있지 않으면 지워집니다.
https://tsrstreetwear.com/gate-of-olympus-max-bet/
You have viewed 0 of 0 games! 2. Play Store에서 Gate As Olypuls(을)를 다운로드 받습니다 컴퓨터에서 Zeus Gates(을)를 실행하면 보다 큰 화면에서 이용할 수 있으며, 마우스와 키보드로 앱을 이용하는 것이 화면을 터치하는 것보다 훨씬 빠릅니다. 동시에 기기의 배터리 문제에 대해 걱정할 필요가 없습니다. Gates of Olympus Gates of Olympus Einbauküche, offene Küche, Kücheninsel, Pantry-Küche, oder nur eine Arbeitsplatte… 마우스 커서를 올리면이미지 순서를 ON OFF 할 수 있습니다. 컴퓨터에서 Zeus Gates(을)를 실행하면 보다 큰 화면에서 이용할 수 있으며, 마우스와 키보드로 앱을 이용하는 것이 화면을 터치하는 것보다 훨씬 빠릅니다. 동시에 기기의 배터리 문제에 대해 걱정할 필요가 없습니다.
Anthonysmibe –
https://medbridgepharmacy.com/# MedBridge Pharmacy
PatrickMob –
tijuana pharmacy online: MedicoBridge RX – MedicoBridge RX
ThomasCeM –
MedicoBridge RX: order meds from mexico – mexican pharmacies online
ldbbcuoux –
Back to back offer, Holiday Offer, PONANT Bonus 15% Wins are multiplied in base and Free Games The game is accessible via all portable and non-portable devices, as well as representatives of the animal world living in those parts. Our team is mixed, as well as that all the bonuses are offered by fair and reliable casinos. Players can find all their products from the navigation tab at the top right corner of every page, keep in mind that youre competing against other players. Play for free 15 dragon pearls free spins no deposit not only does Sloty Casino have more than 1,000 games, all of whom are just as eager as you are to win a piece of the prize pool. About Us Contacts Policy Privacy Policy Sitemap Terms & Conditions · Flights Darwin Bamurru Plains round-trip with a luggage allowance of one 15kg piece.
https://rideonrental.com/class777-casino-online-casino-platform-review-for-australian-players/
That doesn’t mean there’s anything wrong with Gates of Olympus Xmas 1000. Certainly, if you’re a fan of scatter pays games like this and fancy a festive version to get you in the Christmas spirit, it’s one of the better options out there – especially since we’re sticking with the ‘1000’ aspect. Following in the footsteps of its predecessor, which became one of the world’s best online slot games, Gates of Olympus 1000 takes you on a magical journey through ancient Greece, where gods guard precious treasures. Whether you are an experienced player or just starting with slot games, Gates of Olympus 1000 will amaze you. The spectacular visuals will make you feel like you are on Olympus. The effects and visuals take you to unforgettable realms of ancient Greece.
fsmedmkzh –
There was an error while loading. Please reload this page. You can submit new cheats for this game and help our users gain an edge. Dichos campos establecen la cantidad de veces que las jugadores poseen instalar el monto de el bono desprovisto lograr eximir 50 tiradas gratis en Book of Ra Trucos las ganancias generadas con manga larga bocamanga extendida él. Por ejemplo, si el carga de postura sería sobre 30 ocasiones nuestro monto del bono, así como nuestro bono sería sobre cincuenta€, los jugadores poseen situar algún entero de 1500€ falto sacar apartar los ganancias. Bastantes jugadores inscribirí¡ frustran alrededor mirar que nunca podrán apartar los ganancias con facilidad. La plataforma se destaca por su variada oferta de temáticas y proveedores, así como por su gran ratio de pago, que se traduce en múltiples probabilidades de ganar.
https://avaliacao.vitormadureira.com.br/2026/03/11/sharing-the-lucky-ones-casino-experience-in-new-zealand/
Splice is a powerful mobile video editor designed to meet the needs of both professional content creators and beginners. This app brings the capabilities of a desktop editor to your phone, allowing you to create and share stunning videos effortlessly. With its intuitive interface and advanced features, Splice is perfect for producing professional-quality videos that stand out on social media. Level up your video’s appeal with stunning transtions. In the realm of video editing, Vivid Glam rises above the rest as the paramount choice for both beginners and professionals alike. This remarkable app is readily available for free download on the App Store, and it redefines the way you approach video editing. Vivid Glam is your gateway to crafting captivating, professional-quality videos with unparalleled ease and precision.
Laurene –
References:
Anabolic steroid withdrawal symptoms
References:
https://servus-nachbar.at/Neuigkeiten/index.php/;focus=W4YPRD_com_cm4all_wdn_Flatpress_7491266&path=&frame=W4YPRD_com_cm4all_wdn_Flatpress_7491266?x=entry:entry250616-190613%3Bcomments:1
PatrickMob –
buy medicines online in india: india pharmacy – mail order pharmacy india
ThomasCeM –
can i order online from a mexican pharmacy: mexican pharmacies that ship to the united states – MedicoBridge RX
PatrickMob –
pharmacy mexico: MedicoBridge RX – los algodones pharmacy online
mostbet_zlMr –
mostbet születésnapi bónusz [url=https://www.mostbet2021.help]https://www.mostbet2021.help[/url]
ThomasCeM –
MedBridge Pharmacy: reputable online pharmacy reddit – MedBridge Pharmacy
Anthonysmibe –
http://medicobridgerx.com/# farmacia mexicana en linea
PatrickMob –
indian pharmacy online: best online pharmacy india – best india pharmacy
ThomasCeM –
MedicoBridge RX: п»їmexican pharmacy – MedicoBridge RX
PatrickMob –
online mexico pharmacy: MedicoBridge RX – mexican pharmacies online
ThomasCeM –
MedicoBridge RX: farmacia online usa – medicine mexico
PatrickMob –
world pharmacy india: online pharmacy india – online pharmacy india
ThomasCeM –
MedicoBridge RX: MedicoBridge RX – MedicoBridge RX
EdwardPrido –
https://corevitalpharmacy.com/# Cialis 20mg price in USA
MichaelJah –
http://primelinepharmacy.com/# online ed prescription
Arthurswoms –
best online ed meds: ed pills pharmacy – ed rx online
HectorLoala –
NovaMen Pharmacy: generic sildenafil – NovaMen Pharmacy
bmynbjstf –
De nombreux casinos partenaires proposent Gates of Olympus casino. Nous vous présentons la meilleure offre de notre classement. Consultez les promotions disponibles pour maximiser vos gains. Sweet Bonanza to jeden z najpopularniejszych slotów od Pragmatic Play, który podobnie jak „Gates of Olympus” oferuje mechanikę Tumble oraz system wypłat bez tradycyjnych linii. Gra osadzona w kolorowej, cukierkowej scenerii, przyciąga graczy nie tylko estetyką, ale także możliwością zdobycia dużych wygranych dzięki multiplikatorom i funkcji darmowych spinów. Te bezpłatne gry hazardowe oferują graczom nowoczesną grafikę, wysoką jakość obrazu i animacji. W rezultacie gra jest nie tylko interesująca z punktu widzenia interaktywności, ale również atrakcyjna wizualnie. Pierwsze trójwymiarowe sloty zaczęły pojawiać się już w latach 2000. i bardzo szybko zdobyły popularność właśnie dzięki swojej warstwie graficznej. Jeśli planujesz rozpoczęcie dalszej gry w tego typu sloty, polecamy zwrócić uwagę na następujące tytuły:
https://india4u.eu/bizzo-casino-recenzja-dla-graczy-z-polski/
Gry za darmo kasyno baccarat to gra, będziesz mógł korzystać ze wszystkich najpopularniejszych rozwiązań bankowych i wypłacić do 40 000 EUR miesięcznie. Mimo to gracze mogą polegać na witrynach do gier z innych rynków regulowanych w celu zapewnienia uczciwej gry i innych usług kasynowych, co pozwala graczom na długą sesję gry. Pamiętaj, w zależności od tego. Kiedy tak się dzieje, ponieważ jest pokryta ikonami tematycznymi. niedziela 14.09.2025 Dowód istnienia danego bytu leży po stronie dowodzącej istnienie tegoż. Inaczej dochodzimy do absurdu (vide: czajniczek Russela, Latający Potwór Spaghetti; Hartmański Kubuś Puchatek nie jest wcale tak oryginalnym wymysłem). Z drugiej strony wszyscy mamy jakieś przyjmowane bez dowodu przekonania na świat. Jedni wierzą w boga bogów w takiej czy innej formie i liczbie, inni w siły nadprzyrodzone. A niektórzy w żadne. Było tak zawsze, także w średniowieczu rządzonym przez Kościół. Którego luminarze jednak o tym nie wspominają, skarżąc się na niespotykany i nagły upadek wiary.
EdwardPrido –
https://novamenpharmacy.com/# NovaMen Pharmacy
Arthurswoms –
NovaMen Pharmacy: NovaMen Pharmacy – NovaMen Pharmacy
HectorLoala –
how to get ed pills: ed pills pharmacy – low cost ed pills
EdwardPrido –
https://primelinepharmacy.shop/# discount ed meds
HectorLoala –
cheap ed medicine: buy ed medication online – cost of ed meds
MichaelJah –
https://corevitalpharmacy.shop/# Cialis 20mg price
Arthurswoms –
sildenafil online: Viagra online price – buy viagra here
HectorLoala –
buy ed meds online: PrimeLine Pharmacy – ed treatment online
EdwardPrido –
http://corevitalpharmacy.com/# Cialis 20mg price
mostbet_tkEt –
mostbet ios quraşmır [url=mostbet2013.help]mostbet2013.help[/url]
melbet_egPr –
melbet problema site [url=melbet63048.help]melbet63048.help[/url]
HectorLoala –
Buy generic 100mg Viagra online: NovaMen Pharmacy – NovaMen Pharmacy
EdwardPrido –
https://novamenpharmacy.shop/# NovaMen Pharmacy
mostbet_ijen –
mostbet Oʻzbekistonda to‘lov [url=www.mostbet73618.help]mostbet Oʻzbekistonda to‘lov[/url]
Arthurswoms –
Cheap generic Viagra online: NovaMen Pharmacy – generic sildenafil
HectorLoala –
how to get ed pills: PrimeLine Pharmacy – cheap ed meds online
MichaelJah –
http://corevitalpharmacy.com/# CoreVital Pharmacy
EdwardPrido –
https://novamenpharmacy.com/# NovaMen Pharmacy
HectorLoala –
cheap ed pills: PrimeLine Pharmacy – ed meds cheap
Arthurswoms –
sildenafil over the counter: sildenafil 50 mg price – NovaMen Pharmacy
EdwardPrido –
http://primelinepharmacy.com/# online ed treatments
HectorLoala –
ed online treatment: ed pills pharmacy – online ed meds
Arthurswoms –
sildenafil 50 mg price: sildenafil 50 mg price – best price for viagra 100mg
Casino_evmi –
https://nmgazeta.ru/nmnews/2783885/zenit-i-spartak-gotovyatsya-k-glavnomu-matchu-tura-rpl.html
HectorLoala –
Cheapest Sildenafil online: NovaMen Pharmacy – NovaMen Pharmacy
EdwardPrido –
http://novamenpharmacy.com/# Generic Viagra for sale
MichaelJah –
https://primelinepharmacy.shop/# where to get ed pills
Arthurswoms –
Cheap Cialis: Buy Tadalafil 10mg – CoreVital Pharmacy
HectorLoala –
CoreVital Pharmacy: CoreVital Pharmacy – cheapest cialis
EdwardPrido –
https://novamenpharmacy.com/# NovaMen Pharmacy
mostbet_kyEr –
мостбет баланс [url=http://mostbet05638.help]http://mostbet05638.help[/url]
Arthurswoms –
NovaMen Pharmacy: over the counter sildenafil – NovaMen Pharmacy
HectorLoala –
generic sildenafil: Generic Viagra online – Viagra without a doctor prescription Canada
EdwardPrido –
http://corevitalpharmacy.com/# Cialis without a doctor prescription
Arthurswoms –
buy viagra here: NovaMen Pharmacy – NovaMen Pharmacy
MichaelJah –
http://novamenpharmacy.com/# NovaMen Pharmacy
HectorLoala –
buy erectile dysfunction medication: online erectile dysfunction prescription – how to get ed pills
EdwardPrido –
http://corevitalpharmacy.com/# CoreVital Pharmacy
Arthurswoms –
Generic Viagra online: NovaMen Pharmacy – NovaMen Pharmacy
HectorLoala –
best price for viagra 100mg: NovaMen Pharmacy – cheap viagra
EdwardPrido –
https://primelinepharmacy.shop/# cheap ed drugs
Arthurswoms –
NovaMen Pharmacy: NovaMen Pharmacy – sildenafil online
HectorLoala –
NovaMen Pharmacy: NovaMen Pharmacy – NovaMen Pharmacy
MichaelJah –
https://corevitalpharmacy.shop/# Cheap Cialis
EdwardPrido –
https://primelinepharmacy.shop/# ed medications online
Richardfut –
jojobet güncel adres [url=https://jojovip.top/#]jojobet[/url]
Casino_yhmi –
https://maps.google.ae/url?sa=t&url=https://www.komoot.com/user/5592829740548
EdwardPrido –
https://primelinepharmacy.shop/# ed online meds
Stevenmup –
https://jojovip.top/# jojobet güncel giriş
Richardfut –
jojobet casino: jojobet
EdwardPrido –
https://novamenpharmacy.com/# Viagra online price
MichaelJah –
http://corevitalpharmacy.com/# CoreVital Pharmacy
AnthonyDiz –
https://pharmacologicalsciences.com/ cialis
Whitneygrode –
buy ed meds online Pharmacological Institute online ed prescription
Williamvut –
https://novamenpharmacy.com/# NovaMen Pharmacy
AnthonyDiz –
https://pharmacologicalsciences.com/edpills.html viagra
Whitneygrode –
erectile dysfunction medications online Pharmacological Institute ed meds on line
Williamvut –
http://novamenpharmacy.com/# NovaMen Pharmacy
DewayneElurf –
https://pharmacologicalsciences.com/ Pharmacological Sciences Research Institute
Williamvut –
https://primelinepharmacy.com/# erectile dysfunction online prescription
AnthonyDiz –
https://pharmacologicalsciences.com/ ed pills
Whitneygrode –
cheapest ed pills Pharmacological Sciences Research Institute online erectile dysfunction prescription
Williamvut –
http://primelinepharmacy.com/# where can i buy ed pills
AnthonyDiz –
https://pharmacologicalsciences.com/generics.html cialis
RudolphSteak –
Quand j’utilise [url=https://staxino-casino-888.fr/]https://www.staxino-casino-888.fr/[/url] je fais direct attention a la liste des slots et aux jeux mis en avant. Je prefere les plateformes ou tout est accessible en quelques clics. La rapidite est aussi super importante. Une bonne experience passe par la simplicite.
DewayneElurf –
https://pharmacologicalsciences.com/cialis.html kamagra
Whitneygrode –
erectile dysfunction drugs online Pharmacological Sciences Research Institute buy ed meds
Williamvut –
https://primelinepharmacy.shop/# cheapest erectile dysfunction pills
AnthonyDiz –
https://pharmacologicalsciences.com/edpills.html Pharmacological Sciences Research Institute
AnthonyDiz –
https://pharmacologicalsciences.com/edpills.html ed pills
Casino_upmi –
https://matras-promtex.ru/
Williamvut –
http://novamenpharmacy.com/# NovaMen Pharmacy
AnthonyDiz –
https://pharmacologicalsciences.com/ Pharmacological Institute
AnthonyDiz –
https://pharmacologicalsciences.com/ Pharmacological Sciences
Williamvut –
https://novamenpharmacy.shop/# NovaMen Pharmacy
AnthonyDiz –
https://pharmacologicalsciences.com/viagra.html viagra
Williamvut –
https://primelinepharmacy.shop/# ed online meds
Whitneygrode –
cheap ed treatment Pharmacological Institute cheap ed drugs
AnthonyDiz –
https://pharmacologicalsciences.com/viagra.html viagra
DewayneElurf –
https://pharmacologicalsciences.com/cialis.html levitra
AnthonyDiz –
https://pharmacologicalsciences.com/cialis.html levitra
Williamvut –
https://primelinepharmacy.com/# cheap ed meds
Whitneygrode –
best ed medication online Pharmacological Sciences ed pills cheap
Whitneygrode –
ed meds by mail Pharmacological Sciences Research Institute boner pills online
Williamvut –
https://primelinepharmacy.shop/# erection pills online
AndreamUth –
Pharmacological Institute [url=https://pharmacologicalsciences.com/#]Pharmacological Sciences Research Institute[/url] cialis
Whitneygrode –
online ed pills Pharmacological Sciences Research Institute low cost ed pills
RickyChini –
pin up kz вход: pin up
EdwardFeX –
pin-up казино играть: pin up
Williamvut –
https://corevitalpharmacy.com/# CoreVital Pharmacy
RickyChini –
pin up [url=http://ugtk.kz/#]pin up[/url]
Whitneygrode –
buy ed medication Pharmacological Sciences cheap ed pills online
Williamvut –
https://novamenpharmacy.com/# Viagra online price
Whitneygrode –
online ed prescription Pharmacological Sciences ed medicines
RickyChini –
pin up: pin up
Whitneygrode –
cheapest online ed meds Pharmacological Institute order ed meds online
Williamvut –
https://novamenpharmacy.shop/# NovaMen Pharmacy
RickyChini –
pin up [url=https://pinupkz.online/#]pin up[/url]
Whitneygrode –
best ed medication online Pharmacological Institute order ed pills online
RickyChini –
pin up kz вход: pin up
Richardmog –
generic antibiotics online cheap OTC antibiotics prescribed antibiotics online
Ronaldcon –
https://antimicrobialresearch.com/cipro.html Doxycycline Hyclate
Williambut –
[url=https://antimicrobialresearch.com/doxycycline.html#]Ciprofloxacin Hydrochloride[/url] buy antibiotics over the counter
RalphErync –
buy antibiotics over the counter Antibiotics Pharmacology get antibiotics quickly
Ronaldcon –
https://antimicrobialresearch.com/zithromax.html OTC antibiotics
Richardmog –
antibiotic without presription Sulfamethoxazole Trimethoprim buy antibiotics for sinus
Williambut –
[url=https://antimicrobialresearch.com/cipro.html#]Antibiotics Pharmacology[/url] otc uti medicine
RalphErync –
antibiotics for uti OTC antibiotics buy doxycycline antibiotics
Ronaldcon –
https://antimicrobialresearch.com/cipro.html Doxycycline Hyclate
Louispab –
https://antimicrobialresearch.com/bactrim.html antibiotics
Richardmog –
cheapest antibiotics Sulfamethoxazole Trimethoprim antibiotics online pharmacy
iqpluszxp –
Når du kjøper bonusspillet kan du velge om du vil utløse bonusrunden med minst 3, 4, 5 eller 6 scatter. Antallet scattersymboler du får, eller betaler for, gir deg ulikt antall gratisspinn, fra 7 til 19. Med en Bonus Buy-kostnad mellom 60x og 250x grunninnsatsen din kan du kjøpe funksjonen for mellom 60 kr og 250.000 kr. Jackpotspill Gates of Olympus This website is using a security service to protect itself from online attacks. The action you just performed triggered the security solution. There are several actions that could trigger this block including submitting a certain word or phrase, a SQL command or malformed data. Før du setter i gang med å spille, er det greit å justere innsatsen etter budsjett og risikovilje. På Gates of Olympus kan du enkel justere hvor mye penger som skal satses per runde, ved å trykke på pluss og minus på konsollen.
https://luminahavenwellnesshub.co.ke/de-beste-revolut-casino-online-spillene/
Gates of Olympus gratis spill er mer enn mulig. Prøv det ut før du begynner å satse ekte penger. Dette er den enkleste og mest rasjonelle måten å forstå oppsettet og funksjonene til dette spillet på. Gates of Olympus, utviklet av Pragmatic Play, tilbyr en fengslende blanding av høy volatilitet, engasjerende mekanikker og fantastisk grafikk, alt satt i den mytiske verdenen til greske guder. Med sitt 6×5 rutenettlayout, kaskaderende hjul og høye multiplikatorer gir spillet en spennende og dynamisk opplevelse. Lyden og musikken forsterker den episke følelsen ytterligere, og gjør hvert spinn til et storslått eventyr. De fleste historiene i spill med gresk tema inneholder heroiske oppdrag og ikoniske gudekamper. Ta lynet og start den olympiske historien med disse spillene med gresk tema:
Narkologicheskaya klinika Trezvii vibor_smKn –
клиника наркологическая платная [url=https://narkologicheskaya-klinika-trezvyj-vybor.ru/]клиника наркологическая платная[/url] .
Williambut –
[url=https://antimicrobialresearch.com/cipro.html#]Azithromycin Dihydrate[/url] buy antibiotics from canada
Richardmog –
generic antibiotics online cheap OTC antibiotics antibiotics over the counter
Ronaldcon –
https://antimicrobialresearch.com/otc-antibiotics.html Amoxicillin Trihydrate
Richardmog –
generic antibiotics Doxycycline Hyclate generic antibiotics online cheap
Louispab –
https://antimicrobialresearch.com/cipro.html antibiotics
RalphErync –
get antibiotics without seeing a doctor OTC antibiotics buy antibiotics online
Ronaldcon –
https://antimicrobialresearch.com/zithromax.html antibiotics
Williambut –
[url=https://antimicrobialresearch.com/bactrim.html#]Ciprofloxacin Hydrochloride[/url] antibiotics for uti
Richardmog –
antibiotics drugs antibiotics buy antibiotics online safely
Ronaldcon –
https://antimicrobialresearch.com/doxycycline.html Antibiotics Pharmacology
RalphErync –
antibiotics for uti Sulfamethoxazole Trimethoprim antibiotics drugs
Richardmog –
buy antibiotics from india OTC antibiotics buy antibiotics online safely
Williambut –
[url=https://antimicrobialresearch.com/cipro.html#]Doxycycline Hyclate[/url] get antibiotics without seeing a doctor
Richardmog –
antibiotic without presription Doxycycline Hyclate cheap antibiotics
Ronaldcon –
https://antimicrobialresearch.com/cipro.html IARP
RalphErync –
cheap antibiotics Ciprofloxacin Hydrochloride best online doctor for antibiotics
Williambut –
[url=https://antimicrobialresearch.com/#]Azithromycin Dihydrate[/url] buy antibiotics from canada
Richardmog –
online antibiotics Antibiotics Pharmacology online antibiotics
Ronaldcon –
https://antimicrobialresearch.com/otc-antibiotics.html IARP
Louispab –
https://antimicrobialresearch.com/zithromax.html antibiotics
Richardmog –
buy antibiotics for sinus Antibiotics Pharmacology Over the counter antibiotics for infection
Williambut –
[url=https://antimicrobialresearch.com/cipro.html#]Sulfamethoxazole Trimethoprim[/url] Over the counter antibiotics for infection
bzlfubtju –
Gates of Hades offers a fresh spin on the familiar Gates of Olympus formula, making it a solid choice for fans of the series. iSoftBet bietet eine überlegene Auswahl an erstklassigen Inhalten mit Megaways™ und Hold & Win-Funktionen an, die ein grossartiges Benutzererlebnis für die Spieler ermöglichen. Soft decline, SCA notwendig Werden vier oder mehr Scatter irgendwo auf den Walzen getroffen, so werden die Freispiele freigeschalten. Zu Beginn werden den Spielern 15 Freispiele zugestanden. Und immer wenn die Vervielfachungssymbole während der Freispielfunktion auf den Walzen erscheinen, wird der Multiplikatorenwert zum Gesamtmultiplikator addiert. Ob adjust Hase im Casinogeschäft oder Anfänger, jeder nach göttlicher Vergnügen sucht – Gates of Olympus bietet für jeden dasjenige Richtige. Mit einer reizvollen RTP von 96, 5% ebenso flexiblen Einstellungsoptionen werden Sie sich fühlen, als hätten die Götter dieses Spiel nur für Sie erschaffen. Sie können Gates of Olympus kostenlos spielen, geradeaus hier, ohne Anmeldung, Einzahlung oder jegliches Risiko. Der Position hat einen RTP Wert von ninety six, 5% und viele hohe Volatilität.
https://xtremepape.rs/members/loganturner.654084/#about
Beyond the bonus features, Gates of Olympus also boasts a unique ‘All Ways Pay’ system. Instead of traditional paylines, the game awards payouts for combinations of 8 or more matching symbols anywhere on the reels. This creates numerous opportunities for wins and makes every spin an exciting prospect. Free spins in online slots are a thrilling feature that can enhance your gaming experience, offering the chance to win without placing additional bets. To activate them, particularly in the “Gates of Olympus” slot by Pragmatic Play, you usually need to land a certain number of scatter symbols on the reels within a single spin. Typically, this symbol is represented by an icon integral to the game’s theme – in the case of Gates of Olympus, it might feature a Greek mythology figure.
Ronaldcon –
https://antimicrobialresearch.com/bactrim.html Antibiotics Pharmacology
bugjlsdwu –
Finally, note that all the high stakes roulette games listed here are live-dealer or auto-wheel games, not RNG (computer-generated). Live tables usually allow bigger limits since exposure is managed with staffed studios, pacing, and VIP oversight. RNG versions often cap lower because they run faster and around the clock. Finally, note that all the high stakes roulette games listed here are live-dealer or auto-wheel games, not RNG (computer-generated). Live tables usually allow bigger limits since exposure is managed with staffed studios, pacing, and VIP oversight. RNG versions often cap lower because they run faster and around the clock. For those exploring strategies, the super stake roulette free play option offered at partner casinos allows practice without real stakes. Once confident, players can move into live sessions of super roulette 5000x with real money for a chance to secure the maximum win of €250,000.
https://www.posme.co.in/teen-patti-live-dealer-an-exciting-casino-game-experience-for-pakistani-players/
Aloha! Cluster Pays is a somewhat different but enjoyable slot. It took some time to get used to, but has grown on us and is now one of our favourite Netent slots. On the playing field there may be the pay combinations of 9 – 30 matching symbols: There are some nice added features in the game that will help boost overall payouts. From wilds to bonus rounds, Aloha! Cluster Pays can be a very rewarding slot selection. The Ice Casino bonus for new players is a good offer, the steps in collecting the bonus remain the same. With up to 1,000,000 winning ways, whether you want to play on your own or with our charming live dealers. The calculated maximum multiplier for this game is 2023x, some casinos may charge a small fee for withdrawals. The Cluster pay feature which means that the same symbols can form a winning combination horizontally or vertically. Collecting at least 9 symbols of a cluster gives you a special prize.
Richardmog –
can you buy antibiotics over the counter Azithromycin Dihydrate buy antibiotics online
Ronaldcon –
https://antimicrobialresearch.com/ OTC antibiotics
Williambut –
[url=https://antimicrobialresearch.com/otc-antibiotics.html#]Azithromycin Dihydrate[/url] prescribed antibiotics online
Louispab –
https://antimicrobialresearch.com/cipro.html Ciprofloxacin Hydrochloride
Richardmog –
buy zithromax antibiotic Amoxicillin Trihydrate uti antibiotics online
RalphErync –
Over the counter antibiotics for infection Azithromycin Dihydrate prescribed antibiotics online
Ronaldcon –
https://antimicrobialresearch.com/cipro.html Antibiotics Pharmacology
RalphErync –
generic antibiotics online cheap Antibiotics Pharmacology antibiotics over the counter
Williambut –
[url=https://antimicrobialresearch.com/amoxil.html#]Amoxicillin Trihydrate[/url] uti antibiotics online
mostbet_twoi –
mostbet link [url=https://mostbet16734.help/]mostbet link[/url]
mostbet_cner –
mostbet купон ставок [url=https://www.mostbet2029.help]https://www.mostbet2029.help[/url]
mostbet_uyoi –
mostbet mines game [url=https://mostbet16082.help/]https://mostbet16082.help/[/url]
Richardmog –
antibiotics over the counter Doxycycline Hyclate best online doctor for antibiotics
mostbet_jiei –
mostbet вейҷер бонус [url=https://www.mostbet07482.help]https://www.mostbet07482.help[/url]
melbet_kgPl –
как вывести с мелбет [url=http://melbet08561.help]http://melbet08561.help[/url]
RalphErync –
generic antibiotics online pharmacy Ciprofloxacin Hydrochloride cheapest antibiotics
Ronaldcon –
https://antimicrobialresearch.com/bactrim.html Sulfamethoxazole Trimethoprim
Stevefaula –
reliable mexican pharmacies [url=https://bordercarerx.com/#]BorderCare RX[/url] mexico farmacia
MichaelWhoms –
legit mexican pharmacy without prescription: reliable mexican pharmacies – BorderCareRX
MatthewTruri –
NorthCareRx: medication canadian pharmacy – canada discount pharmacy
Edwardevott –
http://bordercarerx.com/# BorderCare RX
melbet_gept –
мелбет коэффициенты [url=http://melbet18207.help]мелбет коэффициенты[/url]
MichaelWhoms –
best online pharmacy usa: п»їlegitimate online pharmacies india – safe online pharmacy
MatthewTruri –
NorthCareRx: NorthCareRx – canadian pharmacy world
Edwardevott –
https://primeindiameds.com/# best online pharmacy
Stevefaula –
NorthCareRx [url=https://northcarerx.com/otc.php#]canadian king pharmacy[/url] NorthCareRx
Phillipciz –
https://primeindiameds.com/# canadian pharmacies comparison
MichaelWhoms –
cheapest online pharmacy india: top 10 pharmacies in india – legit online pharmacy
MatthewTruri –
canadian pharmacy viagra 50 mg: Prime India Meds – best online pet pharmacy
Edwardevott –
https://primeindiameds.com/# cialis online pharmacy
MatthewTruri –
mexico pharmacies online: BorderCareRX – legit mexican pharmacy without prescription
Stevefaula –
canadian pharmacy online ship to usa [url=https://northcarerx.com/ed-pills.php#]NorthCareRx[/url] canadian drug pharmacy
Arthurcaurb –
Globalement sur [url=https://dragonia-casino-101.fr]dragonia casino[/url] je regarde surtout les slots et la structure du site. Je prefere quand tout est logique et rapide a parcourir. Sur telephone c’est encore plus important. Une interface claire rend tout plus agreable.
Edwardevott –
https://primeindiameds.com/# pharmacy com canada
Phillipciz –
http://bordercarerx.com/# BorderCare RX
MatthewTruri –
canadian pharmacies comparison: canadian pharmacy 24h com safe – NorthCareRx
Edwardevott –
https://primeindiameds.shop/# best india pharmacy
MatthewTruri –
cheapest pharmacy to fill prescriptions without insurance: Prime India Meds – canadian pharmacy cialis
Stevefaula –
best canadian pharmacy [url=https://northcarerx.shop/#]canadian pharmacy antibiotics[/url] NorthCareRx
Edwardevott –
https://northcarerx.com/otc.php# canadian pharmacy ratings
MatthewTruri –
canadian pharmacy drugs online: Prime India Meds – canadian pharmacy meds
Phillipciz –
https://bordercarerx.shop/# BorderCareRX
Stevefaula –
canadian online drugstore [url=https://northcarerx.com/#]canadian pharmacy online[/url] NorthCareRx
Edwardevott –
https://primeindiameds.shop/# online pharmacy same day delivery
MatthewTruri –
reputable pharmacies in mexico: legit mexican pharmacy without prescription – reliable mexican pharmacies
Edwardevott –
https://northcarerx.shop/# canadian world pharmacy
MatthewTruri –
legit mexican pharmacy without prescription: mexico pharmacies online – BorderCare RX
Stevefaula –
canadian king pharmacy [url=https://primeindiameds.shop/#]best online pharmacy india[/url] pill pharmacy
MatthewTruri –
NorthCareRx: NorthCareRx – canadian pharmacy king
Edwardevott –
http://bordercarerx.com/# mexico pharmacies online
Phillipciz –
http://primeindiameds.com/# canada discount pharmacy
MichaelWhoms –
BorderCare RX: mexico pharmacies online – BorderCare RX
MatthewTruri –
canadian pharmacy oxycodone: is canadian pharmacy legit – canadian drugs online
Edwardevott –
https://bordercarerx.shop/# legit mexican pharmacy without prescription
Stevefaula –
vipps canadian pharmacy [url=https://northcarerx.com/ed-pills.php#]ed drugs online from canada[/url] legit canadian pharmacy online
plinko_brsa –
plinko ставка минимальная [url=www.plinko50862.help]www.plinko50862.help[/url]
MichaelWhoms –
online pharmacy com: Prime India Meds – cialis canada online pharmacy
MatthewTruri –
canadian pharmacy king: NorthCareRx – NorthCareRx
Edwardevott –
https://bordercarerx.com/# BorderCareRX
Aurora –
References:
Bodybuilding muscle names
References:
https://uznove.uz/user/relishdad1/
sweet-bonanza_xiEa –
sweet bonanza bono recarga méxico [url=http://sweet-bonanza72501.help/]http://sweet-bonanza72501.help/[/url]
Phillipciz –
https://northcarerx.shop/# vipps approved canadian online pharmacy
MatthewTruri –
NorthCareRx: NorthCareRx – canadian drug prices
Stevefaula –
www pharmacyonline [url=http://primeindiameds.com/#]top 10 pharmacies in india[/url] canadian pharmacy 24 com
Edwardevott –
https://primeindiameds.com/# canadian pharmacies not requiring prescription
MichaelWhoms –
medical mall pharmacy: indian pharmacy online – medical mall pharmacy
MatthewTruri –
canadapharmacyonline legit: canadian pharmacy ltd – onlinecanadianpharmacy 24
Edwardevott –
https://bordercarerx.com/# mexican pharmacies no prescription
Stevefaula –
hydrocodone mexico pharmacy [url=https://bordercarerx.com/#]BorderCareRX[/url] BorderCare RX
pinup_whOn –
pin-up Oʻzbekiston Apelsin [url=http://pinup52914.help]http://pinup52914.help[/url]
MichaelWhoms –
recommended canadian pharmacies: Prime India Meds – online pharmacy 365 pills
MatthewTruri –
NorthCareRx: canadian discount pharmacy – NorthCareRx
Phillipciz –
http://primeindiameds.com/# my canadian pharmacy review
Edwardevott –
https://bordercarerx.shop/# BorderCareRX
melbet_zfor –
melbet зеркало бишкек [url=www.melbet76521.help]www.melbet76521.help[/url]
sweet-bonanza_jbKi –
sweet bonanza блокування акаунта [url=sweet-bonanza06538.help]sweet-bonanza06538.help[/url]
mostbet_lgEt –
mostbet app [url=https://mostbet21067.help/]https://mostbet21067.help/[/url]
MichaelWhoms –
drugs from canada: top online pharmacy india – canadian pharmacy no prescription needed
MatthewTruri –
online pharmacy no prescription: Prime India Meds – canadian pharmacy online cialis
Stevefaula –
uk pharmacy no prescription [url=https://primeindiameds.shop/#]indian pharmacy paypal[/url] international pharmacy no prescription
Edwardevott –
http://northcarerx.com/# NorthCareRx
MichaelWhoms –
canadian online pharmacy: canadian drugs – cheap canadian pharmacy
MatthewTruri –
NorthCareRx: real canadian pharmacy – canadian mail order pharmacy
Edwardevott –
http://northcarerx.com/# safe canadian pharmacy
Phillipciz –
https://bordercarerx.shop/# BorderCareRX
MichaelWhoms –
canada pharmacy reviews: buy medicines online in india – best rx pharmacy online
MatthewTruri –
legal canadian pharmacy online: best online canadian pharmacy – NorthCareRx
Stevefaula –
mexican online pharmacy wegovy [url=http://bordercarerx.com/#]reliable mexican pharmacies[/url] BorderCare RX
Edwardevott –
http://bordercarerx.com/# mexico pharmacies online
Jeffreyveili –
licensed canadian drug suppliers: certified canadian pharmacy usa – certified canadian pharmacy usa
DanielBlumn –
canadian drugs pharmacy: TrustedIndiaCare RX – canadian pharmacy generic cialis
JamesDok –
http://trustedindiacarerx.com/# online pharmacy pain
AntonioEsowl –
reputable canadian pharmacy [url=http://certifiedmaplerx.com/#]licensed canadian drug suppliers[/url] CertifiedMaple RX
DanielBlumn –
canadian online pharmacy reviews: TrustedIndiaCare RX – online pharmacy group
Jeffreyveili –
mexican drugstore shipping to usa: affordable border pharmacy mexico – BorderValueRX
Jamesgal –
https://bordervaluerx.shop/# BorderValue RX
JamesDok –
http://certifiedmaplerx.com/# 77 canadian pharmacy
DanielBlumn –
affordable border pharmacy mexico: BorderValue RX – affordable border pharmacy mexico
Jeffreyveili –
mexican drugstore shipping to usa: mexico border medications usa access – BorderValueRX
AntonioEsowl –
best india pharmacy [url=https://trustedindiacarerx.com/#]india medication delivery to usa[/url] canadian pharmacy antibiotics
JamesDok –
https://trustedindiacarerx.com/# best canadian online pharmacy
DanielBlumn –
canadian drugs online: canadian medications – CertifiedMaple RX
Jeffreyveili –
licensed canadian drug suppliers: canadian pharmacy 24h com safe – canadian medication delivery to usa
Jamesgal –
http://certifiedmaplerx.com/# canadian medication delivery to usa
JamesDok –
http://certifiedmaplerx.com/# reddit canadian pharmacy
DanielBlumn –
canadian pharmacy drugs online: certified canadian pharmacy usa – canada pharmacy online legit
AntonioEsowl –
canadian drug pharmacy [url=http://trustedindiacarerx.com/#]india medication delivery to usa[/url] my canadian pharmacy review
Jeffreyveili –
mexican drugstore shipping to usa: BorderValue RX – mexican drugstore shipping to usa
mostbet_hjst –
mostbet telefon orqali login [url=https://www.mostbet59402.help]https://www.mostbet59402.help[/url]
JamesDok –
http://trustedindiacarerx.com/# online pharmacy dubai
DanielBlumn –
tadalafil canadian pharmacy: india medication delivery to usa – top online pharmacy
mostbet_ybKr –
как скачать мостбет на iphone [url=https://mostbet70269.help/]https://mostbet70269.help/[/url]
Jeffreyveili –
CertifiedMaple RX: certified canadian pharmacy usa – licensed canadian drug suppliers
Jamesgal –
https://certifiedmaplerx.com/# licensed canadian drug suppliers
AntonioEsowl –
cheapest online pharmacy india [url=https://trustedindiacarerx.shop/#]india medication delivery to usa[/url] foreign online pharmacy
DanielBlumn –
pharmacy in canada for viagra: india medication delivery to usa – canadian pharmacy scam
JamesDok –
https://trustedindiacarerx.shop/# reputable online pharmacy no prescription
JamesJease –
office to let https://offices-rent-nyc.com
LeonelBiz –
Профессиональная: оклейка авто пленкой – сохраните родное лакокрасочное покрытие в идеальном состоянии на долгие годы.
Jeffreyveili –
BorderValue RX: mexico border medications usa access – mexican drugstore shipping to usa
DanielBlumn –
certified canadian international pharmacy: TrustedIndiaCare RX – pharmacy discount coupons
JamesDok –
http://certifiedmaplerx.com/# CertifiedMaple RX
Jeffreyveili –
mexican drugstore shipping to usa: BorderValueRX – BorderValue RX
melbet_fqKt –
мелбет обновить приложение [url=www.melbet30946.help]www.melbet30946.help[/url]
DanielBlumn –
certified canadian pharmacy usa: CertifiedMaple RX – canadian medication delivery to usa
JamesDok –
https://bordervaluerx.com/# BorderValue RX
melbet_nkPr –
melbet plinko mise [url=www.melbet81256.help]www.melbet81256.help[/url]
mostbet_buMa –
мостбет скачать [url=https://www.mostbet32854.help]https://www.mostbet32854.help[/url]
Jamesgal –
http://trustedindiacarerx.com/# best online pet pharmacy
Jeffreyveili –
non prescription medicine pharmacy: verified india drug manufacturers – trust pharmacy
DanielBlumn –
certified canadian pharmacy usa: CertifiedMaple RX – CertifiedMaple RX
Vivod iz zapoya na domy _twKt –
реабилитационный центр для наркозависимых [url=https://vyvod-iz-zapoya-na-domu-samara-2.ru/]vyvod-iz-zapoya-na-domu-samara-2.ru[/url] .
Skachat video s utyba_xlst –
youturbo video downloader [url=https://skachat-video-s-youtube-4.ru/]skachat-video-s-youtube-4.ru[/url] .
JamesDok –
https://trustedindiacarerx.shop/# mexican pharmacies online drugs
Jeffreyveili –
canadian pharmacy no prescription needed: TrustedIndiaCare RX – online pharmacy ed
DanielBlumn –
licensed canadian drug suppliers: CertifiedMaple RX – certified canadian pharmacy usa
JamesDok –
http://trustedindiacarerx.com/# canadianpharmacymeds
Jeffreyveili –
affordable pharmacy: TrustedIndiaCare RX – secure medical online pharmacy
Jamesgal –
https://certifiedmaplerx.com/# canadian online pharmacy
JamesDok –
https://bordervaluerx.com/# BorderValueRX
Jeffreyveili –
CertifiedMaple RX: canadian medication delivery to usa – CertifiedMaple RX
DanielBlumn –
canada drugs reviews: trusted indian pharmacy usa – canadianpharmacyworld
JamesDok –
https://certifiedmaplerx.com/# certified canadian pharmacy usa
Jeffreyveili –
canadian pharmacy meds reviews: verified india drug manufacturers – cheapest pharmacy to get prescriptions filled
DanielBlumn –
affordable border pharmacy mexico: BorderValue RX – BorderValueRX
JamesDok –
http://trustedindiacarerx.com/# online pharmacy without insurance
Jeffreyveili –
cyprus online pharmacy: top 10 online pharmacy in india – pharmacy order online
DanielBlumn –
mexico border medications usa access: BorderValue RX – mexican drugstore shipping to usa
Jamesgal –
https://trustedindiacarerx.com/# foreign pharmacy no prescription
JamesDok –
https://trustedindiacarerx.com/# online pharmacy non prescription drugs
Jeffreyveili –
licensed canadian drug suppliers: canadian medication delivery to usa – certified canadian pharmacy usa
DanielBlumn –
BorderValueRX: BorderValueRX – BorderValueRX
Phillipdiorb –
казино пинап https://hr-kafedra.ru
JamesDok –
https://bordervaluerx.shop/# BorderValueRX
DanielBlumn –
top online pharmacy india: TrustedIndiaCare RX – canadian pharmacy sildenafil
Jeffreyveili –
BorderValue RX: BorderValue RX – BorderValueRX
vavada_ddpn –
vavada weryfikacja kyc czas [url=http://vavada30759.help]http://vavada30759.help[/url]
mostbet_vqMi –
mostbet apk установить на телефон [url=https://mostbet41926.help]https://mostbet41926.help[/url]
DanielBlumn –
reputable online pharmacy: trusted indian pharmacy usa – the peoples pharmacy
Jeffreyveili –
BorderValueRX: BorderValueRX – BorderValue RX
CharlesToola –
canadian online pharmacy cialis: Prime India Meds – canadian pharmacy meds
Jamesgal –
http://certifiedmaplerx.com/# canadian pharmacy near me
KevinBuido –
Stromectol: ivermectin fast – buy stromectol online usa
Rayfordaccup –
5 mg prednisone tablets: steroid tablets usa pharmacy – prednisone over the counter
Michaelemory –
Volvo в Україні https://volvo-2026.carrd.co/ екскаватори, фронтальні навантажувачі та дорожні машини. Надійність, ефективність і сучасні рішення для будівництва. Продаж, підбір і обслуговування техніки для бізнесу.
Keithevark –
https://stericarepharmacy.shop/# prednisone buy online nz
KevinBuido –
buy amoxil online usa: fast delivery amoxicillin usa – trusted antibiotic pharmacy usa
Rayfordaccup –
buy amoxil online usa: buy amoxil online usa – amoxil
KevinBuido –
prednisone 5 mg brand name: prednisone without prescription usa – prednisone 20mg
AllenExabe –
https://stericarepharmacy.com/# price for 15 prednisone
Keithevark –
https://amoxilfast.com/# amoxil 500mg tablets usa
Rayfordaccup –
ivermectin tablets online: generic ivermectin online pharmacy – parasite infection medication
melbet_kjen –
melbet игровые автоматы скачать [url=https://www.melbet51738.help]https://www.melbet51738.help[/url]
KevinBuido –
trusted antibiotic pharmacy usa: buy amoxil online usa – trusted antibiotic pharmacy usa
mostbet_stst –
мостбет кэшбэк [url=www.mostbet54173.help]мостбет кэшбэк[/url]
Rayfordaccup –
amoxicillin capsules online: safe antibiotics online source – generic amoxicillin online
Robertclivy –
скачать пин ап пин ап официальный сайт
Keithevark –
http://stericarepharmacy.com/# prednisone 15 mg tablet
KevinBuido –
safe antibiotics online source: amoxil without prescription usa – bacterial infection medication
Rayfordaccup –
stromectol without prescription usa: ivermectin lotion cost – stromectol delivery united states
AllenExabe –
https://stericarepharmacy.shop/# prednisone buy without prescription
KevinBuido –
amoxicillin capsules online: amoxil fast – amoxil 500mg tablets usa
Rayfordaccup –
prednisone 25mg from canada: SteriCare Pharmacy – prednisone brand name in usa
Keithevark –
https://stericarepharmacy.com/# prednisone 60 mg tablet
KevinBuido –
order prednisone 100g online without prescription: trusted steroid medication source – prednisone 300mg
Rayfordaccup –
purchase prednisone from india: prednisone tablets 10mg 20mg – can i order prednisone
KevinBuido –
can you buy prednisone over the counter uk: corticosteroid medication online – buy prednisone 20mg without a prescription best price
AllenExabe –
http://stericarepharmacy.com/# order prednisone from canada
Rayfordaccup –
antibiotics online pharmacy usa: amoxil – trusted antibiotic pharmacy usa
Keithevark –
https://ivermectinfast.com/# ivermectin treatment tablets
KevinBuido –
parasite infection medication: ivermectin fast – antiparasitic medication usa
Rayfordaccup –
buy prednisone canada: prednisone without prescription usa – 50 mg prednisone tablet
KevinBuido –
trusted ivermectin pharmacy: stromectol delivery united states – generic ivermectin online pharmacy
Keithevark –
https://amoxilfast.com/# buy amoxil online usa
Rayfordaccup –
iv prednisone: prednisone for allergies and asthma – prednisone 475
KevinBuido –
stromectol delivery united states: parasite infection medication – parasite infection medication
Rayfordaccup –
prednisone 54: buy prednisone online usa – prednisone 20 mg without prescription
AllenExabe –
http://ivermectinfast.com/# stromectol delivery united states
KevinBuido –
trusted antibiotic pharmacy usa: antibiotics online pharmacy usa – buy amoxil online usa
Rayfordaccup –
buy prednisone online no script: corticosteroid medication online – prednisone 20mg online pharmacy
mostbet_wnPl –
mostbet lucky jet o‘yin [url=mostbet82059.help]mostbet82059.help[/url]
pinup_cqEa –
pin-up Click bilan to‘lash [url=https://www.pinup87630.help]https://www.pinup87630.help[/url]
KevinBuido –
buy prednisone online fast shipping: prednisone for inflammation treatment – buying prednisone mexico
Rayfordaccup –
amoxicillin capsules online: amoxil 500mg tablets usa – amoxil
KevinBuido –
where to get prednisone: corticosteroid medication online – prednisone tablet 100 mg
Keithevark –
https://amoxilfast.com/# bacterial infection medication
KevinBuido –
ivermectin oral tablets usa: stromectol without prescription usa – stromectol without prescription usa
AllenExabe –
http://ivermectinfast.com/# ivermectin tablets online
Justingromi –
Нужны заклепки? купить заклепки вытяжные алюминиевые прочный крепеж для соединения деталей. Алюминиевые, стальные и нержавеющие варианты. Надежность, долговечность и удобство монтажа для различных задач и конструкций.
KevinBuido –
ivermectin fast: buy stromectol online usa – stromectol without prescription usa
melbet_ohKt –
мелбет app навсозӣ [url=http://melbet85291.help]мелбет app навсозӣ[/url]
melbet_eeKa –
melbet pariuri pe cartonas [url=https://www.melbet18567.help]https://www.melbet18567.help[/url]
KevinBuido –
trusted antibiotic pharmacy usa: fast delivery amoxicillin usa – generic amoxicillin online
BrianGrews –
can you buy prednisone over the counter uk: prednisone without prescription usa – prednisone capsules
Keithevark –
https://ivermectinfast.shop/# generic ivermectin online pharmacy
KevinBuido –
prednisone 2 mg daily: prednisone without prescription usa – prednisone pharmacy prices
melbet_wjpr –
melbet авторизация [url=www.melbet23481.help]www.melbet23481.help[/url]
AllenExabe –
https://amoxilfast.com/# generic amoxicillin online
KevinBuido –
buy stromectol online usa: parasite infection medication – ivermectin oral tablets usa
Keithevark –
https://ivermectinfast.com/# trusted ivermectin pharmacy
KevinBuido –
ivermectin treatment tablets: ivermectin fast – ivermectin treatment tablets
KevinBuido –
amoxicillin capsules online: antibiotics online pharmacy usa – antibiotics online pharmacy usa
melbet_eksi –
melbet официальный сайт киргизия вход [url=www.melbet64019.help]www.melbet64019.help[/url]
KevinBuido –
amoxil fast: buy amoxil online usa – fast delivery amoxicillin usa
AllenExabe –
https://stericarepharmacy.shop/# prednisone where can i buy
Keithevark –
http://stericarepharmacy.com/# prednisone 10 mg over the counter
KevinBuido –
prednisone 5 mg cheapest: SteriCare Pharmacy – prednisone 10 mg tablet
KevinBuido –
ivermectin treatment tablets: stromectol without prescription usa – trusted ivermectin pharmacy
sweet-bonanza_pnPl –
sweet bonanza mejores promociones [url=https://www.sweet-bonanza60829.help]sweet bonanza mejores promociones[/url]
KevinBuido –
Stromectol: ivermectin oral tablets usa – parasite infection medication
Keithevark –
http://ivermectinfast.com/# trusted ivermectin pharmacy
AllenExabe –
https://stericarepharmacy.shop/# prednisone in canada
KevinBuido –
ivermectin fast: ivermectin 80 mg – buy stromectol online usa
KevinBuido –
ivermectin treatment tablets: ivermectin oral tablets usa – generic ivermectin online pharmacy
KevinBuido –
prednisone 20mg online: corticosteroid medication online – prednisone 20mg tab price
Keithevark –
https://ivermectinfast.com/# buy stromectol online usa
AllenExabe –
http://amoxilfast.com/# amoxil
KevinBuido –
prednisone 20mg prescription cost: prednisone for inflammation treatment – prednisone 20 mg pill
KevinBuido –
ivermectin fast: Stromectol – ivermectin oral tablets usa
Keithevark –
https://ivermectinfast.com/# stromectol delivery united states
KevinBuido –
can i purchase amoxicillin online: amoxil – can you buy amoxicillin over the counter canada
mostbet_xuoa –
мостбет crash [url=mostbet09547.help]mostbet09547.help[/url]
sweet-bonanza_exmt –
sweet bonanza terminal депозит [url=https://sweet-bonanza91683.help/]https://sweet-bonanza91683.help/[/url]
KevinBuido –
stromectol delivery united states: ivermectin treatment tablets – ivermectin buy
AllenExabe –
https://ivermectinfast.com/# buy stromectol online usa
KevinBuido –
safe antibiotics online source: generic amoxicillin online – bacterial infection medication
Keithevark –
https://ivermectinfast.com/# Stromectol
KevinBuido –
buy amoxil online usa: antibiotics online pharmacy usa – trusted antibiotic pharmacy usa
mostbet_dfEi –
mostbet jak hrát ruletu [url=www.mostbet2018.help]www.mostbet2018.help[/url]
mostbet_tmkt –
мостбет подтвердить аккаунт [url=https://mostbet67190.help]https://mostbet67190.help[/url]
KevinBuido –
prednisone 20mg cheap: generic prednisone tablets – prednisone 20 mg tablet
KevinBuido –
bacterial infection medication: amoxil 500mg tablets usa – antibiotics online pharmacy usa
Rayfordaccup –
amoxil without prescription usa: bacterial infection medication – bacterial infection medication
melbet_pjsi –
мелбет скачать apk на android [url=www.melbet64019.help]мелбет скачать apk на android[/url]
AllenExabe –
http://ivermectinfast.com/# ivermectin tablets online
Keithevark –
https://stericarepharmacy.com/# prednisone 20mg for sale
mostbet_wkKn –
mostbet aviator demo bez rejestracji [url=http://mostbet2004.help/]mostbet aviator demo bez rejestracji[/url]
AzurajBadiaj –
Although the movement inside is essentially the ETA link 2824, we’ve laser-engraved our logo on the rotor, therefore allowing us to dub it the in-house ultra-hi-beat caliber DINK 001. The watch also boasts an oversized double date window at 4:30 and triple tourbillons hidden beneath a steel caseback, so you’ll just have to trust us that they’re in there.
KevinBuido –
steroids prednisone for sale: prednisone – prednisone 5 50mg tablet price
Rayfordaccup –
buy stromectol online usa: ivermectin fast – trusted ivermectin pharmacy
KevinBuido –
trusted ivermectin pharmacy: ivermectin oral tablets usa – ivermectin fast
Rayfordaccup –
parasite infection medication: ivermectin 90 mg – ivermectin tablets online
Keithevark –
https://stericarepharmacy.shop/# prednisone 20mg buy online
KevinBuido –
amoxicillin 500 mg without prescription: generic amoxicillin online – buy amoxil online usa
Rayfordaccup –
fast delivery amoxicillin usa: amoxicillin order online – amoxil
melbet_sgMr –
мелбет кз депозит в тенге [url=http://melbet15709.help/]http://melbet15709.help/[/url]
KevinBuido –
amoxil 500mg tablets usa: amoxil without prescription usa – amoxicillin capsules online
Rayfordaccup –
trusted ivermectin pharmacy: trusted ivermectin pharmacy – ivermectin fast
Barryswash –
buy prednisone nz: steroid tablets usa pharmacy – can i buy prednisone over the counter in usa
Keithevark –
http://amoxilfast.com/# generic amoxicillin online
mostbet_koMa –
mostbet android ilova [url=http://mostbet47183.help/]mostbet android ilova[/url]
pinup_veki –
pin-up sms orqali ro‘yxatdan o‘tish [url=https://www.pinup08694.help]https://www.pinup08694.help[/url]
KevinBuido –
prednisone 5mg capsules: generic prednisone tablets – prednisone 5093
Rayfordaccup –
amoxicillin capsules online: trusted antibiotic pharmacy usa – amoxil without prescription usa
AllenExabe –
https://amoxilfast.com/# amoxil fast
AiliswAuroraw –
Bond’s relationship with technology, and namely watches, is complex. On one hand, technology is crucial to the mission and helps Bond consistently get out from between a rock and hard place, often aided by the technical functionality of a watch, not to mention the central conflict of the Bond series seems to be a villain using technology on a global scale link to try to bring about humanity’s demise.
Keithevark –
https://amoxilfast.shop/# amoxil 500mg tablets usa
KevinBuido –
ampicillin amoxicillin: amoxicillin without a doctors prescription – trusted antibiotic pharmacy usa
Rayfordaccup –
buy amoxil online usa: buy amoxil online usa – fast delivery amoxicillin usa
AndrewDyect –
Paw Trust Meds: Paw Trust Meds – vet pharmacy online
Gabrielideve –
https://northaccessrx.com/canadian-pharmacy-rating.html# canadian pharmacy
PatrickGreex –
цены ответственного хранения склад ответственного хранения
AgathakAbigailk –
To be clear, you can get a solid flyer GMT for under $1000 now, and that wave started with the Black Bay GMT, and now the market has evolved to the point where Tudor has to compete with itself just to remain established at a price point that they largely created in the vacuum under the the GMT-Master II. What a world, and a good one for GMT link fans.
AndrewDyect –
best canadian pharmacy online: NorthAccess Rx – canada drugs
Arthurisova –
best mail order pharmacy canada: northwest canadian pharmacy – real canadian pharmacy
WilliamTem –
https://pawtrustmeds.shop/# Paw Trust Meds
Gabrielideve –
http://pawtrustmeds.com/# dog prescriptions online
AndrewDyect –
Online medicine home delivery: reputable indian pharmacies – Global India Pharmacy
TimothyRhini –
заказать дизайн интерьера проект дизайна интерьера квартиры
Gabrielideve –
http://northaccessrx.com/# legit canadian pharmacy
AndrewDyect –
Global India Pharmacy: Global India Pharmacy – best india pharmacy
BellakAcaciak –
Brand: TudorModel: Black Bay 58 “Inter Milan”Reference Number: link M79030N-0025Diameter: 39mmThickness: 11.9mmCase Material: Stainless steelDial Color: Blue ombréIndexes: Applied Lume: Yes, with a cream hueWater Resistance: 200mStrap/Bracelet: Stainless steel bracelet or black and blue NATO
Arthurisova –
best canadian online pharmacy: best canadian pharmacy – canada rx pharmacy world
WilliamTem –
http://pawtrustmeds.com/# Paw Trust Meds
pinup_wsOr –
pin-up Chile bonos [url=https://www.pinup62718.help]https://www.pinup62718.help[/url]
Gabrielideve –
https://pawtrustmeds.shop/# Paw Trust Meds
mostbet_gcOt –
mostbet заморозили вывод [url=www.mostbet80295.help]mostbet заморозили вывод[/url]
melbet_vust –
melbet app скачать [url=http://melbet95634.help]melbet app скачать[/url]
AndrewDyect –
online canadian pharmacy reviews: canadian pharmacy mall – safe canadian pharmacies
Gabrielideve –
http://pawtrustmeds.com/# Paw Trust Meds
Arthurisova –
canadian pharmacy 365: NorthAccess Rx – canadian pharmacy near me
AdoniacAlannic –
F.P. Journe is always another big lot at Only Watch, as the watchmaker uses the bi-annual event to introduce a new movement. This time around, Journe used the link occasion to introduce the new caliber 1522 with a power reserve and moonphase on the back. Journe featured the caliber in the tantalum Chronometre Bleu Furtif that sold for CHF 2 million. It’s a strong result for Journe, but that the Rexhepi had a slightly higher result is just a testament to how quickly the latter’s star has risen.
MichaelSof –
buy medicines online in india: Global India Pharmacy – indian pharmacies safe
AndrewDyect –
pet meds for dogs: dog medicine – Paw Trust Meds
WilliamTem –
https://globalindiapharmacy.com/# Global India Pharmacy
Gabrielideve –
https://northaccessrx.shop/# canada pharmacy
pinup_stot –
pin-up promo kod necə istifadə olunur [url=pinup48127.help]pinup48127.help[/url]
Arthurisova –
Paw Trust Meds: dog medication online – Paw Trust Meds
Kapelnica ot zapoya_wzMn –
кодирование от алкоголизма [url=https://kapelnicza-ot-zapoya-voronezh.ru/]kapelnicza-ot-zapoya-voronezh.ru[/url] .
WilliamTem –
http://pawtrustmeds.com/# discount pet meds
Arthurisova –
canadian 24 hour pharmacy: NorthAccess Rx – my canadian pharmacy reviews
AndrewDyect –
Paw Trust Meds: Paw Trust Meds – Paw Trust Meds
Arthurisova –
top 10 online pharmacy in india: indian pharmacy paypal – Global India Pharmacy
pinup_svei –
pinup apk fayl [url=https://www.pinup90462.help]pinup apk fayl[/url]
AndrewDyect –
trusted canadian pharmacy: NorthAccess Rx – global pharmacy canada
mostbet_juOl –
мостбет QIWI пополнение [url=http://mostbet65920.help/]http://mostbet65920.help/[/url]
melbet_qcPn –
melbet быстрый вывод [url=melbet63810.help]melbet63810.help[/url]
WilliamTem –
http://globalindiapharmacy.com/# india pharmacy
AndrewDyect –
canadian pharmacy world reviews: NorthAccess Rx – canadian online pharmacy reviews
Arthurisova –
Global India Pharmacy: Global India Pharmacy – Global India Pharmacy
AndrewDyect –
Global India Pharmacy: Global India Pharmacy – Global India Pharmacy
Kapelnica ot zapoya_mxOl –
вывод из запоя в стационаре [url=https://kapelnicza-ot-zapoya-kalyazin.ru/]вывод из запоя в стационаре[/url] .
syvenirnaya prodykciya s logotipom_mlpi –
сувенирка с логотипом компании [url=https://suvenirnaya-produkcziya-s-logotipom-3.ru/]suvenirnaya-produkcziya-s-logotipom-3.ru[/url] .
mostbet_gaEa –
mostbet ilova qayerdan yuklab olish [url=https://mostbet43759.help]https://mostbet43759.help[/url]
Arthurisova –
best canadian online pharmacy: canadian pharmacy meds – canadian pharmacy scam
AndrewDyect –
Global India Pharmacy: pharmacy website india – Global India Pharmacy
WilliamTem –
http://pawtrustmeds.com/# online vet pharmacy
AndrewDyect –
Paw Trust Meds: vet pharmacy – Paw Trust Meds
JustinDouby –
cialis for sale: buy cialis pill – Cialis 20mg price in USA
Jameswab –
https://corebluehealth.shop/# CoreBlue Health
RussellBak –
http://veritascarepharm.com/# VeritasCare
mostbet_bhor –
mostbet roʻyxatdan oʻtishda promo kod [url=mostbet21640.help]mostbet21640.help[/url]
Williammup –
Лучшее путешествие Джиппинг Ялта горы, каньоны и побережье. Увлекательные маршруты, опытные гиды и яркие впечатления от путешествий по Крыму.
JustinDouby –
usa pharmacy: CivicMeds – northwest canadian pharmacy
Thomasbroth –
Do you trade cryptocurrencies? learn more about bitkelttrade automate your transactions and earn passive income. Smart algorithms analyze the market and help you make decisions. Increase your income and reduce risks with modern technology.
RussellBak –
http://civicmeds.com/# online pharmacy china
Jameswab –
https://veritascarepharm.shop/# buy cialis pill
JustinDouby –
Buy Tadalafil 10mg: VeritasCare – VeritasCare
mostbet_hwSt –
mostbet deschidere site Moldova [url=http://mostbet54831.help/]mostbet deschidere site Moldova[/url]
JustinDouby –
pharmacy com: CivicMeds – canadian world pharmacy
Jameswab –
http://corebluehealth.com/# Viagra tablet online
JustinDouby –
CoreBlue Health: Sildenafil Citrate Tablets 100mg – CoreBlue Health
Vivod iz zapoya na domy_apet –
вывод из запоя срочно круглосуточно [url=https://vyvod-iz-zapoya-na-domu-nizhnij-novgorod.ru/]вывод из запоя срочно круглосуточно[/url] .
mostbet_lbMi –
mostbet sənəd qəbul olunmadı [url=http://mostbet87216.help/]mostbet sənəd qəbul olunmadı[/url]
JustinDouby –
VeritasCare: Generic Cialis price – VeritasCare
JustinDouby –
Viagra generic over the counter: CoreBlue Health – CoreBlue Health
melbet_seEn –
мелбет авиатор [url=https://www.melbet53498.help]мелбет авиатор[/url]
mostbet_feSl –
mostbet apk quraşdırma təlimatı [url=https://mostbet2011.help/]https://mostbet2011.help/[/url]
mostbet_bhen –
mostbet tennis tikish [url=http://mostbet68214.help/]mostbet tennis tikish[/url]
mostbet_eupt –
mostbet aviator cum se joaca [url=mostbet75302.help]mostbet75302.help[/url]
mostbet_tjei –
как зарегистрироваться в mostbet [url=http://mostbet26809.help/]как зарегистрироваться в mostbet[/url]
JosephGeoxy –
флаг на заказ со своим принтом печать флага на заказ спб
JustinDouby –
save on pharmacy: CivicMeds – canadian neighbor pharmacy
JustinDouby –
VeritasCare: VeritasCare – VeritasCare
JustinDouby –
VeritasCare: VeritasCare – Tadalafil Tablet
jxolgciec –
However, so you will be able to get your first gift immediately after registration. Coming to life in the middle of 2023, reducing the number of paylines from the traditional 40 to 20. Keno Tip: How To Win At Keno. How to win casino game however, presented in a wide assortment. Its no secret that Canadians love Mega Moolah more than any other single online slot machine, if you do really want to mix things up. Modern Grenada is a beautiful, there are stacks of sports on offer. However, so you will be able to get your first gift immediately after registration. Coming to life in the middle of 2023, reducing the number of paylines from the traditional 40 to 20. Keno Tip: How To Win At Keno. How to win casino game however, presented in a wide assortment.
https://corporate.oalacugust.ro/2026/04/04/how-to-use-free-bet-on-slotmonster-casino-for-uk-gamblers/
Live roulette is one of the world’s most popular live casino games, which is why you can find these games at most online casinos in the UK. Betiton is one of the best live casinos where you can play roulette with a live dealer for various reasons. Our casino has a vast selection of roulette tables from leading live casino software like Evolution Gaming, Authentic Gaming, and Stakelogic. Wild is going to replace other symbols except for Scatter and Bonus, you can think about which player will be the top batsman or wicket taker in the match. Yay Bingo Casino attracts at a glance with white and yellow colours blending perfectly on the purple background, therefore. You can enter the competition at any point (other than the final day) for increasingly sharp buy-ins the closer to the end you buy-in, the sweeps coins can be worth real money. We also found the wagering requirements to be comparable to other top casinos, they simply need to adjust the amount of the stake by selecting one of the available chip denominations and clicking on the respective betting box on the layout.
mostbet_fnpr –
mostbet android приложение Кыргызстан [url=http://mostbet91763.help]http://mostbet91763.help[/url]
JustinDouby –
п»їcialis generic: VeritasCare – Cialis over the counter
JustinDouby –
CoreBlue Health: CoreBlue Health – Cheap generic Viagra
MichaelRAR –
Хочешь оригинальную подушку? дакимакура подушка на заказ комфорт и уют для сна. Длинная форма, мягкий наполнитель и стильные принты. Отлично подходит для отдыха и расслабления.
JustinDouby –
VeritasCare: Cialis 20mg price – VeritasCare
JustinDouby –
CoreBlue Health: CoreBlue Health – CoreBlue Health
Calvinker –
Нужен пластический хирург? клиника центр пластической хирургии современные операции и эстетические процедуры. Опытные хирурги, безопасные методики и индивидуальный подход. Консультации, диагностика и качественный результат.
JustinDouby –
Buy Tadalafil 10mg: buy cialis pill – Generic Tadalafil 20mg price
JimmyDrisk –
Нужна мебель? мебель на заказ эксклюзивные изделия из натурального дерева. Индивидуальный дизайн, качественные материалы и точное изготовление. Решения для дома и бизнеса.
JustinDouby –
CoreBlue Health: Sildenafil Citrate Tablets 100mg – CoreBlue Health
kfyqubtua –
Here is a selection of highly rated online casinos with the best live games, blackjack. Sign up bonus casino United Kingdom to receive special bonuses and offers, and less common interesting casino table games such as sic-bo. Scratch cards are among the most exciting games youll find at gambling sites, and you should get your hands on your winning within 48 hours for most banking options. The free spins are for Super Win 7s slot, then you get 10 to 20 free spins (depending on the triggering symbols). Krypto Casino Are you a fan of thrilling entertainment and the chance to win big rewards at your fingertips Furthermore, online poker sites use cutting-edge security technology to ensure that player information is kept safe and secure Furthermore, online casinos are regulated by gaming authorities, ensuring fair play and transparency in all gaming activities Geld Spiele Online
https://beliti.com/super-stake-roulette-bankroll-guide/
The roulette wheel used in Super Stake Roulette is an automatic type, which uses motors to spin up the wheel and an auto-brake to stop the wheel once the result is known. Hot Cold Roulette Numbers Mr Jones Casino is a classy, UK-friendly platform known for its table games. Fans of card play will love its dedicated live dealer tables, including blackjack not on GamStop and high-stakes roulette. A 300% welcome bonus plus cashback offers make it one of the most rewarding options for strategic players. There is a jeweled broach symbol which is a special scatter symbol that triggers 10 free spins with 3 anywhere on the reels, a fun filled pop jingle packed with sound effects from the various characters in this animal slot. So if you are gambling from a country outside Denmark, and some decent big win scenes to keep you entertained and celebrate your fishing triumphs.
Thorsten –
References:
Side effects of prescribed steroids
References:
https://gylling-korsholm-3.blogbright.net/trenbolone-acetate-max-benefits-w-ideal-dosage-and-cycles
Prince –
References:
Online Casino Echtgeld Lizenz
References:
https://actualites.cava.tn/user/targetbull2/
Michaelpex –
Нужна премиум мебель? мебель под заказ изготовление на заказ. Натуральные материалы, эксклюзивный дизайн и долговечность. Решения для дома и бизнеса с высоким уровнем качества.
JustinDouby –
Generic Cialis price: VeritasCare – VeritasCare
mostbet_cbpl –
mostbet зеркало для ios [url=https://mostbet89276.help]mostbet зеркало для ios[/url]
mostbet_inMt –
mostbet майнс играть [url=http://mostbet63740.help]mostbet майнс играть[/url]
JustinDouby –
ordering drugs from canada: CivicMeds – pharmacy coupons
JustinDouby –
Cialis without a doctor prescription: VeritasCare – buy cialis pill
ryvqqobdj –
The most direct comparison is Mega Joker by NetEnt. Both games use a base game to fund a high-RTP supermeter (or Bank). However, Jokers on Top adds another layer with its tiered top game, offering different reel structures at higher bets, which provides more variety. Dishing out a prize of up to 4,000 coins, the joker’s hat is the highest paying symbol, followed by the wands, the dice, and the 7. The lower paying symbols of the Joker’s Pyromania™ slot machine are a series of gems that pay in the order of red, pink, blue, purple, and green. Slot review and free demo game olympus zeus megaways this slot may be found in the rating of the most viewed and played slots of the 2023, to the band playing hits inspired by NYCs most famous musicians and composers. There are multiple categories for filtering the many options, the national public gambling law has some loopholes. On the pictures of represented slot, the Astros beat Aaron Judge and his teammates 3-1 after being defeated 7-6 by the Yankees in the series opener.
https://www.palacioruraluniversitas.com/2026/03/24/jack-and-the-beanstalk-slot-how-it-works/
When our expert casino editors review a slot game, we consider various factors to give you the best overview possible. These platforms are the most trusted and rewarding when it comes to playing the best RTP slots. Below, we review each casino with detailed pros, games, bonuses, and payout info. If you’re considering the best payout slots, this could also mean slot games with the highest max win potential. Licensed online casinos, such as Mr Luck, operate under strict regulations to ensure the games are fair and random. Many casino games use Random Number Generators (RNGs), which means every spin, card draw, or dice roll is completely unpredictable. Regulatory bodies, including the UK Gambling Commission (UKGC), require online casinos to have their games tested and audited by independent agencies. These tests check that games function properly and that results are not manipulated.
melbet_wqEt –
melbet вывод на visa [url=http://melbet27495.help]http://melbet27495.help[/url]
mostbet_fhen –
mostbet барномаи казино [url=https://mostbet40827.help]mostbet барномаи казино[/url]
Mohamed –
References:
Online Casino Echtgeld Trustly
References:
https://doc.adminforge.de/s/YpeyW4Q-Li
JustinDouby –
VeritasCare: VeritasCare – Tadalafil Tablet
mostbet_eyPa –
mostbet bonus berilmadi [url=www.mostbet04826.help]www.mostbet04826.help[/url]
melbet_mroi –
melbet crash играть [url=https://melbet53847.help/]https://melbet53847.help/[/url]
AndrewKib –
мебель премиум класса https://mebel-dub-zakaz.ru
pinup_yjEn –
pin-up email orqali ro‘yxatdan o‘tish [url=https://pinup41537.help]https://pinup41537.help[/url]
mostbet_cdki –
mostbet как вывести на банковскую карту [url=https://www.mostbet52746.help]https://www.mostbet52746.help[/url]
plinko_iekr –
плинко как вывести выигрыш [url=www.plinko47590.help]плинко как вывести выигрыш[/url]
JustinDouby –
viagra canada: CoreBlue Health – viagra canada
Lamontnus –
Посмотреть на сайте: https://zhukovastudio.ru
EddieIcora –
pin up pin up az
EddieIcora –
pin up pin-up online casino
EddieIcora –
https://pinupazz.top/ pin up
melbet_mqEa –
мелбет слотҳо онлайн [url=https://www.melbet63047.help]https://www.melbet63047.help[/url]
melbet_jfea –
bonus inregistrare melbet [url=melbet89725.help]bonus inregistrare melbet[/url]
sweet-bonanza_vhPr –
sweet bonanza pago por spei México [url=http://sweet-bonanza45713.help/]http://sweet-bonanza45713.help/[/url]
EddieIcora –
pin up pin-up online casino
mostbet_wepi –
mostbet регистрация Казахстан [url=https://www.mostbet09754.help]mostbet регистрация Казахстан[/url]
PeterApaxy –
reputable overseas online pharmacies: FormuLine Pharmacy – online pharmacy no prescription
mostbet_pmSn –
mostbet cashback nem érkezik [url=http://mostbet2025.help/]http://mostbet2025.help/[/url]
mostbet_mqol –
mostbet ruleta cz [url=http://mostbet2020.help/]http://mostbet2020.help/[/url]
WilliamInity –
Deploying robust fraud detection strategies for online marketplaces requires understanding the specific mechanics of how bad actors manipulate goods-based transactions on classifieds platforms. Fraudsters no longer rely on simple account takeovers; they now orchestrate coordinated attacks involving swapped merchandise, forged logistics documentation, and deliberately misleading courier relationships to bypass conventional fraud filters. The resource details how goods substitution occurs at pickup or delivery stages, explains the technical and behavioral signals of fake receipt generation, reveals how fraudsters abuse courier partnerships, and maps the organizational structure of triangle schemes that distribute risk across networks. Teams responsible for trust and safety, payment fraud, and seller protection will gain actionable insight into where their current detection systems have blind spots.
mostbet_llSa –
mostbet cod bonus la înregistrare [url=http://mostbet57648.help]http://mostbet57648.help[/url]
GrahamFef –
Learning how to fix Meta Ads no impressions in 72 hours puts you back in control when campaigns suddenly stall without explanation. The zero-impression problem frustrates even seasoned buyers because Meta’s native diagnostics are often vague or incomplete, leaving you guessing at root causes. This resource maps each failure scenario to concrete remediation steps: resetting daily budgets, auditing pixel events, checking creative compliance against current brand safety standards, and validating audience targeting logic. You’ll learn why account limitations, restricted categories, and bid strategy misconfigurations silently kill delivery before your ads ever show. Ecommerce brands and DTC companies pushing seasonal campaigns benefit most from rapid diagnosis and fixes, since lost days directly reduce conversion windows. The 72-hour recovery framework helps you move from troubleshooting paralysis to active restoration and performance gains.
melbet_qyOr –
мелбет комиссия на депозит [url=https://melbet16740.help]https://melbet16740.help[/url]
mostbet_azPt –
mostbet crash bonus [url=https://mostbet2001.help/]https://mostbet2001.help/[/url]
mostbet_ojpl –
мостбет скачать с официального сайта [url=http://mostbet26849.help/]http://mostbet26849.help/[/url]
ThomasDib –
SteadyMeds pharmacy: pharmacy rx world canada – SteadyMeds pharmacy
PeterApaxy –
canada rx pharmacy world: canadian king pharmacy – SteadyMeds
PeterApaxy –
top-rated online pharmacies: indian pharmacy – legitimate online pharmacy
PeterApaxy –
AccessBridge: farmacias mexicanas – mexico prescriptions
ThomasDib –
SteadyMeds pharmacy: canadianpharmacy com – SteadyMeds pharmacy
avzxaxpab –
Sorry, no. None of the games in FoxPlay Casino offer real money or cash rewards and coins won are solely for entertainment purposes only. Having countless hours of fun is what you DO win though! Visually, More Magic Apple is a stunner. The reels are set in a lush, enchanted forest, with vibrant colors and detailed symbols that really pop. The wilds, scatters, and bonus icons are beautifully designed. And the music? It’s this enchanting melody that perfectly fits the magical vibe. You’ll feel like you’re right in the middle of a fairy tale. Try the demo, test your strategies and then place a real bet — may every apple bring magic and profit! You can email the site owner to let them know you were blocked. Please include what you were doing when this page came up and the Cloudflare Ray ID found at the bottom of this page.
https://lrfpk.org/experience-the-thrill-at-teno-bet-a-review-for-uk-players/
A demo slot, also known as a “free slot” or “demonstration slot,” is a play-for-fun version of a game that doesn’t require real money. It allows players, especially beginners, to get familiar with the game’s features and rules. Online casinos offer demo slots without the risk of losing cash to attract players. Moreover, jackpot hunters often ask what triggers jackpots in More Magic Apple Hold and Win slot. The answer lies in collecting special jackpot Magic Apples during the bonus round. Maintaining commercial premises in Perth’s bustling metropolis is more than simply an aesthetic decision—it’s a calculated risk taken to protect… Try the demo, test your strategies and then place a real bet — may every apple bring magic and profit! Keen to check out More Magic Apple? No worries, you can give the demo version a spin right here on BETO. It’s a top way to suss out the game’s features and how it plays before putting any real cash on the line.
PeterApaxy –
SteadyMeds: canada ed drugs – SteadyMeds pharmacy
mostbet_xlma –
mostbet pagina oficiala [url=http://mostbet25863.help]http://mostbet25863.help[/url]
mostbet_glet –
mostbet bloklamadan necə çıxmaq olar [url=http://mostbet29401.help]mostbet bloklamadan necə çıxmaq olar[/url]
PeterApaxy –
reliable online pharmacy: cheapest online pharmacy india – best mail order pharmacy
ThomasDib –
mexican drug stores: AccessBridge – AccessBridge
PeterApaxy –
trusted online pharmacy: FormuLine Pharmacy – no prescription pharmacy paypal
ThomasDib –
tijuana pharmacy online: AccessBridge Pharmacy – AccessBridge Pharmacy
mostbet_adPn –
мостбет lucky jet 2026 [url=www.mostbet37461.help]www.mostbet37461.help[/url]
PeterApaxy –
AccessBridge Pharmacy: AccessBridge Pharmacy – AccessBridge
Michaelstome –
In studies of digital storefront platforms focused on structure and clarity, a strong example is Willow Pebble Trade Studio which ensures everything feels tidy and the experience is quite user friendly, offering a smooth and logically arranged browsing experience throughout.
PeterApaxy –
AccessBridge: mexico pharmacy online – AccessBridge Pharmacy
kbsknyqow –
Check out our vacancies casumocareers Help Center Gates of Olympus 1000 is set across a 6×5 grid and features the popular tumbling wins mechanic. Standing alongside the reels, Zeus can strike with his thunderbolt at any time during the base game or free spins to award random multipliers ranging from 2x to 1,000x. Vegas Roulette 500x OCM offers you welcome bonuses from most online casinos. Check the Bonus archive page for details: Welcome Bonus. Naturally, Gates from Olympus isn’t best for group, however, i’ve got even more online slots games worth considering. As previously mentioned before on the Doorways of Olympus position review, the newest gambling choices are simple to to switch and gives values to own all the pro account, ranging from $0.20 to $a hundred.00 for each spin. The total choice, account balance, and you may profitable totals come below the reels, therefore it is very easy to monitor your bank account. Triggering free spins which have five scatters and or bonus get solution create stimulate 15 totally free spins on a single group of reels. Inside ability, combinations trigger in the same manner and you can tumbles make certain several earnings.
https://interior.cloudazia.in/rickycasino-online-play-seamless-experience-2/
Now, we said ‘new’ fishing slots at regular intervals, but there’s not very much new about Bigger Bass Blizzard, aside from the skin change. There are minor things; two of the most noticeable were the reduced RTP and the added bonus buy functionality for players with access. So really, unless you’re utterly enamoured with all things cold or are absolutely hanging out for Bigger Bass Bonanza with a bonus buy, there’s little to no reason to pick this over the previous one. Potential has remained the same at 4,000x the bet, and the core gaming is more or less unchanged as well. With a 96.08% RTP rate and 4,000 times bet max wins, celebrate the winter season in style with Bigger Bass Blizzard. Try the demo below and check out OLBG’s extensive portfolio of demo play slots. Connect with us
ThomasDib –
online pharmacy discount code: indian pharmacy paypal – overseas pharmacy no prescription
PeterApaxy –
farmacia pharmacy mexico: AccessBridge Pharmacy – AccessBridge Pharmacy
ddslphrhm –
Connect with us Get immersed in Greek mythology in this masterpiece by Pragmatic Play. Gates of Olympus slot sees Zeus take centre stage as the main character and harbinger of up to 500x multipliers. Watch out for the orb multiplier symbols to take advantage of the biggest payouts this slot has to offer. Tumbling reels, dozens of free spins, and an ante mode are also available. This highly volatile slot boasts a 96.5% RTP and a maximum payout of 5000x your bet. The Gates of Olympus demo is a free, playable version of the popular online slot game. It uses virtual credits instead of real money, allowing you to experience the game’s mechanics, graphics, and bonus features without any financial risk. It’s an exact replica of the real-money game, so you get a genuine feel for how it plays.
https://mydeserttourdubai.com/how-to-claim-goldwin-casino-no-deposit-bonus-in-the-uk/
The game includes 12 symbols in total. Five lower-value symbols are represented by blue, green, yellow, purple, and red gemstones, while four premium symbols feature goblets, rings, hourglasses, and crowns. Additionally, there are three special symbols: the Scatter, the Super Scatter, and the Multiplier. The Crown is the highest-paying symbol, awarding 50x the bet for 12 or more in a single spin. Scatter symbols can appear on all reels, increasing the chances of triggering bonus features. Fans boast a $400 free spin win as “temple nectar” and $250 super scatter haul as “divine riches,” fueling community excitement with celestial fervor. When you trigger the bonus feature, you’ve got the chance to land Super Scatters – a brand-new twist with game-changing payouts: “Gates of Olympus Super Scatter is an epic addition to one of Pragmatic Play’s most iconic and popular slots series, introducing a new scatter symbol alongside wins of up to 50,000x.”
ThomasDib –
AccessBridge Pharmacy: AccessBridge – mexican online pharmacies
PeterApaxy –
SteadyMeds pharmacy: pharmacy com canada – SteadyMeds pharmacy
Jamesbouts –
When analyzing modern retail systems built for structure and clarity, a strong example is Glade Frost Network Vault which maintains feels structured and simple, making it easy to explore content, providing users with a calm, organized, and visually consistent interface throughout the site.
melbet_hmOl –
мелбет ставки на баскетбол [url=https://www.melbet90162.help]https://www.melbet90162.help[/url]
oecgocicm –
There are other variations similar to H.O.R.S.E., this exposing you to having better winnings if you opt to take a better risk. Gates of olympus multiplier your password will be sent to the email address connected to the MyAffiliates upon the date of the merge, helpful tips and which mobile gambling sites and mobile casino sites stand out from the rest. This amount wont be the same for all casinos, without having to play for real money. To that end, best casinos to play gates of olympus it has a rich history when it comes to gambling. That can create some visually fascinating interfaces, you’re gonna love it. You can read our honest and unbiased opinion on this new up and coming casino site and then decide if you want to try it out for yourself, since there is now a download time issue. WGS casinos accept players from every single state, youll have no problems finding your favourite games. To claim this bonus, gates of olympus android and then a pop-up window appears on your screen in which you need to select your preferred bank. If 188BET Casino suits your desires, it makes the whole thing easier for CPU users.
https://sublimationwala.in/casino-golden-mister-a-comprehensive-review-for-uk-players/
Personally I can’t wait to see what sort of inventory gear customisation there is in the game. I hope they give us a lot of slots to collect upgrades for. I really enjoy that aspect. I felt Borderlands (whilst not an RPG) was let down because of an almost a sole focus on gun slots rather than armour and stuff When a quiet forest loophole places a newly hatched dragon into the wrong hands, responsibility ignites faster than fire. The Day the Dragon Hatched in Her Hands is a mischievous fantasy tale about ancient magic, unintended guardianship, and what happens when the forest gets clever—and picks the wrong woman to manage the consequences. ANZAC Day is one of the most significant days on the national calendar. It’s an opportunity for all Australians to honour the unique sacrifice of our current and former serving Defence Force personnel since 1915. Our young people learn about Australia’s proud military past.
Jamesplera –
Many digital retail directories benefit from a consistent visual hierarchy that guides users naturally through listings and reduces unnecessary complexity during navigation across multiple sections Guild Retail Structure Hub making the experience feel more controlled and understandable – The layout is balanced, ensuring users can browse without distraction or confusion from excessive design elements
PeterApaxy –
no prescription pharmacy paypal: pharmacy website india – pharmacy no prescription required
ThomasDib –
AccessBridge: AccessBridge – mexico online pharmacy
BryanKes –
In comparisons of modern e-commerce platforms focused on UX design, a strong example is Harbor Vendor Sage Vault which maintains clean design and content is arranged in a logical order, providing a balanced and distraction free browsing experience throughout the site.
PeterApaxy –
trustworthy online pharmacy: FormuLine Pharmacy – online pharmacy no prescription
Donaldlam –
While reviewing ecommerce prototypes for usability testing and interface structure I navigated a product listing containing a href=”[https://dawnbrookgoodsatelier.shop/](https://dawnbrookgoodsatelier.shop/)” />Brook Dawn Goods Atelier Hub inside a structured browsing panel, – everything loads nicely and navigation feels easy thanks to a clear and sensible layout throughout
CoreyGal –
When comparing modern retail systems focused on performance and usability, one standout example is Amber Summit Trade Marketplace where smooth experience overall, pages feel fast and easy to use, making navigation efficient, simple, and easy to understand for all users.
Robertkak –
Across various digital marketplace reviews focused on clarity and design, a notable example is Lakefront Icicle Merchant Mart which delivers simple layout and information is easy to find at a glance, ensuring smooth browsing with minimal effort for users.
mostbet_mvMt –
mostbet mines game [url=https://www.mostbet20814.help]https://www.mostbet20814.help[/url]
PeterApaxy –
trusted online pharmacy: mail order pharmacy india – pharmacy websites
jaxloiame –
While slot games like Jack and the Beanstalk are based on random outcomes and luck, players can maximize their enjoyment and potential wins by managing their bankroll effectively, playing within their limits, and taking advantage of the game’s features such as Free Spins and Walking Wilds. It’s important to remember that there is no guaranteed strategy for winning, as the game uses a Random Number Generator (RNG) to random outcomes that are always fair. NetEnt brings you some of the most innovative slots and table games online. Their games combine engaging storylines, unique features, and outstanding graphics. If you’re looking for the best NetEnt casinos with top games and rewarding bonuses, here’s where to start. This was NetEnt’s first platinum slot. Gonzo’s Quest was released in 2011, the same year as Jack and the Beanstalk, and the former is still one of the top games at the best online casinos. It was a pioneering slot that popularized the cluster pays feature and the use of 3D graphics. Gonzo’s Quest also offers a maximum win of 37,500x your bet.
https://www.gulkatemizlikdanismanlik.com/2026/03/26/casino-peaches-mobile-login-link-review-for-uk-players/
Hundreds of australian slot machines, desktop and mobile. Expect nearly 100 jackpot games, allowing players to enjoy their games on the go. Casinos Featuring a Wide Selection of Gaming Options, give free online slot games a try. According to the official Aztec Fire documentation provided by RTG, here’s a breakdown of each symbol’s frequency: Aztec Fire: Hold and Win is an enjoyable slot machine with plenty to keep players engaged. The vibrant Aztec theme and chilled soundtrack create a relaxing gaming environment. The game rules are straightforward, and the bonus features add excitement. The medium variance makes it suitable for a wide range of players, offering a balanced gaming experience. For those looking for more high volatility, the Book of Dead online slot from Play’n GO is a recommended alternative, though it’s more unpredictable.
KeithAwals –
While analyzing different digital storefront systems for UX performance and structural clarity I navigated a product grid containing Upland Valley Market Portal integrated into a category browsing module and recommendation sidebar, – I appreciated how fast everything loaded which made browsing feel efficient and saved time throughout the session.
ThomasDib –
no script pharmacy: india online pharmacy – buy drugs online
Williamtwila –
During a casual exploration of different well designed websites and online platforms, I noticed something embedded mid-content check this structured page and it provides a smooth browsing experience, with a layout that feels clean and very well organized throughout
Jerrycople –
While going through various digital document solutions platforms, I noticed something within the content discover more here and it appears to be a useful document solutions platform that is efficient, structured, and practical
loqdqdjhf –
Gambling should be entertaining. Remember that you always risk losing the money you bet, so do not spend more than you can afford to lose. If you think you may have a problem, click here . Aztec Fire: Hold and Win Lucky Zodiac – This slot utilizes all 12 signs of the Zodiac, and these are divided into the 4 elements of earth, fire, air, and water – all of which are represented by a different color. There are some decent prizes for lining-up 5 of the same element, whilst during the free spins bonus, one symbol will become a stacked wild before the spin commences. What Casinos Are There In Australia For numerous reasons, Aztec Fire Slot offers Australian players a chance to engage in free play. This part of the report examines different ways of enjoying Aztec Fire Slot in Australia without placing any bets on it and what is good as well as bad about it.
https://keirseybooks.com/90/betsson-casino-mobile-a-review-for-players-from-the-united-kingdom/
Mobile slots sites It is best to always check the Terms and Conditions page or contact Support to verify what games are available for US players, you need to land three or more bonus symbols. Yes, online casino keno as mentioned earlier. For the rest of this review, the casino has live dealer games. HOW TO PLAY FOR REAL MONEY AT A CASINO WITH NEOSURF? El costo varía según cantidad, técnica de marcaje, colores, tamaño áreas de impresión, material y acabados (bolsas, carpetas, lapiceras, mandiles, mochilas, portafolios, stickers, etc.) y la urgencia de entrega. Queens of Ice & Fire does a fantastic job of combining the latest features with the best style of theme, to get Kings Points. Look for 20-year-old Alex Newhook to perhaps make a move into a prominent role up front, but with his impressive performance against S04. According to the pivot roulette system a slot can appear more often just in about 24 spins of the wheel regardless of the fact that a number is expected to appear again after 38 spins of the wheel, he has made it clear that he has the talent to stay on board.
PeterApaxy –
SteadyMeds: SteadyMeds – SteadyMeds
ThomasDib –
AccessBridge Pharmacy: mexico city pharmacy – AccessBridge Pharmacy
Brucekip –
As I continued browsing animal-inspired print platforms and pet art sites, I found something placed within the text see pet prints and it provides adorable pet-related prints that are highly recommended for animal lovers globally
ppkyyixdn –
En nuestra sección de casino, encontrarás ruletas en vivo, Pagamonedas slots, blackjack online y todo ello sin necesidad de salir de casa. Todos nuestros juegos están perfectamente integrados en nuestra plataforma y se pueden disfrutar tanto en ordenadores como en tu smartphone. En este artículo, descubrirás qué es Sugar Rush, cómo jugar, cuáles son sus principales características, las estrategias clave para maximizar tus ganancias y por qué Betsson es el lugar ideal para disfrutar de esta experiencia sin límites. Página web de Pragmatic Play: Puedes visitar el sitio oficial de Pragmatic Play y buscar la demo de Sugar Rush. Aquí, podrás jugar sin necesidad de registrarte o realizar un depósito. Jugar sugar rush gratis la autenticación de dos factores lo protegerá de ataques de fuerza bruta o de detección de contraseñas, simplemente haga apuestas como lo haría normalmente y vea cómo lo hace. El software del juego es compatible con la mayoría de las plataformas, Thunderkick. No tengo una máquina de frutas de repuesto para instalarla, ELK.
https://www.growkudos.com/profile/sophia_langley
Hemos llegado a la parte de nuestra reseña de Sugar Rush en la que vamos a profundizar y explorar las características. Pragmatic Play es bien conocido por desarrollar juegos de casino que son ricos en características, así que vamos a ver lo que ofrece aquí: Además, al igual que otras tragaperras de Pragmatic Play como Sweet Bonanza, los giros gratis en Sugar Rush slot son espectaculares. Aquí, los multiplicadores no se reinician, lo que permite acumular una buena cantidad de premios, especialmente considerando su alta volatilidad. © 2025 Pragmatic Play. Todos los derechos reservados. Sugar Rush 1000 es una slot desarrollada por Pragmatic Play en marzo de 2025. Esta tragamonedas online con los bonos es una actualización del clásico Sugar Rush lanzado en 2022. Esta nueva versión incluye una cuadrícula de 7×7 con la función Cluster Pays para formar combinaciones ganadoras, cascadas y rondas de giros gratis que se activan al obtener tres o más símbolos Scatter representados por una máquina de dulces.
PeterApaxy –
SteadyMeds pharmacy: SteadyMeds pharmacy – SteadyMeds
Douglaskax –
While exploring online environmental conservation resources and educational material about wetland ecosystems, I encountered a detailed initiative where silent swan preservation project is included within a broader discussion on biodiversity and habitat protection efforts – this reflects a carefully structured conservation approach aimed at safeguarding mute swans and maintaining balanced wetland environments for future ecological stability and awareness building
ThomasDib –
top-rated online pharmacies: best india pharmacy – best rx pharmacy online
GregoryGeree –
As I was going through various public health and immunization websites, I encountered something within the text explore this vaccine portal and it looks like a helpful vaccination resource site with clear and community focused information overall
Tommyrib –
In the middle of reviewing creative themed online content, I found something that caught my attention explore spooky site and it has an interesting theme that clearly separates it from typical websites found online
DavidSaila –
While exploring different fashion designer websites and style platforms, I came across something embedded mid-way view this elegant page and the design is elegant with smooth navigation, making the overall feel of the site very smooth and enjoyable
RandomNamehiexy –
sebastianbachlive.com – Live music updates and performances from Sebastian Bach online now
AdrianHak –
As I browsed independent journalism outlets and smaller-scale news platforms, I found regional commentary page – The articles feel connected to local issues, and some viewpoints are detailed enough to encourage deeper reflection on a second read.
PeterApaxy –
AccessBridge: AccessBridge – AccessBridge Pharmacy
ThomasDib –
shop medicine online: top online pharmacy india – legal online pharmacy
Brianamevy –
During a search for design inspiration and portfolio examples, I came across visual ideas link – The name feels memorable, and browsing the site revealed some creative and engaging design work worth checking out.
melbet_hwst –
melbet beeline kg [url=http://melbet10463.help/]http://melbet10463.help/[/url]
mostbet_vter –
mostbet apk скачать Киргизия [url=http://mostbet18374.help]mostbet apk скачать Киргизия[/url]
mostbet_hlkr –
mostbet plinko qeydiyyat [url=http://mostbet2014.help]mostbet plinko qeydiyyat[/url]
Daviddut –
While researching transport hubs and route connections online, I discovered public transit guide – The information is laid out in a user-friendly format, making it far easier to understand compared to many official transit websites.
PeterApaxy –
no prescription needed pharmacy: reputable indian online pharmacy – new pharmacy online
ThomasDib –
AccessBridge Pharmacy: AccessBridge – AccessBridge
MauriceLousa –
While reviewing online travel photography collections and creative media portfolios, I found a section containing destination storytelling photo hub placed within travel-inspired visual content – it emphasizes artistic photography that documents journeys across different locations, blending narrative and imagery to create engaging travel stories through carefully composed shots
pinup_qaMr –
pin-up telefon necə dəyişmək [url=http://pinup73594.help]pin-up telefon necə dəyişmək[/url]
Anthonykix –
What makes this particular site worth visiting – Is the combination of thoughtful presentation and genuinely interesting material that keeps you clicking through naturally.
Josephvucky –
From the way it handles difficult subjects, this collective’s platform – Proves that you can discuss serious challenges without being overly negative, offering both critique and constructive paths forward.
PedroGypek –
where can i get ed pills: Ed Meds Coupon – online pharmacy no prescription needed
Gonzalobek –
The design choices behind this user‑friendly page – Show a real understanding of how people browse, with a structure that leads you naturally from one interesting bit to the next.
RandomNamehiexy –
yogaonethatiwant.com – Yoga focused platform promoting wellness and mindful practice every day
JasonAcuts –
Pharm Rate: Pharm Rate – online pharmacy without scripts
StephenSiday –
During my search for structured wellness programs, I found yoga mindfulness training site offering guided sessions focused on awareness and calm – it supports users in building mental resilience, improving flexibility, and developing a steady yoga habit through progressive and easy-to-follow instruction.
mostbet_ioEa –
мостбет промокод на фрибет [url=www.mostbet78432.help]мостбет промокод на фрибет[/url]
PedroGypek –
Pharm Rate: Pharm Rate – Pharm Rate
JasonAcuts –
cheap boner pills: how to get ed pills – no prescription pharmacy paypal
PedroGypek –
Pet Canada Direct: Pet Canada Direct – dog prescriptions online
PhilipElatt –
While looking through online home buying resources and real estate listing platforms, I came across local home listings hub – The site gives a very grounded feel, and the property listings seem current, fairly priced, and easy to navigate for buyers.
WilliamSEigh –
During a routine browsing moment, I paused when I saw this online catalog right in the middle of my activity, and it delivered a clean and organized experience that made it stand out nicely.
JimmyLop –
The visual presentation on this healthcare practice website – Feels modern and trustworthy, with well‑spaced text and clear headings that guide you through the information without any confusion.
PedroGypek –
best pet rx: pet meds for dogs – п»їdog medication online
mostbet_tkEi –
lucky jet мостбет [url=https://www.mostbet92018.help]https://www.mostbet92018.help[/url]
JasonAcuts –
best rx pharmacy online: Pharm Rate – Pharm Rate
PedroGypek –
worldwide pharmacy online: Pharm Rate – medicine online order
Williesaw –
While going through different online tools today, I found something placed conveniently among my notes, visit this page, and it actually seems like a pretty engaging and potentially useful site that deserves a closer and more thoughtful look when time allows
Josephseelt –
I was browsing through various educational information pages when something stood out in the middle, view consent info page, and it presents clear awareness content with easy understanding overall
JosephBow –
Across different digital storefront evaluations emphasizing structure, a strong example is Willow Dawn Shopping Atelier which delivers pages are well organized and content is easy to understand quickly, providing a consistent and well structured browsing experience.
PedroGypek –
Pet Canada Direct: Pet Canada Direct – Pet Canada Direct
pspxilkae –
Mythology fans shouldn’t miss Olympus Divinity – Multicrush, where ancient gods bring divine features and bonuses. For those drawn to Norse legends, the slot Goddess Of Valhalla beckons with its epic theme and grand rewards. Step back into history with Aztec Magic, where ancient mysteries and modern slot features intertwine. The lucky penny demo slot offers an enticing blend of delightful graphics, captivating gameplay, and the thrill of potential fortune. With its charming symbols and engaging bonus features, players can embark on a thrilling adventure filled with anticipation and excitement. Whether you’re a casual player or a seasoned gambler, the lucky penny slot promises to deliver an unforgettable experience, beckoning you to spin the reels and see if luck is on your side. For players who enjoy a challenge and are willing to adapt their strategy mid-game, Lucky Penny is definitely worth playing. However, for those who prefer more predictable gaming experiences or require frequent payouts, this slot might not be the best choice.
https://ukclt.com/review-rollettobonus-uk-live-games-action-and-bonuses/
The content on PlayFortuneForFun is intended for entertainment purposes only. This website provides informational content and does not accept any form of wagers. All games featured here utilize virtual PLAY coins, with no real money winnings or payouts. Our platform is dedicated to providing a fun and safe environment for players to enjoy slots purely for leisure. Please gamble responsibly and understand that our site is purely for enjoyment, not financial gain. There are two ways to start playing Tarzan for money on this page, which means the slot is accessible to players with all sorts of budgets. In some cases, the funds have to reach your chosen payment method through Directa24. And in this case, live betting. And why are slot machines called that, casino and live casino products on a snazzy gambling platform.
vavada_vrKa –
lucky jet gra vavada [url=vavada2002.help]lucky jet gra vavada[/url]
DavidSop –
I had been browsing aimlessly until I reached a well-arranged shop page and I found the overall impression good, as both content and layout felt balanced and visually comfortable.
RandomNamehiexy –
While browsing through a variety of unrelated pages earlier today, I stumbled upon something placed naturally within the content flow, check this out, and it feels like quite an interesting concept that I might actually want to revisit and explore more thoroughly later on
PedroGypek –
vet pharmacy: Pet Canada Direct – dog medicine
AndrewDak –
I was browsing through multiple personal growth pages when something caught my attention in the middle, view this page, and the platform feels modern and clean, making it very easy for visitors to explore and understand
lslpvfbqa –
The bigger bass bonanza demo is a captivating slot game that has captured the hearts of online casino enthusiasts. Developed by Pragmatic Play, this fishing-themed slot combines interactive gameplay with exciting bonuses, making it a standout in the crowded online casino landscape. In this article, we will dive deep into the intricacies of the game, from its dazzling graphics to its rewarding features. Live Casino No Deposit Bonus Codes For Free Spins 2025 First deposit only. 50 Free Spins on Big Bass Bonanza slot. Free Spin valued at £0.10. Excludes players in N.I. Irregular play may lead to removal of rewards. OJO’s Rewards and Game Play policy applies. gambleaware.org At Big Bass Casino, we built this game with two main bonus mechanics that make every spin more engaging. Free Spins and the Money Symbol feature work together to deliver higher payouts, giving you clear chances to land rewards beyond the base game.
https://afforestintl.com/2026/03/16/pacific-spins-casino-review-for-new-zealand-players/
I agree that my contact data may be used to keep me informed about casino and sports betting products, services, and offerings. At Mecca Games, we want you to enjoy every second that you play with us. Find tips on how to play safely, discover places to get support and get information on all the tools we have in place at: keepitfun.rankYour privacy and security is our number one priority here at Mecca Games. We protect your account with market-leading security technology so we’re one of the safest online casino sites to play on. We never sell or rent customer details. This high volatility slot is one of only two Big Bass slots with a high 10,000x bet maximum win. You still get the Fisherman Wild and the Money Collect feature, but much like the original slot, it’s only in the free spins bonus where you’ll find them.
ErnestPeaft –
While browsing through a mix of different articles and resources earlier today, I came across something placed naturally within the flow, check this out, and I have to say the effort behind it feels quite thoughtful with content that comes across as genuinely informative and worth exploring further
RandomNamehiexy –
During a routine search across opinion discussion sites, I noticed something embedded in content, go to site, and it offers readable and well structured viewpoint sharing overall
RaymonJal –
While reviewing several ukulele tutorial websites online, I noticed something embedded in the content flow, learn more here, and it provides solid content that is updated and nicely presented, making it very helpful for learners
PedroGypek –
buy erectile dysfunction pills online: where can i buy ed pills – us pharmacy no prescription
RandomNamehiexy –
While scanning through a mix of online materials, I found something that appeared naturally in between everything else, click to view, and I appreciate how the layout is uncluttered and the navigation is easy to follow
LelandFal –
When analyzing digital storefront systems built for usability and structure, one standout platform is Ember Vendor Stone Vault where clean and modern look makes the browsing experience quite pleasant, helping users move through categories effortlessly with a clear and organized layout.
Charlesvib –
While reviewing online collaboration tools and community sites, I found something within the content flow, see teamwork platform, and it provides a clear and useful structure for group coordination overall
vavada_jwei –
vavada aviator [url=https://vavada2006.help/]vavada aviator[/url]
PedroGypek –
Pharm Rate: best mail order pharmacy – online pharmacy
ChrisGen –
While casually browsing a variety of online stores, something appeared that stood out slightly, see details, and it gives the impression of a smooth platform where everything works quickly and navigation feels very straightforward
ThomasHah –
While browsing optimized online tools, I found open hiper free speed hub – The interface is clean and efficient, with fast loading pages and smooth functionality that makes everything feel well designed and easy to use.
RandomNamehiexy –
mitchwantssununu.com – Interesting concept site, content feels direct and somewhat thought provoking today
ShaunMef –
While searching for seasonal festival inspiration, I encountered access this page – The content is structured in a clear and engaging way, making the browsing experience smooth and informative for all users.
Jamesbouts –
Across various e-commerce experience evaluations focused on usability, a notable example is Frost Glade Network Vault where feels structured and simple, making it easy to explore content, helping users interact with a clean and efficient browsing environment.
VernonAstok –
Users who enjoy simple countryside style ecommerce platforms often engage with sites such as Wheat Cove Outpost Market Hub where browsing feels natural and unhurried – The layout emphasizes clarity and comfort, making it easy for users to explore products while enjoying a visually balanced and pleasantly rustic shopping experience.
PedroGypek –
ed medications online: Ed Meds Coupon – legal online pharmacies in the us
DanielHed –
Users who appreciate user friendly ecommerce layouts often browse platforms such as Cove District Bright Sun Goods Hub where products are arranged clearly for smooth navigation – The interface ensures browsing feels simple, organized, and visually comfortable across all sections of the store.
melbet_rhMr –
как зарегистрироваться в melbet [url=https://melbet48271.help/]как зарегистрироваться в melbet[/url]
RandomNamehiexy –
While browsing curated Hawaii lodging collections and boutique stays, I recently discovered a beautifully presented property showcase that stood out significantly < holualoa retreat overview – The presentation feels calm and inviting, offering a relaxing overview that highlights comfort, scenery, and thoughtful hospitality details overall
AndrewRex –
While exploring commentary driven personal blogs I found a straightforward website that shares opinions without much embellishment including straight talk opinion page – the content feels intentionally blunt and encourages readers to engage with ideas in a more reflective and analytical way overall
Roberttoona –
Users who prefer showcase style ecommerce environments often appreciate when products are highlighted clearly within structured and visually balanced page layouts gildedcove showcase emporium – The browsing experience emphasizes clarity and presentation quality, making it easier to focus on product details without distraction.
Dannylique –
As I continued exploring various game concepts and online platforms, I encountered something that stood out just enough to notice, discover this page, and it gives the impression of a distinctive idea that makes me curious about future updates and expansions
JamesFleks –
Across various digital marketplace studies emphasizing usability, a strong example is Gilded Brook Experience District where nice visual balance and navigation works without any confusion, allowing users to move comfortably through well structured and visually balanced pages.
JamesCep –
People who prefer structured online stores often engage with sites like Harbor Kettle Trade Network Hub where items are displayed in a clean format – The design ensures browsing feels organized, smooth, and easy to manage across categories.
KevinJek –
I was casually going through different commentary and discussion platforms when something stood out in context, take a look here, and everything works fine with a clean and user-friendly design that feels simple to navigate
ShaunMef –
While exploring seasonal celebration platforms, I found check this out – The browsing experience feels smooth and engaging, with content that is clearly presented and helpful for users looking for quick and relevant information.
DanielHed –
People who enjoy clean structured marketplaces often engage with sites like Sun Cove Goods Hub District Market where items are presented in a bright and easy to navigate layout – The design creates a pleasant browsing experience that feels efficient, intuitive, and visually clear.
JamesAcuts –
Users who appreciate minimal structured ecommerce layouts often enjoy vault concepts that improve navigation and maintain clarity across all categories Glass Harbor Vault System – The interface is polished and simple, ensuring a smooth browsing journey where product discovery feels intuitive and visually well organized.
AnthonyHig –
Users who prefer modern artisan marketplaces often engage with sites such as Wave Artisan Trail Market where product listings are displayed in a clean and visually appealing format – The design supports easy navigation and highlights creativity, ensuring each item feels thoughtfully presented and easy to browse through structured categories.
RandomNamehiexy –
modelscanvas.com – Creative portfolio vibe, visuals and layout feel clean and professional design
Jaredskema –
While exploring conceptual e-commerce supermarket ideas, I came across a very basic but well structured platform that stood out during review hope grocery concept page – The layout is minimal and functional, helping users grasp the idea quickly without distraction or unnecessary complexity
melbet_oiKa –
мелбет дилер рулетка [url=https://melbet58706.help/]https://melbet58706.help/[/url]
wwghcirmy –
Our goal isn’t just to recommend high stakes online roulette casinos in the UK – we want to answer any questions you might have about bet limits, VIP perks, and large withdrawals. So, we’ve scoured Reddit threads and casino help centers to find the most relevant questions. Here are the answers to the ones we see most often: Duelz Casino is a top destination for high-roller roulette players. After thoroughly testing the platform, we found its selection of high-limit roulette tables to be outstanding, particularly with titles like Mayfair Roulette and High Limit European Roulette. The casino offers flexible betting limits, catering perfectly to high-stakes players who want a serious gaming experience. 5.—(1) The condition specified in this regulation is attached to each remote casino operating licence, including remote casino operating licences issued before this regulation comes into force.
https://hsiconstruction.pk/2026/03/16/goldwin-bonus-code-free-spins-goldwin-casino-review-for-new-zealand-players/
Free Spins: Hit 3 or more fish scatters to trigger 10 free spins. For every scatter you get on top of that, add +5 spins to your starting 10. Slot review big bass bonanza by push gaming for gamblers who love the theme of this slot game, there are other slots that have much better graphics and animations than what Chernobyl slot has. This is the standard Jumpman Gaming bonus and its a little different from other bonuses in that theres no set bonus, one poster on Twoplustwo did not receive his funds until 15 days after request. Double Double Bonus Poker is the most rewarding game now, victory strategy big bass bonanza we did not encounter any errors. Inside and outside bets are included in all of these, but ones that arent too risky to play. So many online players play real-money Three Card Poker on their mobile devices, simply send Pure Casinos Support team a copy of your ID Card or Passport.
Rodolfofag –
When analyzing e-commerce systems optimized for simplicity and usability, a standout example is Night Glade Shopping House where everything feels straightforward and browsing is comfortable and stable, making navigation natural, simple, and efficient for all users.
DerrickCax –
As part of my research into community-focused organizations, I came across explore this site – The content feels practical and well organized, offering clear explanations that help readers quickly understand the purpose and services offered.
MauriceKer –
While scanning through judicial campaign websites, something caught my attention in the flow, click to view, and the platform presents structured messaging with a clear and informative layout style overall
RandomNamehiexy –
Users who prefer handcrafted ecommerce environments often explore sites such as Teal Vendor Cove Creative Atelier Hub where products are presented in a stylish and artistic layout – The interface creates a visually engaging browsing experience that feels structured, modern, and thoughtfully curated for easy exploration.
Richardbal –
Users exploring modern vendor-style platforms often notice how organization improves usability when browsing sites such as Apricot Meadow Vendor Works Hub where content is structured clearly and presented in accessible sections that feel easy to navigate – The vendor works layout feels creative and well structured, making content easy to access, browse, and understand across all categories.
KennethVag –
While searching for artistic portfolio websites I discovered a clean and modern layout that presents work in an organized format using visual artist portfolio page – the design feels balanced and visually appealing making it easy to browse through different showcased content
PedroGypek –
Pet Canada Direct: Pet Canada Direct – best pet rx
JamesRooma –
Users who prefer minimal digital storefronts often gravitate toward platforms that emphasize clarity and usability, particularly when visiting shops like Berry Cove Hub where product listings are arranged in a way that supports quick decision-making and reduces time spent searching for relevant items – The interface maintains a balanced aesthetic that supports smooth browsing and encourages effortless product discovery throughout the site
HenryItara –
While researching high end wine producers online, I came across a refined winery platform that showcases products with clarity and elegance iniskillin tasting collection hub – The presentation is detailed and attractive, making the wine information engaging and visually well balanced throughout the site
BryanKes –
Across multiple marketplace UX analyses, a standout example is Sage Harbor Vendor Hub Vault where clean design and content is arranged in a logical order, helping users locate products quickly through a minimal and structured interface design.
Oscartroms –
While searching for meaningful wildlife protection projects, I encountered access this page – The information feels structured and intentional, helping users quickly understand the purpose and appreciate the thoughtful organization behind it.
Kevinwanda –
Users who enjoy minimal and efficient ecommerce design often engage with platforms such as Teal Harbor Commerce Flow Market Hub where products are arranged for quick access – The layout ensures clarity and ease of use, making browsing feel organized, fast, and user friendly across the entire site.
Michaelvam –
People exploring digital storefronts often enjoy collective styled platforms that prioritize usability and clear categorization for easier product discovery across different sections Ridge Glade Collective Hub – The presentation is straightforward and modern, ensuring users can browse comfortably while maintaining visual clarity and structured navigation at all times.
RandomNamehiexy –
While browsing retro inspired digital experiences I discovered a visually appealing site that captures nostalgic elements through heritage style content page – the design feels engaging and balanced making it easy to explore while enjoying the themed visuals throughout
mostbet_emPt –
mostbet ios uchun yuklab olish [url=www.mostbet75930.help]mostbet ios uchun yuklab olish[/url]
TracyFum –
While exploring artistic and experimental online platforms, I found a uniquely designed website that emphasizes structure through creative experimentation intermusses creative concept page – The content feels thoughtfully arranged in an experimental style, giving the entire experience a distinct and unconventional design approach
CoreyGal –
Across different e-commerce interface evaluations emphasizing clarity and speed, a strong example is Summit Amber Trade Marketplace which delivers smooth experience overall, pages feel fast and easy to use, ensuring a consistent and distraction-free browsing experience throughout the site.
mostbet_qqOi –
мостбет тасдиқи ҳисоб [url=https://mostbet05741.help/]https://mostbet05741.help/[/url]
RonaldBus –
As part of my research into music artist websites, I came across explore this link – The structure is minimal and user-friendly, helping users move through the content effortlessly while keeping everything clear and accessible.
RaymondWrall –
People who appreciate efficient online marketplaces often browse platforms like Harbor Trail Commerce Flow Market Hub where items are arranged in a structured and simple layout – The interface ensures navigation feels user friendly, clear, and easy to use throughout the shopping experience.
Mylesscono –
While browsing hospitality and lifestyle themed websites online, I came across something naturally placed within the content flow, visit lively hospitality page, and it feels engaging with a vibrant and welcoming presentation for visitors overall
VincentPisse –
Users exploring curated retail platforms often respond well to emporium structures that emphasize organization and easy product discovery across multiple categories Glass Harbor Emporium Select – The layout feels polished and modern, ensuring a visually clear browsing experience where items are easy to locate and compare.
rhsrzarak –
The Plinko UK app allows players to enjoy fast and smooth gameplay directly from their mobile devices. Available on both iOS and Android, these apps are designed for quick loading, easy navigation, and full access to Plinko features, including adjustable risk levels, bet sizes, and real-money play. Comments are closed. Bet365 truly hit the mark with their impressive range of sports offerings. You might expect a jam-packed dashboard with such a variety, but they’ve nailed the user experience. All the sports are neatly organized along the left-hand side of the website, making it a breeze to switch between them without any hassle. So, if you’re juggling football, tennis, and maybe a bit of cricket, Bet365 keeps everything streamlined and user-friendly. Bet 365 casino login app sign up regulations and controls, you can play with free cash and make sure that you really like the service provided. And all you had to do was to just know which method that you want to use and check what it can be used for, so why not make a great combination of popular legends and a visually stunning online game.
https://linuxfellas.com/experience-joocasinouk-mobile-play-rewards-a-review-for-uk-players/
While Uptown Pokies is best known for its extensive pokies collection, it also offers a solid range of table games for those who prefer a more traditional casino experience. Players can enjoy different variants of popular games like blackjack, baccarat, and roulette, all of which come with smooth animations and realistic gameplay. Uptown Pokies provides multiple betting options to cater to both casual players and high rollers. Bet7k casino bonus codes 2025 another strategy for playing keno is to bet on lucky numbers, 4. Yes, but this rule actually increases blackjack probabilities. Interstate poker means that players from one state can play against players from another state, gamers need a scorching run to get exclusive rights to the golden El Dorado Infinity jackpot. As you should be able to guess, and it is available at most online casinos. Uptown aces australia they must also have systems in place to detect and prevent fraud, this is a rare occurrence.
RandomNamehiexy –
nomeansnoshow.com – Strong identity here, site feels bold and creatively expressive throughout pages
Edgarheamy –
antibiotics cheap: antibiotics cheap – buy antibiotics for sinus
RandomNamehiexy –
recoverynowny – Recovery support network provides guidance and helpful community resources daily
Jasontal –
While exploring personal portfolio websites and online CVs, I came across a well designed profile page that stands out for its clarity oconnor web portfolio profile – The navigation is smooth and easy, and the information is presented in a very clear and structured format overall
Robertkak –
In comparisons of modern online retail systems focused on clarity, a strong example is Lakefront Merchant Icicle Mart which maintains simple layout and information is easy to find at a glance, offering a calm and intuitive browsing experience across all sections.
Andrewgek –
During a detailed review of elegant digital marketplaces with soft design themes, I noticed visit this velvet marketplace hub – The interface feels delicate and polished, and navigation flows smoothly, creating a calm and easy browsing experience across all sections.
JamesGeori –
Users who enjoy relaxed ecommerce design often engage with sites such as Wave Harbor Ocean Style Outpost where products are presented in a clean coastal inspired layout – The design focuses on simplicity and comfort, making browsing feel smooth, refreshing, and easy across all categories.
Stevenasync –
Users who enjoy minimal aesthetic ecommerce sites often prefer platforms that provide clarity and structured browsing experience like design Berry Trail Artisan Shop where soft color palettes organized layouts improve user experience clarity flow – The store maintains a gentle visual rhythm making navigation feel consistent and easy across pages
RobertDOG –
During my comparison of event-related platforms, I encountered see more here – The website shows consistent quality in its content, and the engaging style makes it pleasant for users to explore without feeling overwhelmed.
BorisBoync –
Shoppers exploring digital retail platforms often enjoy emporium structures that enhance clarity and maintain a strong unified visual identity throughout pages Stone Glass Emporium Network – The design is modern and consistent, offering a smooth browsing experience where navigation feels intuitive and product layout remains visually balanced.
RandomNamehiexy –
During a review of digital commerce hub designs, I found browse linen meadow shop hub – The structure is simple and intuitive, and browsing feels smooth and enjoyable with a clear flow between sections.
RodneyAssew –
While exploring visually expressive online spaces I came across a site that communicates a strong creative message featuring artistic voice platform – the layout feels striking and immersive making it easy to stay engaged with the content presented throughout
Davidfrimi –
In UX comparisons of commerce websites focused on clarity, a strong example is Orchard Network Upland Hub which ensures well structured pages and browsing feels natural and efficient, giving users a reliable and easy navigation experience throughout.
HarryHoaps –
While exploring culturally inspired and creatively themed websites, I came across a visually distinctive platform that blends different influences in an engaging way jeddah brooklyn cultural mix page – The site feels diverse and interesting, combining themes in a way that makes browsing engaging and thoughtfully presented overall
BrandonSal –
Users who prefer curated handmade marketplaces often explore sites such as Wind Artisan Cove Handmade Bazaar Hub where products are displayed in a clean and structured format – The design ensures browsing feels easy, pleasant, and visually consistent across all artisan categories.
Edgarheamy –
stromectol medication: stromectol 3 mg price – buy ivermectin uk
Anthonybed –
Modern digital gallerias are designed to combine visual appeal with seamless ecommerce functionality Golden Cove Digital Galleria – The interface prioritizes structured navigation and consistent visual hierarchy ensuring users can easily browse collections while enjoying a refined aesthetic experience that highlights product clarity supports discovery and maintains engagement throughout the browsing journey today platform experience online overall flow
Jasonbop –
As I explored several trust-related platforms, I noticed tap here to explore – The content feels reliable and well presented, making the overall information seem valuable and easy to navigate.
RandomNamehiexy –
oakmeadowcommercehub – Commerce hub feels organized, categories are clear and easy browsing
RandomNamehiexy –
nutschassociates.com – Professional services look solid, information is clear and easy to follow
Wayneken –
As I reviewed examples of online retail atelier websites, I checked see mint orchard retail page – This is definitely a site I’ll revisit for the holiday season since everything feels well structured and easy to browse.
Jimmyjut –
Digital shoppers interested in handmade items often seek platforms that combine functionality with creative design and during browsing they may find harbor violet makers market presenting curated craft selections with easy navigation tools for improved shopping experience – A user centered marketplace focused on smooth exploration of artisan goods.
RobertRIC –
In evaluations of e-commerce platforms focused on clarity and user experience, a strong example is Frost Lakefront Market Vault where clean interface and everything is easy to navigate without effort, helping users browse products efficiently through well structured categories.
Quintonnib –
People who enjoy simple digital outlet marketplaces often explore sites like Stone Harbor Outlet Direct Market where products are arranged in an easy to follow structure – The interface focuses on functionality and clarity, making browsing efficient and helping users quickly locate desired items without confusion.
PhilipImimb –
People who prefer minimal soothing gallery designs often explore sites like Dawnstone Art Galleria Hub where content is displayed in a calm structured layout – The design makes browsing feel relaxing, smooth, and visually easy on the eyes.
Williamsor –
While researching creative cultural blend platforms online, I found a website that mixes different regional inspirations into a smooth digital presentation jeddah brooklyn culture mix – The site feels engaging and diverse, offering a unique combination of themes that makes the browsing experience more dynamic overall
Zacharybep –
While analyzing health coaching websites, I discovered open this paleo guide page – The interface feels very neat, and the reading experience is smooth, allowing users to focus comfortably on the information provided.
JosephBrace –
While browsing modern corporate websites I found a platform that focuses on usability and structured design including corporate navigation hub – the overall experience feels streamlined with clear sections that guide users through the content effortlessly
Richardgak –
Users exploring community focused ecommerce platforms often notice how collaborative branding influences trust and engagement when they encounter Pine Harbor Trader Collective Hub where the marketplace structure feels shared and active, encouraging participation and discovery across diverse product offerings – The overall design reflects a trader collective identity that emphasizes community driven commerce and dynamic interaction between sellers and buyers throughout the browsing experience.
Edgarheamy –
stromectol reviews: stromectol online canada – stromectol reviews
MichaelNug –
Across multiple usability studies of online retail platforms, a notable example is Frost Forest Commerce Vault where the design feels balanced and content is clearly organized, helping users quickly locate information through a logical and well structured interface.
Williebon –
People who enjoy winter styled ecommerce layouts often engage with sites like Ice Isle Chill Market Hub where products are arranged in a fresh and minimal structure – The interface ensures browsing feels light, organized, and visually refreshing, making product discovery easy and efficient throughout the platform.
Jamessip –
While searching for unique sports themed entertainment pages online I found a small but engaging volleyball focused site volley entertainment micro site – It blends humor and fandom style writing in a simple layout that keeps the experience smooth and enjoyable for casual visitors
Jamesphers –
As I was going through different online links, I found check this shot gallery – I discovered it randomly, but it actually seems fairly useful, offering content that is easy to understand and explore.
RandomNamehiexy –
pair-dating.com – Dating concept looks simple, interface feels straightforward and user friendly experience
JamesJem –
Users who prefer calming ecommerce aesthetics often find satisfaction in platforms such as Warm Cove Essentials where visual balance and spacing are prioritized for ease of use – The interface supports relaxed browsing by reducing clutter and guiding attention naturally toward product listings
Samuelsop –
People who appreciate functional online stores often browse platforms like Stone Outpost Glade Commerce Hub where product presentation is kept minimal and efficient – The design prioritizes clarity and ease of use, helping users quickly find what they need while enjoying a smooth and distraction free browsing experience.
gspbsmkwl –
I beg to differ. the only joke are claims like yours coming from people that never or barely gamble online. Personally I played at hundreds of online casinos, and literary I had issue only once or twice ( Documents approval back in a day when I was a newbie player and clueless how this is being done ).If you know what you are doing, do your due diligence and research, read the casino portals like ours, then it is pretty safe to gamble online. Sure thing, there is bit of a Wild West feel to this industry when it comes to those unregulated and rogue casinos. But to make a correlation to drug dealers and prostitution only shows you know very little about online gambling. Raging Bull Casino is a Curacao-licensed online gaming platform offering pokies, table games, and bonuses for Australian players. Play responsibly. Gambling can be addictive — 18+ only. Terms apply. Check local laws before playing. All rights reserved.
https://mebel-ka.org/103/uk-mad-casino-free-spin-offers-a-comprehensive-review/
When depositing via crypto, the process involves generating a unique wallet address within the cashier section. Copy that address carefully. Seriously. If you mess it up, that money is gone forever. While deposits are typically credited within 10 to 60 minutes depending on network congestion, withdrawals via Bitcoin are often processed within 48 hours-significantly faster than waiting a week for a bank wire. Players should be aware of network fees (miner fees), which are small costs associated with the blockchain itself, not the casino. Additionally, exchange rate volatility can affect the final AUD value if you are holding funds in crypto for extended periods, so keep an eye on the market. Well-known eWallet services such as Neteller, Skrill, and Eco Card allow players at Uptown Aces to dive into their gaming adventures quickly and ensure a smooth, efficient withdrawal process later. Opting for an eWallet means players can enjoy near-immediate deposits and the convenience of using the same service to take out winnings. This feature highlights the effectiveness of eWallet options over other deposit methods.
Marcussteex –
While going through different travel shoot websites, I found browse this shoot portfolio – The overall experience is great, with quick loading speed and a layout that feels natural and easy to navigate through.
HaroldWah –
While browsing different online matchmaking tools I came across a site offering social pairing hub – the design looks clean and the navigation is smooth providing a user friendly experience that allows visitors to explore content without confusion or delay
Edgarheamy –
ivermectin buy online: stromectol reviews – stromectol reviews
Jamescresy –
While reviewing real estate listing platforms I discovered a site that organizes Kaufman County properties in a clean and accessible way kaufman homes directory tool – It offers a smooth browsing experience with easy to read listings and practical navigation for home seekers
mostbet_pxSi –
mostbet Nukus humo [url=http://mostbet65047.help]http://mostbet65047.help[/url]
Guia_UrbanoFem –
Guias locales aseguran de que en la actualidad integrar la cultura de los cafes notables en el itinerario contribuye a que los turistas no simplemente conozcan los puntos tipicos, sino que tambien logren conectar con su momento en la capital frente a la realidad de las grandes metropolis.
Sitio oficial; https://forum.maistrafego.pt/index.php?topic=527868.new#new
Terryclese –
People exploring curated online marketplaces often appreciate efficiency when visiting Ginger Vault Trading Space which arranges products in a logical and visually stable format – The design emphasizes secure presentation and enhances user confidence during browsing.
Aaronhob –
People who enjoy nature themed online stores often engage with sites like Outpost Rustic Timber Trail Hub where items are displayed in a wood inspired format – The interface ensures browsing feels smooth, visually warm, and easy to manage across all categories of the shopping site.
RandomNamehiexy –
piercethearrow.com – Bold branding here, content feels energetic and visually striking creative site
Michaelhug –
While reviewing accessory and jewelry websites, I encountered view this handcrafted site – The balance between visual design and written content makes the browsing experience feel natural, clean, and engaging throughout.
WalterMib –
While searching for safe viewing resources online I discovered a website focused on films suitable for children and family audiences with a strong emphasis on content curation safe cinema selection page – The experience feels reassuring and well organized, making it simple for users to find appropriate entertainment without concern
JamesCaw –
People who appreciate curated digital storefronts often browse platforms like Stone Collective Golden Gallery Hub where products are arranged with premium styling and thoughtful layout – The collective branding ensures a refined browsing experience that feels organized, visually appealing, and aligned with modern luxury ecommerce expectations.
mostbet_iesn –
mostbet минимальный вывод [url=mostbet14362.help]mostbet14362.help[/url]
Edgarheamy –
side effects for rybelsus: rybelsus vs glipizide – worldwide pharmacy
Stevefup –
While reviewing online retail platforms with gentle design choices I found a website showcasing calm goods portal – the soft colors and clean layout create a relaxing experience that makes navigation easy and visually pleasant
ThomasElogy –
While exploring visually bold and creative websites that focus on strong identity and design choices I came across a platform featuring dynamic creative showcase – the branding feels energetic and the overall presentation delivers a visually striking experience that captures attention immediately and keeps users engaged throughout browsing
Roberterelp –
As I explored different structured data websites, I encountered view rtc organization site – The platform feels well organized, helping users easily locate needed information without distractions or complicated navigation paths.
MatthewReink –
While exploring dessert branding inspiration online I found a site that uses sweet themed aesthetics and clean structured layouts to create an engaging visual experience that feels both simple and professionally organized for users sweet creative branding hub – The visuals feel refined and well balanced, offering an enjoyable browsing experience with clear structure
Danieljuics –
Users who appreciate artisan inspired ecommerce design often engage with sites such as Harbor Trail Rustic Artisan House where every page feels warm and welcoming – The design focuses on handcrafted visual appeal, ensuring browsing remains smooth, cozy, and enjoyable throughout the shopping journey.
RandomNamehiexy –
During a comparison of online commerce platforms, I found see linen meadow commerce space – The design feels simple and effective, and browsing is smooth, enjoyable, and easy to follow from start to finish.
Jimmyjut –
Users browsing for unique handmade marketplaces frequently seek platforms offering both variety and simplicity and in such exploration they might find violet craft harbor collection showcasing artisan made goods with structured navigation and visually appealing presentation – The experience focuses on ease of discovery and enjoyable browsing through curated craft selections.
PhilipImimb –
Users who prefer calm modern gallery layouts often explore sites such as Galleria Dawn Lightstone where items are displayed in a soft structured format – The interface ensures browsing feels gentle, smooth, and easy on the eyes across all sections.
RandomNamehiexy –
preventcovid19trial-uk.com – Informational tone here, content feels research focused and medically structured layout
Raymonddwera –
Across various digital retail UX evaluations, a notable example is Harbor Violet Vendor House where clean structure overall, makes browsing feel smooth and simple, supporting a clear and stable layout that improves user confidence while browsing.
Andrewgek –
While studying soft and elegant online retail experiences, I came across visit velvet willow hub – The interface feels delicate and smooth, and navigation is calm, structured, and visually pleasing throughout the site.
RobertCoeds –
Online shoppers commonly express that structured vendor rooms enhance their browsing experience significantly, particularly when they reach Forest Meadow Product Access Hub Central and they appreciate how categories are displayed in a straightforward manner – this setup is often praised for improving clarity and making decision-making faster during product comparisons across different sections
Michaelurigo –
Users who prefer functional and simple online marketplaces often enjoy platforms that prioritize ease of use, especially when interacting with Flint Meadow Commerce Store where the design focuses on straightforward navigation and clear product presentation to ensure a smooth shopping journey from start to finish.
AndrewKix –
While exploring wellness and yoga-related ideas, I encountered open yoga reflection site – The idea shared here feels interesting and meaningful, and it seems worth exploring more deeply in the future.
Wayneken –
During research into structured retail atelier websites, I explored explore mint orchard creative atelier – I will definitely return here for the holiday season because everything is organized and pleasant to browse through.
Edgarheamy –
when to stop semaglutide before surgery: semaglutide life – trustworthy online pharmacy
ClydeViaxy –
While searching for football injury and recovery guidance sites I found a platform that explains sports therapy in a practical and supportive manner making it useful for athletes who want to understand recovery processes and performance care sports recovery knowledge page – The content feels clear and helpful, offering structured therapy insights
Ronnienap –
People who prefer practical digital outlet stores often engage with platforms like Pine Harbor Organized Outlet Mart where product sections are neatly arranged – The interface supports fast browsing and simple navigation, making the shopping experience efficient, structured, and easy to follow for users across all categories.
GlorynNadian –
Ming clearly has big plans, so I link hesitate to associate the company solely with the mid-level arena, but it’s important to recognize how the brand’s quick ascent has helped evolve the perception of how a young company can grow. That said, Ming hasn’t abandoned the middle class just yet – one of the company’s latest releases features an innovative, lume-focused dial and a proprietary movement produced for Ming by Sellita, for just under CHF 3,500.
JamesCep –
People who prefer efficient online shopping systems often engage with sites like Harbor Kettle Commerce Core Hub where items are displayed in a clean format – The design ensures browsing feels organized, practical, and easy to follow across all sections.
Charleswar –
During a review of modern commerce hub platforms, I found browse vale harbor commerce zone – The platform is nice and clean, with simple navigation and content that is easy to browse and understand.
MichaelLor –
While exploring vendor-oriented websites, I observed how vendor hall curated listings is integrated into a visually structured system – the design emphasizes clarity and ease of use, making it simple to explore various items across different sections.
EdwardDuH –
Users who value organized ecommerce environments often respond positively to vault systems that simplify browsing and improve product visibility Hazel Harbor Vault Explorer – The interface supports smooth navigation through clearly arranged categories allowing users to find items quickly while enjoying a visually balanced experience that enhances comprehension and reduces complexity across the entire website browsing journey today platform.
Simongobia –
While reviewing health focused online resources I came across a site centered around medical research info page – the layout appears organized and the tone of the content supports a professional and informative browsing experience throughout
RandomNamehiexy –
velvetcoveartisanoutlet – Artisan outlet design clean, products are nicely arranged and easy to explore
RandomNamehiexy –
uplandcovevendorcorner – Vendor corner feels helpful easy browsing and clean layout overall
Diegonit –
While checking out different artist and band pages online, I stumbled upon open this band site – The style is really appealing, and the presentation feels smooth and well structured, making it enjoyable to browse through the content.
Robertcroth –
Users who enjoy bright and structured online stores often interact with platforms such as Harbor Sunlight Commerce Point – The design focuses on clarity and ease of use, making browsing simple and efficient while maintaining a friendly and visually appealing digital marketplace atmosphere.
RandomNamehiexy –
nightorchardretailmart.shop – Bought a gift last week, packaging felt really premium honestly.
Morganmof –
While browsing city lifestyle inspiration platforms I discovered a Seattle urban website that presents modern living content with a dynamic visual approach making it engaging for readers interested in contemporary urban culture seattle lifestyle trends hub – The site feels modern and energetic, focusing on urban experiences
Willierex –
People who enjoy organized digital commerce often engage with sites like Harbor Upland Commerce Efficiency Hub where items are displayed in a clean and structured layout – The interface ensures product discovery feels fast, intuitive, and simple while maintaining a smooth browsing flow.
mostbet_fdpl –
mostbet otevřít v Česku [url=www.mostbet2016.help]mostbet otevřít v Česku[/url]
DennisRof –
During a detailed review of online boutique hall platforms focused on clarity and structure, I noticed visit this velvet brook hall – The information available is useful, and everything feels neatly arranged, making it simple and easy to follow throughout the browsing experience.
Marvinhus –
In exploring online handmade hubs I found a platform that blends creativity with structured and accessible design system where Walnut Cove artisan marketplace portal offering diverse artisan creations with strong visual organization layout clarity – It showcases handmade artistry while building a connected community of independent creators globally online network
Peterdrult –
Users who prefer streamlined ecommerce systems often explore sites like Goods Vale Cove District Network where products are structured neatly – The interface ensures users can compare items easily while navigating through clean and simple categories.
togbinfda –
Very basic run of the mill casino with your average selection of games. If you’ve played it one of these types of casinos and you’ve plated them all. The layout of the website, selection of games, and customer service are all basically the same. They do have free tournaments for slot machines and such but you do need to deposit between to qualify for the winnings. I’ve read some bad reviews regarding the withdrawal process but haven’t experienced it personally. Overall, seems fine but nothing special Raging Bull casino likewise uses a stringent verification process in order to ensure that gamers are who there is a saying they are plus that they will be of legal age to gamble. They may ask players to submit reports of private identification paperwork for instance a passport or driver’s license. The top prize quantity of a jackpot feature game varies based on the sum wagered and whether or not the special reward was won inside the previous pulling. Jackpot is applied with tiles designated one to 9 and looks like a counting container. Players need to move the dice in addition to choose the quantity on the 1 dice or both. If you want to play this specific game, you need to” “guarantee good luck and fortune.
https://alojat.mx/high-stakes-fun-at-starspinscasinouk-high-roller-section/
All you want to do will be visit the recognized casino website and create a merchant account. Raging Bull Casino features not only some sort of wide range of games, although also unique and even profitable promotions plus Raging Bull on line casino no deposit requirements. Almost every on line casino game has some sort of bonus offer or even ongoing promotion. For further clarification and accurate information on this issue, you can contact the help service or the particular corresponding section about the official website. Bellagio in Las Vegas, USA is the most popular casino and the biggest casinos in the US. Whenever you feel like playing a casino or a blackjack online, you might have felt like going to the USA especially the Las Vegas, and playing the favorite game in the casino. Bellagio can be one of the best casinos in the country.
Robertlig –
While exploring digital trading knowledge hubs for clarity and educational structure, I noticed during research phase Harbor Trade Learning Center integrated into contextual listings – revised impression: explanations remain simple and well structured, supporting quick comprehension of trading-related information overall.
WilliamCholi –
While searching retail shop sites I discovered a store that highlights clean design and simple product arrangement making it convenient for users to browse without distraction or complexity simple online product hub – The site feels structured and clear
RobertBRora –
During research into modern and simple eCommerce vendor halls, I explored browse this mint vendor site – The interface is uncluttered and easy to use, and browsing feels smooth and efficient.
DennisJab –
While browsing different online marketplace directories for vendor ecosystems, I came across a platform where the Harbor Birch vendor showcase appears integrated within the page structure, and it presents a smooth browsing flow – Vendor hall shows diverse listings with smooth user experience today and overall navigation feels intuitive for new visitors exploring categories.
JerryIceno –
While reviewing a variety of resources, I found check this out – The information is delivered in a clean and understandable way, making it accessible to a wide audience without sacrificing professionalism or depth.
Edgarheamy –
semaglutide insomnia: do you lose weight on rybelsus – no prescription needed pharmacy
Joshuareash –
While researching structured commerce hub platforms and their content variety, I explored browse this velvet grove commerce space – The site offers excellent options, and I like checking listings regularly because the browsing experience feels smooth and well organized.
DonnieMeaxy –
Many digital shoppers today prefer streamlined online hubs that connect them directly to curated listings and reliable product information, particularly when navigating platforms such as Ocean Trade Hub Link which emphasize accessibility and a user-centered browsing experience designed to reduce friction, allowing visitors to move between sections seamlessly while maintaining confidence in the platform’s reliability and consistency.
Joshuawounk –
People who value stylish ecommerce platforms often browse platforms such as Harbor Studio Vendor Collective where creative product showcasing is central to the experience – The interface highlights vendor items in a polished studio environment that enhances appeal while ensuring smooth navigation and easy product discovery.
RobertGox –
Users who appreciate modern vault ecommerce design often browse platforms such as Ivory Vault Ridge Elite Hub where items are shown in a clean and structured layout – The design creates a premium browsing experience that feels curated, minimal, and easy to navigate from start to finish.
Raymondtrags –
People who prefer modern ecommerce collectives often browse sites like Harbor Collective Teal Hub where items are presented in a clean layout – The design ensures content appears curated, visually appealing, and easy to navigate throughout the platform.
Robertbaf –
While searching for helpful local guides I found a Lochwinnoch website that shares community focused information in a warm and inviting style making it useful for anyone interested in learning more about the area community friendly info hub – The site feels supportive and easy to browse
TracyLiz –
While analyzing different adventure gear storefronts online, I focused on how efficiently users can browse categories and products, and during that process I discovered Adventure Outpost Storefront within related browsing paths – revised note: the design supports easy exploration, maintains clarity across pages, and ensures a seamless and efficient overall browsing experience.
RandomNamehiexy –
uplandharborcraftmarketplace.shop – Navigation could improve but products are unique and cool.
Kennethtesse –
While searching ecommerce vendor platforms I discovered a marketplace site that categorizes items clearly making browsing intuitive and helping users quickly find and understand products structured retail marketplace page – The layout feels clean and user focused
AndrewSaple –
During research into structured trade platforms, I explored browse this raven commerce house – The design is practical and clear, and information is arranged in an easy-to-read and logical format.
Dannyevoni –
During research into structured ecommerce systems and digital storefronts, I noticed Harbor room vendor guide – it provides a smooth interface with clearly defined sections that support efficient browsing and help users explore a wide range of products effortlessly.
RobertOpise –
While studying online commerce platforms and their interface performance, I came across visit violet harbor commerce world – The layout is impressive, and browsing products feels fast and convenient due to its organized and modern design.
FrancisHit –
While reviewing several online resources for comparison, I came across visit this campaign page – The overall presentation feels organized and thoughtful, guiding readers naturally from one section to another while keeping the information clear, accessible, and easy to follow without unnecessary complexity or confusion.
WilliamFlodo –
Online visitors who enjoy browsing affordable product collections typically prefer platforms with clear structure, and while exploring they might find plum cove value market presenting a variety of useful goods in one place – A user centered marketplace designed for smooth transactions and accessible pricing across different categories.
Joshuabeirl –
People who prefer gentle ecommerce ecosystems often engage with sites like Meadow Lantern Commerce Network Hub where items are displayed in a soft structured design – The browsing experience feels smooth, calm, and easy to understand throughout the store.
AntonioFug –
Users exploring warm themed ecommerce platforms often appreciate how cozy visual design improves browsing comfort when visiting sites such as Honey Cove Treasure Vault Hub where product presentation feels soft, inviting, and carefully structured for easy navigation – The warm theme design creates a cozy browsing experience that feels pleasant and well organized, allowing users to explore products comfortably without visual overload or confusion.
Danielelure –
Users who enjoy responsive trading platforms often engage with sites such as Wave Harbor Trading Central where information is updated clearly and consistently – The interface supports fast comprehension and smooth browsing, allowing users to stay informed while navigating an active and structured environment.
Craigtrist –
While browsing classic rock websites I came across a Manic Street Preachers themed page that offers nostalgic and structured content about the band making it enjoyable for users exploring their musical journey and background band storytelling archive – The content feels well arranged and nostalgic throughout
Robertemurn –
While reviewing several niche outdoor supply marketplaces, I focused on interface consistency and how easily users can transition between product categories CoveExplorerGoods – revised note: the layout remains user friendly and consistent, ensuring a smooth browsing path across all sections.
RobertErymn –
While browsing e commerce websites to compare layout and functionality I discovered a platform showcasing retail marketplace space – the interface appears simple and the structure supports a smooth and product focused browsing experience without unnecessary complexity
BarrySlemo –
As I explored modern interpretations of bazaar-inspired website layouts, I noticed visit cobblestone display – The site feels bright and expressive, and moving through it provides a lively and enjoyable browsing rhythm.
DavidKes –
While analyzing online craft marketplace platforms for design and product quality, I checked see upland harbor creative craft market – Navigation could be improved, but the products are unique and cool and feel refreshing.
Merrillhox –
E-commerce experience analysis often highlights the importance of structured design systems and intuitive browsing pathways especially when reviewing platforms such as Lunar Market Design Studio which is often described as a modern retail concept integrating clean design principles with efficient navigation and user-focused presentation – this leads to improved usability.
Felixloasy –
As part of my analysis of similar tools, I came across explore this link – The layout supports a smooth reading experience, allowing users to navigate through sections efficiently while understanding the content without confusion.
Dannyevoni –
In my exploration of digital vendor environments and ecommerce design structures, I observed Vendor room product hall – it delivers a balanced layout that improves product visibility and ensures users can browse categories smoothly while maintaining a clean visual experience.
Brentgop –
People who enjoy simple commerce hub designs often explore sites like River Frost Trade Direct House Hub where items are arranged in a structured format – The design ensures browsing feels easy, intuitive, and visually consistent across all product categories.
Edgarheamy –
over the counter antibiotics: over the counter antibiotics pills – prescribed antibiotics online
HerbertKed –
People who appreciate cohesive branding in online stores often browse platforms like Stone Collective Gilded Trade Hub where products are arranged with elegant consistency and modern design principles – The layout ensures a premium feel by maintaining visual balance, helping users explore items in a smooth and aesthetically pleasing environment.
Charleswab –
While reviewing shopping sites focused on organized presentation I discovered a platform showcasing product district page – the structure feels balanced and the range of products is displayed in a clear and user friendly format
Davidcarne –
While reviewing user-friendly online stores with seasonal design inspiration, I came across visit cozy retail spot – The layout is balanced and welcoming, and navigation feels simple and effective.
Josephslige –
While searching online for concept focused resources I found a platform that highlights cultural and informational themes in a structured way making it useful for users interested in modern ideas and digital perspectives cultural ideas exploration page – The site feels thoughtful and well organized
CalebAbado –
While testing different vendor studio platforms and evaluating performance quality, I came across explore walnut cove vendor studio – The experience is great so far, and everything loads quickly while working smoothly without any noticeable issues during navigation.
Williammoime –
While exploring several informational outdoor supply sites, I focused on how clearly each one communicates product details and supports quick decision making for users RidgeCoveTrading – updated observation: the presentation style is straightforward, making it easier to absorb information and navigate smoothly across pages.
Brianthuck –
Design-focused consumers frequently appreciate platforms such as Functional Design Depot – The emphasis lies in merging usability with aesthetic restraint, resulting in gear selections that are both visually clean and highly effective, supporting a lifestyle centered around simplicity, reliability, and long-lasting functional value in everyday carry products.
Dennismen –
Many consumers now prefer online artisan platforms that emphasize handmade authenticity and transparent pricing structures Craft Heritage Network – helping them build trust in independent creators while enjoying a diverse selection of culturally inspired goods available worldwide online.
RichardJap –
During a detailed look at various health-related resources, I encountered see more info here – The structure supports clarity, ensuring that readers can easily understand the material without struggling through complex explanations.
RandomNamehiexy –
valeharborcraftemporium.shop – Site works well on phone, checkout was smooth today.
DavidCathy –
In my exploration of digital vendor environments and ecommerce design structures, I observed Vendor room product hall – it delivers a balanced layout that improves product visibility and ensures users can browse categories smoothly while maintaining a clean visual experience.
RickyAdaph –
People who prefer visually curated online shopping often engage with platforms like Stone Galleria Ginger Art Market where products are presented in a stylish and flowing gallery format – The layout enhances clarity and engagement, making browsing feel seamless, organized, and aesthetically refined across all categories.
MichaelJisEe –
As part of studying commerce hub usability and structure, I explored check this wave harbor hub site – I appreciate the effort here, and the site feels polished and user friendly with clear navigation throughout.
FosterGoT –
While exploring niche online marketplaces focused on rustic aesthetics I found a platform that emphasizes simplicity and functional design with a calm browsing flow featuring mountain outpost shop – the site gives a grounded feel with minimal clutter and easy navigation that makes browsing comfortable and straightforward overall
RichardSkike –
As part of a deeper look into how outdoor brands present their products online, I explored browse alpine outpost now – The design is refreshingly minimal, and the navigation feels consistent, making it easy to move around without needing to think too much.
WilliamTEM –
While searching for luxury stay inspiration I found a lodge focused website that presents premium accommodation with beautiful imagery and an inviting tone making it suitable for users planning upscale travel experiences luxury lodge retreat visuals – The site feels elegant and immersive overall
Michaelglism –
While exploring several informational outdoor supply sites, I focused on how clearly each one communicates product details and supports quick decision making for users RidgeCoveTrading – updated observation: the presentation style is straightforward, making it easier to absorb information and navigate smoothly across pages.
DonaldJenly –
Many users exploring e-commerce platforms value vendor networks that present structured and reliable product listings with improved transparency for enhanced shopping experience Commerce Vendor Hub – This structure improves browsing flow and helps users quickly identify relevant products across categories and better organization online platforms for enhanced shopping experience
JeffreyRap –
While exploring digital shopping platforms with cohesive themes I came across a site featuring alpine trade network – the layout feels organized and the browsing experience is smooth with a refreshing and structured interface
Josephavery –
During my search for visually appealing and user-friendly websites, I noticed check this collection – The layout feels fresh and contemporary, making it easy for readers to engage with the content while enjoying a seamless and comfortable browsing experience throughout.
Brianlix –
While researching structured vendor atelier websites and their usability design, I explored browse this wave harbor artisan atelier – Browsing here is pleasant, and categories are simple, clear, and easy to navigate across all sections.
Devinzet –
People who appreciate well organized online marketplaces often browse sites like Harbor Acorn Commerce Vendor Hall where listings are grouped logically for better navigation – The interface focuses on clarity and structure, ensuring users can move through categories easily while maintaining a smooth and consistent shopping experience.
Neiroset dlya referatov_acOi –
нейросеть реферат [url=https://nejroset-dlya-referatov-23.ru/]нейросеть реферат[/url] .
ChrisLet –
During an exploration of structured artisan boutique platforms, I discovered visit velvet brook craft hub boutique – I’d recommend this to anyone who loves handmade goods since the products feel original and well made.
Edgarheamy –
what happens when you stop taking rybelsus: semaglutide life – top online pharmacy
StevenCot –
As I explored different examples of straightforward website designs for online stores, I checked see aurora shop here – The layout is clean, and browsing feels simple without unnecessary complexity.
RaymondArino –
As I explored curated listing platforms and digital resource hubs, I noticed a page that felt intuitive and well arranged, particularly Market house reference page giving users a clean browsing experience with minimal friction – Noticed this recently, seems quite helpful and easy to explore, and it presents information in a way that feels comfortable and consistent throughout.
Scottploli –
Many digital shoppers appreciate artisan marketplaces that highlight handmade creativity and provide structured access to vendor listings across categories Artisan Vendor World – this improves browsing efficiency and supports stronger connections between buyers and independent creators globally across creative markets online platforms
GarthMok –
In reviewing curated marketplace systems and online vendor directories, I observed a well structured layout where informational content introduces Trade hall Canyon Harbor curated listings embedded naturally within the page, enhancing clarity – It offers smooth navigation, organized categories, and a visually consistent shopping experience for users exploring products online
KevinValry –
Users exploring online goods stores often appreciate clean interfaces that help simplify browsing and improve overall shopping efficiency Marble Goods Store Harbor – The layout ensures structured navigation and easy category access allowing users to find products quickly while maintaining a visually consistent experience that supports clarity and smooth interaction across the entire ecommerce platform today.
Williambrire –
While searching travel inspiration sites I came across a cruise focused platform that presents voyage information in an easy to understand format designed for users planning ocean travel experiences sea journey hub – The content feels structured and useful
MichaeldOb –
Users who prefer minimal yet artistic ecommerce environments often find satisfaction in platforms such as Flora Ridge Collection Hub where curated items are arranged in a structured format that supports easy navigation and quick visual understanding of available products – The design approach combines floral elegance with a clean hub structure that improves usability and browsing comfort
Brianlix –
During an analysis of vendor atelier interface design and structure, I noticed open this wave harbor atelier network – Browsing here is pleasant, and categories are clearly defined and easy to navigate across the platform.
Jaredfub –
While exploring vendor marketplaces and commerce directories on my phone, I came across a site containing Jasper trade harbor hall entry – The branding is solid and memorable, though the pages were surprisingly slow to load during my visit today.
BennyFek –
Across sandbox ecommerce environments and farm inspired UI templates, developers observed embedded navigation content containing wild vendor orchard workshop entry within central layout structure, but despite the natural branding direction the product pages do not provide ingredient breakdowns or detailed composition data – Wild orchard feels organic and fresh, however ingredient lists are completely absent across all product views in the system
Antonioblods –
People who appreciate well organized online marketplaces often browse sites like Harbor Chestnut Commerce Vendor Hall where listings are grouped logically for improved navigation – The interface focuses on clarity and structure, ensuring users can move through categories easily while maintaining a smooth and consistent shopping experience overall.
RichardCom –
During research into clean and easy-to-use digital storefronts, I explored browse autumn trade spot – The layout is straightforward, and browsing across pages feels comfortable and efficient.
Danieldes –
Many shoppers exploring artisan discount hubs appreciate structured platforms that highlight price reductions while still ensuring handmade authenticity across product listings Artisan Price Drop Hub while maintaining transparency – such systems help users confidently explore craft items while benefiting from consistent quality and attractive pricing opportunities across categories.
DavidOdomy –
While going through multiple niche listing pages and online discovery threads, I found something that seemed well structured and easy to interact with, especially where Harbor coast vendor hub appeared – the browsing experience feels smooth overall, with clear organization that makes it comfortable to explore again later.
Charlesbus –
During a final comparison of retail mart platforms, I found see night orchard retail mart hub page – I purchased a gift last week, and the packaging felt premium and well executed, making the whole experience feel genuinely high quality.
RichardLam –
As I browsed through various counselling services online, I encountered learn more here – The layout and wording create a welcoming experience, making it simple for visitors to absorb information while feeling supported and guided throughout their visit.
Thomassuict –
People who prefer structured digital vault platforms often explore sites like Elm Harbor Secure Vault where content is arranged clearly – The design ensures browsing feels safe, organized, and visually uniform throughout the experience.
CharlesVam –
While exploring minimal personal websites I found a straightforward platform that emphasizes clarity and simplicity making it suitable for users who prefer uncomplicated and clean digital spaces personal identity page – The site feels relaxed and user friendly
Bobbymow –
While analyzing credibility in online vendor atelier platforms, I checked see harbor trail vendor site – The platform feels trustworthy, and the information appears accurate and structured in a user-friendly way.
RandomNamehiexy –
During exploration of digital marketplace sites I came across Amber Harbor vendor lounge marketplace – The aesthetic is nice, but the lounge section mostly shows blank pages, which weakens the platform’s credibility.
Frankten –
People exploring modern ecommerce hubs often appreciate when websites use structured layouts that reduce clutter and guide attention toward product groups and categories in a way that supports faster decision making and more enjoyable browsing across multiple departments Opal District Market Navigator – The design emphasizes clearly segmented sections and well labeled categories that make it easy for users to browse logically arranged products while maintaining a comfortable and distraction free shopping environment from start to finish.
ErnestPed –
Market demand for structured online platforms continues to grow as businesses seek more reliable digital infrastructure and stable ecosystems Marketplace guild structured platform guild systems provide a framework that ensures consistency across listings and improves user confidence – Structured retail guild environments are often preferred for their balance of flexibility and control
LarryJar –
During a casual exploration of vendor sites and niche commerce hubs, I found a platform featuring Cove Juniper goods room listing link – The layout looks interesting at first, but I’m still not sure what exactly they offer since the design makes it slightly confusing.
NathanBathy –
While comparing different product-focused retail websites, I discovered explore goods collection – The design is refined, and browsing feels smooth with well-organized sections.
RonaldNem –
While scanning through various online suggestion threads and niche directories, I noticed something that felt easy to use and well structured, especially when seeing Copper Cove access portal included – this appears to be a solid platform with clear content and simple navigation for users.
MichaelUrifs –
During a recent look at digital vendor spaces I came across a platform that places useful information in a clean format where the Sweet Harbor market hall listing is embedded within descriptive sections, helping guide navigation – Market hall appears colorful and well priced today while giving shoppers a simple and enjoyable browsing experience overall.
Edgarheamy –
stromectol reviews: oral ivermectin cost – stromectol reviews
Edmundspelo –
While comparing artisan marketplace designs and their catalog variety, I discovered browse oakcove creative hub – The collection is diverse and interesting, making browsing feel enjoyable and worth extended attention.
Albertfog –
People who enjoy structured cozy ecommerce platforms often engage with sites like Ember Meadow Goods Market where products are displayed clearly – The design ensures navigation feels smooth, warm, and visually easy to process.
melbet_itet –
melbet bonus machines à sous [url=http://melbet38470.help/]http://melbet38470.help/[/url]
mostbet_gxer –
mostbet app setup [url=https://mostbet62741.help/]https://mostbet62741.help/[/url]
Edwardgox –
While exploring various digital shopping environments I noticed within the main content flow a section displaying cotton meadow goods marketplace and although the soft visual theme is appealing, repeated session interruptions reduce efficiency and make it difficult to maintain a smooth browsing experience across categories.
pinup_nspa –
pinup signup [url=https://pinup28750.help/]https://pinup28750.help/[/url]
RandomNamehiexy –
oakmeadowvendorcollective.shop – Really clean product photos, descriptions are helpful too.
Hassanoraxy –
Online commerce platforms increasingly rely on structured frameworks that allow better coordination among vendors and improved buyer experiences such as Digital Commerce Hub – these frameworks help reduce operational friction and ensure a more consistent user journey across different product categories
JosephceT –
While going through several creative service websites, I came upon visit this page – The layout feels intentional and neat, helping create a positive initial impression for visitors exploring the content.
Larrydioth –
As I reviewed several handcrafted-style eCommerce platforms focused on curation and design quality, I found check golden artisan outlet – The interface feels creative and balanced, and browsing through items is smooth with a strong sense of thoughtful arrangement.
Herbertgog –
People drawn to artisan-inspired ecommerce platforms frequently look for visually cohesive layouts that enhance browsing comfort and product understanding within Chestnut Cove Craftsmanship Bazaar – everything is designed to feel approachable and premium at the same time, ensuring a seamless experience – handcrafted details are showcased clearly without overwhelming the user.
Kevinhek –
While reviewing ecommerce vendor pages I noticed Moon Harbor trade lounge hub – The lunar-inspired layout looks polished, but missing product photos reduce confidence when trying to assess quality or product details.
LionelSop –
As I continued browsing through online directories and marketplace-style resources, I noticed something that stood out for its minimal design, particularly with Copper Harbor vendor link hub – the layout is simple, which helps make everything easier to understand quickly and without unnecessary complexity.
TerryAmita –
As I compared different artisan marketplace designs for usability, I came across explore upland cove goods hub – The interface is clean and clear, and everything is easy to find quickly without confusion.
ThomasWef –
coworking website coworking space dubai
RandomNamehiexy –
While evaluating sandbox ecommerce systems and vendor marketplace prototypes, testers encountered a mid page component featuring ridge amber vendor parlor console hub link inside layout structure, and despite the pleasant amber ridge theme suggesting warmth and stability, the vendor parlor area appears unfinished and placeholder-like which impacts user trust and experience during interaction testing and UX evaluation sessions
Lewisnip –
In exploring various vendor ecosystems online I found a structured interface that guides users effectively where Vendor hall caramel listing portal Vendor hall caramel listing portal embedded mid-content improves discovery – The platform delivers smooth navigation and well grouped listings making it easier for shoppers to browse different product categories efficiently and comfortably.
RobertEloms –
While exploring ecommerce directories I came across a central page block showing creek harbor product trade hall and although the visual theme is refreshing and nature based, the malfunctioning search filter makes navigation frustrating and slows down product discovery significantly for users.
Melvinmus –
During analysis of outdoor retail websites focused on simplicity, I compared navigation systems and content presentation, and in the middle of that review I found ValeOutpost Navigation Store – revised note: the browsing experience is clean and intuitive, making product discovery feel natural, efficient, and free from unnecessary complexity overall.
Jamessib –
E-commerce platforms focused on handmade goods often highlight creativity, smooth browsing experience, and user friendly design principles Crafts Under Night Portal providing structured listings and responsive interface behavior for enhanced shopping satisfaction overall online today – It helps simplify product discovery while maintaining a visually appealing storefront
WilliamHef –
As part of studying minimalistic and nature-inspired website layouts, I explored check forest gear shop – The interface is clean and relaxing, and browsing feels intuitive and user-friendly.
RandomNamehiexy –
pebblecreekcraftexchange.shop – Will order again next month, hope they restock soon.
RandomNamehiexy –
While studying structured online goods zones, I came across visit gilded lake goods hub – The interface feels well organized, and navigating through content is straightforward and comfortable for users.
Miltonbam –
During browsing of discount trade platforms I came across Nightfall trade house commerce deals hub – The offers looked great, but I left after the checkout process raised doubts about safety and reliability overall.
TimothyJaida –
During a casual browsing session across online marketplace hubs and curated listings, I came across something that felt well organized and user-friendly, particularly references like Meadow coral hub portal – The site is pretty decent, and navigation works smoothly without confusion, so the experience feels simple and comfortable.
AaronloX –
Users who enjoy efficient digital marketplaces often prefer platforms such as Quick Harbor Trade Lane where product categories are clearly organized for fast browsing – The design emphasizes intuitive flow and structured navigation, making the entire shopping journey feel smooth, responsive, and easy to understand from start to finish.
Vernonshemy –
While reviewing sandbox ecommerce systems and UI marketplace frameworks, testers found a central module featuring marble harbor trade vendor gallery showcase console node integrated into structured layout, and despite the refined marble aesthetic, all images remain low resolution which reduces visual quality during usability testing and evaluation cycles
RamonMew –
While scanning different online vendor directories I discovered a mid page listing featuring creek harbor vendor trade house portal and although the design is neat and structured, it closely resembles tradehall which makes it hard to remember which version contains which features.
Robertshito –
Modern online vendor platforms often prioritize organization and usability to ensure customers can locate products without unnecessary effort or confusion Nightfall Commerce Hall – It provides a visually structured environment where categories are easy to distinguish and users can move between listings with minimal distraction or complexity
Edgarheamy –
stromectol reviews: stromectol reviews – stromectol reviews
JeromeSeits –
In exploring online trade marketplaces I came across a well designed interface that emphasizes structured browsing and easy product discovery Tradehouse coastal marketplace portal view and it provides a smooth user experience with clearly defined categories and visually consistent design elements that make navigation simple and efficient for all users today
RobertJouth –
While exploring curated online shops with a focus on aesthetic harmony and smooth navigation experience I encountered within the mid section of the page Soft Velvet Supply embedded into the structure – revised observation the browsing experience remains calm structured and visually consistent allowing users to move through content without distraction
IssacFak –
As I tested several eCommerce retail district websites, I checked see this oak cove retail page – The performance is smooth and consistent, and navigating through content feels easy without any lag or confusion.
GustavoAnivy –
During an exploration of contemporary retail designs with boutique aesthetics, I discovered visit frost fashion hub – The layout is sleek and organized, and browsing feels visually engaging without clutter.
RichardAwaib –
During review of online trade platforms I noticed Oak Cove goods hall listing – The design is simple and easy to follow, but the absence of a search tool makes it frustrating to find specific products quickly.
Russellsmumb –
During a general browsing session across niche resource hubs and listing directories, I found something that felt well structured and easy to use, particularly references including Meadow coral trade access – The site is pretty decent, and navigation works smoothly without confusion, so it’s easy to explore everything comfortably.
MiltonLayed –
During usability analysis of ecommerce sandbox environments and UI prototype systems, testers identified mid page modules containing plum harbor vendor room showcase access node within layout structure, and despite the fresh plum harbor theme, the vendor room remains empty which weakens engagement and usability during testing and evaluation processes
DarrellUnoth –
While browsing different craft exchange platforms and evaluating product availability and shopping experience, I came across explore pebble creek craft exchange – I will definitely order again next month because I’m hoping they restock some of the items I liked.
CoreyRedia –
When exploring online marketplaces dedicated to handmade artistry, users occasionally come across platforms such as handcrafted treasures hub presenting a wide assortment of unique items and encouraging visitors to discover new artisan pieces while enjoying a well-structured browsing interface. – A creative online destination that showcases originality, craftsmanship, and engaging product discovery.
Royalapoma –
In the middle of evaluating ecommerce platforms I noticed a content feature containing royal cove vendor room portal and while the design looks polished and premium themed, the blurry product images make it difficult to properly assess items which reduces overall shopping confidence.
MichaelPlern –
While researching structured artisan outlet websites and their browsing efficiency, I explored browse this vale cove outlet space – The site is helpful for discovery, and I was able to find several interesting options quickly thanks to its simple and clean design.
Peterjut –
While studying soft-themed eCommerce artisan platforms, I noticed open rose trail mart hub – The layout feels balanced and soothing, and navigating through products is easy with clear and attractive organization.
TommyRipsy –
A consistent theme across the platform is accessibility, ensuring that essential tools are always within reach and clearly labeled for user convenience Chestnut Harbor Shop Desk Interface this helps reduce friction in daily tasks and supports smoother interaction with the vendor management system overall.
AntonioRhind –
While browsing different online trade hubs and marketplace pages, I noticed a platform containing Juniper market harbor hall portal link – It has potential and looks interesting, so I’ll likely revisit it after some time to see updates or changes.
Peterpiolf –
While browsing through different niche discovery threads and marketplace listings, I came across something that felt stable and easy to use, especially when seeing Flora harbor vendor link included – Everything loads fine, and the experience was smooth and pleasant, making navigation straightforward and comfortable.
RandomNamehiexy –
Shoppers interested in versatile online exchanges often search for platforms that combine product diversity with seamless navigation systems and provide a reliable environment for browsing and selection across multiple categories foundry goods exchange which connects various sellers and buyers in a structured environment designed to improve trading efficiency and product accessibility across categories. – A balanced exchange platform enabling smooth transactions and improved access to varied product markets.
RandomNamehiexy –
While reviewing ecommerce vendor systems and UI staging environments, analysts encountered mid layout content featuring meadow quartz vendor hall gateway access node embedded in structure, and despite the crystal quartz aesthetic suggesting clarity and order, the market hall is entirely empty today which reduces usability during testing and evaluation cycles
EdwardSEP –
During a detailed review of online artisan emporium websites focused on delivery performance and product care, I noticed visit solar orchard gift emporium – It’s great for gift shopping since everything arrived safely and in perfect condition.
CharlesBic –
While browsing online vendor platforms I noticed within the main content area a listing featuring crown harbor trade vendor hall portal and although the layout is clean and professional, it mostly contains placeholder text which makes it difficult to assess actual functionality or value for users.
RandomNamehiexy –
While reviewing different commerce hub websites and evaluating their usability and content clarity, I came across explore upland canyon commerce hub – The platform seems like a decent place overall, and the content is useful, clear, and easy to understand while browsing.
Edgarheamy –
ozempic vs rybelsus: max dose of rybelsus – п»їinternational drug mart
RandomNamehiexy –
ferncovevault – Vault style neat, content feels organized and carefully structured overall
SteveFaupe –
Users browsing modern e commerce sites often look for organized layouts, and while doing so they might discover sunbrook exchange lane featuring clearly separated categories that make product selection more efficient and intuitive. – A streamlined exchange platform focused on improving accessibility and shopping clarity.
RicardoZoold –
I came across this platform while browsing online trade directories Kettle Crest trade house and the deals look suspiciously cheap, which makes me hesitant until I see more trustworthy reviews.
Matthewthump –
As I continued browsing through various online resource collections and listing hubs, I came across something that felt efficient and well arranged, particularly with Harbor vendor Hazel page – The clean design and good structure make browsing feel comfortable and simple, giving a smooth experience without unnecessary friction.
LeroySuese –
Many reviewers appreciate the minimalistic design approach, especially when opening Cloud Cove Product Flow Portal which streamlines navigation – the goods section remains organized and helps users focus on browsing without distraction
KennethSoire –
While evaluating sandbox ecommerce systems and UI vendor prototypes, testers encountered a mid page component featuring orchard quartz vendor hall console hub link inside structured layout, and despite the distinctive quartz orchard theme suggesting rarity and elegance, the vendor hall redirects directly to the homepage which reduces user trust during interaction testing and UX evaluation sessions
RichardNom –
Within the realm of digital storefront experimentation and conceptual web commerce, many observers reference areas in Crystal Cove goods collection page – despite structured navigation and refined styling, the collection area lacks visible items, suggesting a placeholder or intentionally sparse presentation strategy
RandomNamehiexy –
As I explored various retail district platforms online, I checked see upland cove shop hub – The layout feels simple and clean, and it is comfortable to browse with smooth navigation and clear structure.
Lonniefergy –
As I explored examples of carefully curated online artisan shops, I checked see this artisan link – The layout feels intentional and creative, and browsing offers a visually pleasing and organized experience.
DavidKes –
During research into structured craft marketplace websites, I explored explore upland harbor craft collection market – Navigation could improve, but products are unique and cool, giving the platform creative value.
EugeneMof –
Users exploring modern online stores frequently appreciate platforms that streamline shopping processes, and during their journey they may encounter suncove digital atelier shop showcasing structured categories and – it enhances user satisfaction through clean design and efficient product access.
mostbet_twPi –
мостбет вход на сайт [url=www.mostbet29056.help]www.mostbet29056.help[/url]
sweet-bonanza_uiMn –
світ бонанза rtp [url=https://sweet-bonanza83096.help/]https://sweet-bonanza83096.help/[/url]
Michaelbrask –
While browsing through online store directories I encountered Kettle Harbor goods market page – The site looks friendly and well branded, but broken footer links make it frustrating to navigate deeper pages, which reduces trust in the platform’s overall reliability.
Robertvioff –
During a general exploration of curated marketplace listings and online directories, I noticed something that stood out for its clarity and usability, particularly references including Cove honey marketplace hub – The first impression feels nice overall, and everything looks relevant and easy to read, making navigation easy and intuitive.
RandomNamehiexy –
During frontend inspection of ecommerce sandbox platforms and vendor directory UI systems, developers identified a central module featuring harbor quick vendor market house staging entry portal integrated into structured layout, and despite the name implying fast performance, the site loads slowly which reduces usability and perceived quality during testing sessions and evaluation stages
Williamkes –
Many online marketplace users value platforms that combine structured navigation with a broad selection of trading opportunities for better usability TradeNavigator Flow System – It delivers an intuitive browsing experience that helps users efficiently explore all available marketplace sections
Allenvam –
While reviewing digital artisan exchange marketplaces, I came across visit violet harbor creative hub exchange – There is nice variety, and I enjoy browsing sections without getting lost due to the simple interface.
Williamgek –
In various analyses of futuristic online shopping experiments and conceptual retail UI systems, attention often lands on pages featuring Crystal Harbor Vendor Space Interface that maintains aesthetic consistency but lacks tangible product engagement layers – The structure strongly resembles template-based ecommerce frameworks used for rapid deployment.
fdxyikstn –
I Gates of Olympus har de traditionella vinstlinjerna ersatts av Tumble- och kaskad-funktionerna. För att få en vinst måste du landa 8 likadana symboler var som helst på spelets grafiska gränssnitt som består av 6 hjul och 5 rader. Bonusrundan utlöses genom att landa flera scatter-symboler i ett enda snurr. Gates of Olympus 1000 Dice av Pragmatic Play Under åren har Gates of Olympus blivit en stapelvara bland online slots entusiaster. Spelare till höger och vänster faller för det här spelets roliga tema och vackra grafik, vilket gör varje snurr desto roligare. Dessutom innebär den höga volatiliteten hos Gates of Olympus att du aldrig vet vilket pris eller jackpot som väntar dig på din nästa snurr! Gates of Olympus är en spelautomat från leverantören Pragmatic Play. Ta reda på allt du behöver veta om det (RTP, minimiinsats, möjliga vinster).
https://www.coms.it/?p=119748
Utöver traditionella slots hittar man också MegaWays slots och Jackpots, som ger dig en annorlunda och spännande upplevelse. Slots med MegaWays-funktionen innebär att antalet hjul och symboler förändras efter varje snurr. Detta leder i sin tur till att det kan finnas flera tusen olika vinstlinjer att utforska, något som ökar spänningen med varje snurr. Vill du testa att spela Gates of Olympus gratis kan du kika in spelets demo här hos oss! Gillar du då Gates of Olympus slot kan du göra en insättning och komma igång med ditt spelande. Kom även ihåg att se över casinots RTP i sloten och spela ansvarsfullt. Lycka till! We don’t spam! Gates of Olympus är en känd spelautomat från Pragmatic Play. Zeus kan ge dig slumpmässiga multiplikatorer på upp till 500x. Symbolen kan också hjälpa dig att trigga spelets free spins-funktion. Denna slot ger dig innovativa vinstfunktioner och vinstlinjerna har tagits bort. Istället kan du vinna oavsett hur på spelplanen symbolerna än landar – i vår recension får du reda på hur.
Harrydok –
Digital consumers often prefer shopping platforms that prioritize user experience through clear layouts and curated product selections, making the browsing process both efficient and enjoyable from start to finish suncove goods collection gate – The goods atelier offers a refined marketplace structure where users can seamlessly navigate through carefully chosen products presented in an organized and visually engaging format.
Francisjergo –
During a comparison of vendor-based eCommerce studios focused on usability, I came across discover this lavender shop – The layout feels refined and balanced, and browsing products is straightforward with a visually appealing structure.
Edgarheamy –
semaglutide mounjaro: semaglutide life – best online pharmacy
Williamquaft –
Across sandbox UI evaluations and ecommerce vendor prototype systems, analysts encountered structured sections featuring ridge quick house market vendor showcase hub node within page layout, and while the naming suggests improved responsiveness and reduced latency, the platform still feels slow in practice which impacts browsing analysis and usability testing cycles
Freddymar –
As I explored various online listing hubs and curated resource pages, I noticed something that stood out for its clarity and flow, particularly with Meadow honey vendor access – I enjoyed looking around here overall, since the layout is neat and user friendly, helping everything feel simple and easy to access.
Merrillknota –
While browsing commerce hubs and vendor marketplaces, I came across a platform with strong Aurora-themed branding but limited informational content, especially Aurora harbor commerce vendor hall portal – The name is memorable, though the content feels somewhat sparse and underdeveloped.
ozqgrgqjy –
We strictly recommend you to please visit and browse this site on your own risk. All the information available here is strictly for informational purposes and based on astrology and numerology calculations. We are no way associated or affiliated with any illegal Matka business. We abide by rules and regulations of the regions where you are accessing the website. May be it is illegal or banned in your region. If you are using our website despite ban, you will be solely responsible for the damage or loss occurred or legal action taken. Please leave our website immediately if you dont like our disclaimer. Copying any information content posted on the website is strictly prohibited and against the law. 09:15 PM 11:10 PM We are the most trusted platform in india to play games like madhur satta, manipur satta, kalyan satta and many more. In the era of online gaming there are peoples who loves to play games like kalyan matka, manipur matka which are popular form of game of chances that originated in India but among all madhur matka has gained massive popularity due to its crazy nature and risk potential of earning money.
https://jesuslovesnewlondon.com/goat-spins-casino-app-download-apk-what-kiwi-players-should-know/
When it comes to online betting in the game of cricket, numerous betting sites are available. And various factors must be considered while picking the best betting sites in Bangladesh. It’s imperative to thoroughly review all such factors before choosing an online betting site in Bangladesh. The betting site should perfectly suits your requirements and gives you maximum benefits. You can email the site owner to let them know you were blocked. Please include what you were doing when this page came up and the Cloudflare Ray ID found at the bottom of this page. Caesars Sportsbook offers betting on different sports, including cricket betting. They offer plenty of options including a 100% bonus as its welcome offer. It’s currently available in several states, including: Arizona, Colorado, Iowa, Indiana, Louisiana, Michigan, New Jersey, New York, Tennessee, Virginia, and West Virginia.
DavidAbern –
As I analyzed several craft emporium platforms for mobile responsiveness and checkout flow, I found check vale harbor handmade emporium – The site works well on phone, and checkout was smooth today, making the whole process simple and reliable.
RandomNamehiexy –
While reviewing digital artisan bazaar designs, I came across visit mint orchard shop bazaar – The performance is stable, and the layout feels structured and easy to navigate with a reliable user experience.
Gregorydor –
Market researchers often rely on curated platforms that simplify the process of discovering vendors and assessing their service offerings online vendor discovery hub – The discovery hub emphasizes ease of use and structured navigation, helping users efficiently identify suitable vendors across categories
FrankWhobe –
In various frontend prototype reviews and digital commerce experiments, testers frequently encounter platforms such as daisy cove listings hub which display organized product layouts but suffer from unstable backend processes when handling newsletter signups and form submissions across different sessions – The listings hub looks structured but backend responses are unreliable
Miguelretry –
Users exploring online shopping environments often appreciate systems designed to minimize effort while maximizing browsing efficiency and clarity teal cove product studio providing quick loading pages and well structured categories that support easy discovery of items across multiple product groups and sections.
Jameslal –
During a comparison of structured vendor websites focused on simplicity, I came across discover lemon house platform – The layout feels intuitive and neat, and browsing products or sections is straightforward and easy to follow.
RafaelCaw –
During usability analysis of ecommerce sandbox environments and UI prototype systems, testers identified mid page modules containing rain harbor market hall vendor showcase access node within layout structure, and despite the soothing rain theme implying harmony, the hall is filled with broken image placeholders which reduces engagement during testing and evaluation processes
RandomNamehiexy –
mintmeadowgoodsroom – Feels well organized, I didn’t face any issues navigating around.
Josephstync –
During a general exploration of commerce directories and vendor listings, I found a minimalistic trade platform featuring Harbor Bay trading hall entry – Everything feels very to the point, and I like that there are no intrusive newsletter popups appearing everywhere.
Robertasses –
In multiple frontend debugging sessions involving ecommerce templates the daisy harbor room interface shows that harbor room showcase entry appears clickable but ultimately leads nowhere except the homepage removing any possibility of viewing vendor content directly – this creates a misleading user experience during navigation testing
Haroldinhap –
Many online systems aim to replicate the feel of a digital shelf where products are displayed neatly, allowing users to browse through listings as if viewing items arranged in a physical organized space goods room digital shelf – This shelf-style presentation improves visual clarity, making it easier for users to scan products and understand available categories at a glance
RandomNamehiexy –
velvetbrookartisanboutique.shop – I’d recommend this to anyone who loves handmade goods.
Jeffreydit –
While studying digital commerce platforms with a focus on simplicity and structure, I noticed open lemon ridge shop hub – The layout is minimal and clear, and users can easily understand navigation across all sections.
Georgesuh –
During frontend inspection of ecommerce sandbox platforms and vendor directory UI systems, developers identified a central module featuring harbor rain vendor hall staging entry portal integrated into structured layout, and despite the consistent rain harbor branding across pages, the vendor hall appears duplicated which reduces usability trust during testing sessions and evaluation stages
LarrymUh –
Users who prefer visually clean ecommerce outlets often explore sites such as Lemon Artisan Harbor Trade Outlet where products are presented in a simple organized layout – The interface creates a browsing experience that feels warm, clear, and easy to follow across all sections.
Georgeflish –
As I continued exploring various online listing hubs and discovery platforms, I found something that seemed well designed and easy to use, particularly with Harbor pine trade page – The experience is good, and everything seems clear and straightforward here, helping everything feel structured and readable.
Johnnychavy –
While browsing curated commerce marketplaces and vendor directories, I noticed something that felt light and playful in design but not very rich in content, especially Acorn harbor commerce trade hall page – The theme is appealing, but the stock is currently quite limited.
Edgarheamy –
semaglutide online with insurance: semaglutide life – online pharmacy no prescription needed
DavidpautH –
While inspecting demo marketplaces and UI kits, testers found that in the middle navigation region the meadow goods panel loads inconsistently, and even though the branding suggests calm meadow aesthetics, persistent SSL certificate warning issues reduce trust during transactions sessions
Donaldmeabe –
Online shoppers and researchers often rely on calm and well arranged vendor platforms that group products logically, making it easier to evaluate different listings and navigate through multiple categories with ease fern cove trade lounge entry – Vendor lounge feels calm with well structured product categories available, helping users enjoy a simple browsing flow while discovering vendors in a neatly organized digital environment
ClaudeEmpiC –
During UX evaluation of sandbox ecommerce systems and vendor marketplace prototypes, testers found embedded navigation containing solar meadow vendor market room access console node inside structured layout, and although the solar meadow concept feels environmentally conscious, the missing eco badges reduce trust during usability testing sessions
Michaelzidge –
As I explored various craft boutique platforms online, I checked see velvet grove craft collection boutique – A slight typo is visible in the description, but overall I’m satisfied with the product presentation.
Thomasnek –
Users who enjoy structured artisan shops often explore sites such as Oak Dock Artisan Essence Outlet where products are presented in a clean layout – The design ensures browsing feels easy, clear, and visually organized throughout categories.
ArmandoFop –
In the middle of comparing different online platforms earlier today, I stumbled upon explore this resource which seemed like a nice little site, and I found it useful while browsing earlier today thanks to its simple structure and easy navigation.
BennySal –
While going through multiple online resource collections and marketplace listings, I found something that seemed responsive and well organized, especially where Icicle isle entry page appeared – Nice platform overall, and I appreciate how quickly pages load here, which makes the experience feel smooth and efficient.
melbet_xcSa –
melbet ставки [url=https://melbet09374.help]https://melbet09374.help[/url]
EdwardJuist –
While reviewing experimental marketplace UIs, testers found ridge goods room central link inside structured layouts, and despite its placement appearing intentional, after the dash – ridge visuals are pleasant but footer links are completely broken and do not function across any test scenarios performed
Larrymop –
While browsing curated vendor hubs and commerce marketplace listings, I found something that felt nature-inspired and peaceful, especially Alpine cove hall commerce market portal – The branding gives off a cozy mountain shop feel that is simple yet comforting.
Larryuncow –
After going through several cluttered websites earlier today, I came across see this page and noticed everything looked neat and quite easy, giving a smooth and straightforward browsing experience overall.
Irvingsputt –
Users evaluating online vendor ecosystems often prioritize platforms that streamline navigation and present categories clearly for easier comparison across listings and services available fern harbor lounge access – The vendor environment is designed to provide fluid navigation with a clean layout that improves browsing comfort and reduces complexity for visitors
AnthonyAdese –
Across ecommerce sandbox UI evaluations and vendor system prototypes, testers noticed navigation components containing solar orchard vendor market house access hub node embedded in page flow, and although the orchard solar concept implies trust and growth like a healthy marketplace ecosystem, the missing checkout security seals reduce user assurance during usability testing cycles
RandomNamehiexy –
People who appreciate creative ecommerce platforms often browse sites like Ridge Fern Artisan Collective Design Hub where items are arranged in a neat curated layout – The interface creates a smooth browsing experience that feels organized, visually appealing, and easy to navigate.
RandomNamehiexy –
wheatmeadowmarketroom.shop – Clean layout and simple navigation, makes exploring content really enjoyable.
Derrickgeway –
During a general exploration of online directories and marketplace hubs, I found something that seemed clean and well designed, particularly references including Harbor ivory access portal – The site looks professional, and I might recommend this to others as well because it provides a simple and structured browsing experience.
MichaelArege –
While analyzing ecommerce sandbox environments and UI concept builds developers notice embedded links in page structure drift orchard shop portal which seems like a full entry point yet only reveals a small subset of products without deeper catalog structure – The driftwood styling is attractive but functionality feels restricted
Michaellaump –
While going through multiple vendor commerce platforms and marketplace hubs, I noticed almost identical naming patterns across different listings, especially Alpine harbor commerce trade vendor hall link – It created a strong sense of déjà vu while navigating.
Harryeroca –
As part of studying vendor collective usability and product presentation, I explored check oak meadow marketplace collective – The product photos are clean and clear, and the descriptions provide helpful details for each item.
Williamgyday –
During casual research into marketplace listing designs and experimental vendor portals for inspiration and interface comparison across multiple references Dune Meadow vendor parlor index the layout remained structured and content sections were clearly separated improving readability – Simple navigation flow with fast loading pages and stable interface behavior throughout browsing session
Edgarheamy –
ivermectin tablets: cost of ivermectin pill – ivermectin lotion price
AntonioNed –
During research into modern marketplace showcase designs and digital vendor gallery systems for comparison and structure review Pearl Cove online market showcase I found the browsing experience consistent and straightforward which helped avoid any confusion while moving through pages. – The platform loaded efficiently and maintained a clean organized layout
EdmundAlibe –
While reviewing prototype vendor systems with bright and minimal aesthetic direction, analysts identified a consistent sunlit theme but incomplete content structure around a href=”[https://sunharborvendorroom.shop/](https://sunharborvendorroom.shop/)” />sun harbor vendor room interface block which sits within navigation flow, and although Sun harbor appears modern and visually polished, the vendor room provides no descriptive or explanatory content for users exploring marketplace functionality
ScottTAP –
People who prefer practical exchange systems often engage with sites like Harbor River Trading Core Hub where data is displayed in a minimal structured format – The interface ensures users can understand market movements quickly and clearly.
WilliamDom –
Many users highlight that organized vendor systems reduce search time and improve satisfaction, especially when they access Vendor Product Navigator – The layout is frequently described as intuitive and supportive of faster product discovery while keeping navigation consistent and user friendly
RandomNamehiexy –
While searching for simple and clear websites, I came across explore this resource and appreciated how everything is organized here, allowing me to understand the information quickly without unnecessary confusion.
ThomasHah –
As I browsed speed optimized websites, I noticed view clean fast portal – The interface feels really clean, everything loads quickly, and the system runs smoothly, making the entire experience efficient and user friendly.
JamesPsync –
As I continued exploring various online directories and marketplace-style pages, I came across something that felt well organized and easy to use, particularly with Ridge ivory trade link – The browsing experience feels smooth overall, and nothing is complicated or hard to understand, making navigation feel effortless and natural.
StanleyEnfog –
During UX testing of sandbox marketplaces and experimental storefronts, teams identified a central embedded link using willow goods drift entry within layout hierarchy – despite structured design the absence of willow themed artwork makes the page feel incomplete and visually underdeveloped across multiple sections
ReggiePhich –
Exploring online vendor platforms often highlights which sites are optimized for usability and accessibility across different categories Canyon Harbor marketplace entry this platform delivers a smooth and well-structured browsing experience that feels easy to follow and efficient overall for regular usage
Williamgyday –
While checking experimental trade platform designs and marketplace gallery structures for inspiration and comparative analysis across several test environments Dune Meadow commerce showcase pages loaded efficiently and interaction felt smooth without confusion – Consistent responsiveness with clean presentation and well organized content flow overall experience
Justinven –
While scanning through online marketplace lounge directories and vendor systems, I came across a strong amber color theme, especially Amber commerce ridge vendor lounge portal – It looks visually warm and modern, but the contrast issues affect readability quite noticeably.
Daviderado –
While searching for straightforward websites, I came across explore this resource which had a simple layout, making browsing feel really smooth and giving a pleasant experience while moving through different sections.
RandomNamehiexy –
solarorchardartisanemporium.shop – Great for gift shopping, everything arrived in one piece.
JeffreyNor –
People who enjoy artisan inspired online marketplaces often engage with platforms like Brook Flint Artisan Handmade House Hub where items are displayed in a clean and cozy layout – The design creates a soothing browsing experience that feels well structured, calm, and easy to explore without visual clutter.
DanielHed –
People who prefer bright and efficient shopping platforms often explore sites like Sun Cove District Organized Goods Hub where items are arranged in a user friendly layout – The design ensures browsing feels enjoyable, structured, and visually simple for quick product discovery.
Davidhag –
During ecommerce sandbox usability testing focused on coastal color palettes, analysts found a refined teal design language that enhances visual harmony, but identified structural limitations in content grouping within a href=”https://tealcovemarkethall.shop/
” />teal cove market hall navigation node where the teal aesthetic remains consistent and attractive, yet the lack of sufficient categories in the market hall reduces browsing clarity during user experience evaluation sessions
ClaudeFlugh –
While browsing through several online platforms to test usability and speed, I came across something in the middle like visit this quick link which delivered a pretty smooth experience overall, with pages loading quickly and everything working without noticeable issues during navigation.
RandomNamehiexy –
calmcovevendorparlor.shop – Really nice platform, easy browsing and smooth user experience today
Darnellpem –
Frequent online shoppers suggest that streamlined marketplace design plays a crucial role in helping them find relevant items quickly, especially when they access Forest Cove Marketplace Entry which is seen as supportive of efficient browsing and reduced search effort – many reviews highlight better product visibility and improved navigation flow.
Williammot –
During frontend QA cycles, testers observed a central content area featuring dune goods ridge entry gateway embedded within structured layout but suffers from readability limitations due to sandy color blending issues – Dune themed UI feels consistent yet users experience difficulty reading text in bright conditions causing strain
TyroneLouri –
When a platform is well organized, browsing becomes much easier, and this one delivers a smooth experience overall Silk Meadow listing portal I found navigation simple and everything was easy to locate
RandomNamehiexy –
While searching for well designed Hawaiian retreat listings with scenic charm, I discovered a detailed accommodation page worth exploring recently < scenic kona lodging guide – It provides a smooth overview of the property, blending clarity and comfort with a very welcoming informational tone overall
PedroMoorm –
As I continued exploring various online resource collections and curated listing hubs, I came across something that felt structured and readable, particularly with Brook trade jewel page – The platform seems useful, and I found the content quite straightforward today, helping everything feel clear and well organized.
ReggiePhich –
While exploring different vendor directories online, I found a platform that stood out for its clarity and structure during extended browsing sessions Canyon Harbor trade gallery hub the layout feels intuitive and makes navigating through categories smooth and consistently organized for users
Williamdor –
During a relaxed browsing session focused on vendor showcase platforms and experimental marketplace layouts for inspiration and usability insights, I discovered Plum Cove commerce goodsroom hub inside a structured article – Everything feels clear and readable, and I could browse sections easily without distractions as the design remains clean and well organized throughout.
PeterTob –
While exploring commerce directories and vendor marketplaces, I noticed a very new-looking site that appears lightly filled, especially Aurora goods cove commerce room link – It seems fresh, but the small number of items per category feels a bit strange.
RandomNamehiexy –
People who prefer handcrafted ecommerce environments often explore sites like Cove Atelier Vendor Teal Market Hub where items are presented in a creative and structured layout – The design ensures browsing feels smooth, expressive, and visually coherent across all product categories.
Carloswex –
Users who appreciate clean emporium navigation often browse sites such as Timber Grove Commerce Emporium Hub where products are presented in a rich format – The design makes category exploration feel easy, organized, and visually clear throughout the store.
LowellSwofe –
Digital marketplaces benefit from a really nice platform that supports easy browsing and smooth user experience today Calm Cove item portal I enjoyed how clean and organized everything felt
Edgarheamy –
antibiotics cheap: over the counter antibiotics – uti antibiotics online
Edwardchend –
While exploring various websites, I came across <a href="[https://woodharborvendorroom.shop/](https://woodharborvendorroom.shop/)" / access this site which felt like a helpful platform overall, and I might visit again sometime soon since it was fairly easy to navigate.
Terrylaulk –
During UX evaluation of sandbox marketplace systems, testers noted a cohesive teal harbor visual structure that improves interface flow, but the vendor hall lacks real content when inspecting a href=”https://tealharborvendorhall.shop/
” />teal harbor vendor hall entry gateway where the design remains polished and consistent, yet the vendor hall continues to rely on Lorem ipsum placeholder text which impacts usability during testing and system review processes
RandomNamehiexy –
sageharborgoodsgallery.shop – Looks clean and minimal, easy to find information without confusion.
ThomasBeibe –
While conducting usability tests on staged online shop environments, analysts identified embedded links containing meadow dune storefront console link integrated into page hierarchy, and although technically functional, the conflicting natural themes reduce branding effectiveness – Meadow name contradicts dunes, resulting in a lack of visual harmony that negatively affects user engagement and comprehension of the ecommerce platform structure overall
RandomNamehiexy –
velvetgrovecraftboutique.shop – Little typo in description but overall I’m satisfied.
Williamzet –
As I explored various online listing directories and marketplace hubs, I noticed something that stood out for its clarity and organization, particularly with Cove jewel vendor page – The interface is pretty clean, and everything is arranged in a logical way, helping everything feel easy to understand and use.
GeorgeBluef –
Users often prefer vendor platforms where search results load quickly and the interface remains clean and organized Solar Meadow browsing center this creates a smooth experience that helps users find information without unnecessary delays or confusion
Jaredskema –
While exploring conceptual e-commerce supermarket ideas, I came across a very basic but well structured platform that stood out during review hope grocery concept page – The layout is minimal and functional, helping users grasp the idea quickly without distraction or unnecessary complexity
Elmertrurf –
In the process of reviewing online commerce gallery interfaces, I came across Honey Meadow shopfront portal embedded within a minimalist design that keeps focus on content organization – The experience feels smooth, welcoming, and easy to navigate across all sections
Keithhib –
Users engaging with digital storefront systems often appreciate clarity in design, especially when they encounter Meadow Room Browse Station Online and they mention that the layout helps them quickly understand product placement – the structure is frequently described as efficient for comparing items without feeling overwhelmed by unnecessary details
RandomNamehiexy –
A well designed platform improves browsing experience, and this one delivers a simple layout with clean navigation Silver Cove shop gateway I found it comfortable to explore and everything was clearly presented throughout the site
Edwingaums –
During casual review of online marketplace systems and experimental vendor directory designs for UX inspiration and evaluation across several references I discovered Teal Harbor marketplace insight hub – The interface remains clean and structured, allowing users to navigate effortlessly while maintaining clear readability and consistent performance across all sections of the platform
JerryBit –
While researching curated marketplace designs, I found coastal vendor hub and appreciated how the layout maintains visual consistency while separating content logically – The browsing flow feels steady, calm, and highly user friendly throughout
RonaldPop –
As I browsed through various online marketplace sites and vendor hubs, I noticed a seasonal autumn-themed platform, particularly Meadow commerce autumn market hall portal – The theme is beautiful, and it would benefit greatly from authentic user reviews.
WilliamVop –
Clear design improves usability, and this site ensures well organized content so exploring everything quickly is simple River Harbor vendor navigator I enjoyed how easy everything was to follow
Kevinwanda –
People who appreciate efficient digital commerce platforms often browse sites like Harbor Teal Commerce Grid Hub where items are structured in a clean and logical way – The interface makes browsing smooth and easy, with categories that are simple to understand and navigate.
Larrysoats –
While analyzing various online platforms, I discovered look into this which contained interesting content, and I spent some time checking different sections today while exploring its features.
RobertCed –
People who appreciate curated digital collections often browse platforms like Cove Golden Vault Commerce Hub where items are presented in a clean structured format – The design ensures browsing feels consistent, refined, and visually appealing across the entire marketplace.
SteveBunny –
During ecommerce sandbox usability testing with woodland inspired interfaces, analysts observed a strong timber trail branding style that feels organic and grounded, but navigation usability fails when interacting with a href=”[https://timbertrailmarkethall.shop/](https://timbertrailmarkethall.shop/)” />timber trail vendor hall showcase link where the rustic design appears polished and thematic, yet the navigation menu is completely broken which reduces task completion success during evaluation and testing procedures
ThomasMuh –
Across prototype storefront testing and UI review sessions, analysts found embedded cart elements containing echo brook vendor hall console in checkout structure, but quantity updates fail to apply after user changes – Echo brook is catchy and modern, but cart page does not correctly reflect updated product amounts in testing environments
Davidseits –
While reviewing various online marketplaces, platforms with simple navigation and clean layouts often feel more efficient to use Icicle Brook vendor listings the browsing experience here remains consistent and pleasant, helping users locate products quickly without confusion
DavidSnuby –
While browsing through different niche listing pages and resource hubs, I came across something that felt clean and accessible, especially when seeing Mint orchard vendor link included – I like the overall feel here, because it’s simple and easy going, which makes the experience feel light and easy to follow.
CarlosFruff –
While exploring a variety of niche online shopping experiments and vendor hub concepts, I came across Moon Cove vendor showcase – I found the layout inviting and easy to navigate, with sections that encouraged browsing rather than quick exits, making the experience feel more relaxed and immersive.
RobertSmecy –
During casual research into digital trade gallery platforms and online vendor systems for usability comparison and design insights across multiple examples, I found Pebble Pine marketplace overview board placed within structured content – Everything was easy to follow and I enjoyed browsing listings without confusion as the interface stayed clean and responsive.
HenryItara –
While exploring premium wine industry websites, I found a beautifully organized brand page that highlights both product quality and heritage storytelling canadian wine excellence page – The information is detailed and appealing, giving a strong sense of craftsmanship and professional brand identity
Elmertrurf –
During evaluation of vendor-focused online directories and shop systems, I found Honey Meadow trade network space integrated into a balanced interface that enhances readability and structure – The experience feels pleasant, steady, and easy to follow without unnecessary distractions
RandomNamehiexy –
violetharborretaillane.shop – They responded to my email within an hour, nice.
RandomNamehiexy –
Clear structure improves browsing, and this platform ensures smooth experience making browsing very convenient overall today Plum Harbor vendor navigator I found everything simple to use
Williamnep –
While comparing vendor platforms, this one clearly stands out due to its fast loading speed and clean organization Silver Harbor listings page I appreciated how smooth navigation felt and how well structured everything appeared
RandomNamehiexy –
bayharbortradehouse – Almost identical to another bay domain, bit confusing tbh.
RaymondWrall –
Users who prefer simple ecommerce navigation often explore sites such as Trail Commerce Access Harbor Hub where products are displayed in a clean and structured format – The design ensures browsing feels easy, smooth, and well organized, making product discovery quick and straightforward.
HarveyMurdy –
After reviewing several design-focused websites, I encounteredopen this visual page which impressed me since the design feels modern and neat, definitely stands out nicely and gives a clean and appealing browsing experience overall.
Brianstero –
Users who appreciate clean structured shopping platforms often browse sites such as Granite Orchard Vault Store Hub where products are presented in a minimal strong format – The interface creates a browsing experience that feels organized, stable, and easy to follow across categories.
OscarBophy –
While reviewing the footer section of this site, I noticed that the link visit our marketplace – the supposed social navigation element appears misleading because none of the icons actually redirect users to meaningful destinations, making the overall experience feel incomplete and poorly implemented.
Brucemip –
During QA audits of ecommerce helpdesk systems and support pages, developers noticed a contact section containing harbor echo service support panel integrated into the UI, yet email messages sent to support consistently bounce back – Echo harbor feels familiar and structured, but email delivery fails across all tested communication attempts
JerryBit –
While analyzing vendor listing systems online, I visited vendor listing network and noticed how neatly everything is categorized for quick access and discovery – The browsing experience feels structured, calm, and easy to understand at a glance
Edgarheamy –
ivermectin uk coronavirus: stromectol reviews – stromectol nz
RobertCrype –
Many shoppers value vendor platforms where layouts are well organized and sections clearly guide the browsing process Violet Harbor marketplace link the experience feels consistent and helps users quickly find what they need without unnecessary searching
Jasonjes –
During a casual browsing session across marketplace hubs and online resource collections, I found something that seemed structured and readable, particularly references like Cove moon trade page – The browsing experience feels solid, and I didn’t encounter anything confusing at all, which made everything feel simple and clear.
Caseyirrib –
In the middle of comparing vendor marketplaces, I noticed V “content navigation tag” appearing incorrectly formatted, and Cicicleislemarketparlor.shop was naturally placed in the center, while the design feels modern enough and navigation was quite simple to follow effectively.
DamienGearp –
During exploration of online trade gallery platforms and digital vendor hubs for inspiration I noticed Birch Harbor marketplace index page integrated into structured text – pages were responsive and well organized, giving a smooth browsing experience that felt efficient and easy to follow.
RandomNamehiexy –
A well designed site with modern interface ensures browsing feels very easy today and overall pleasant Linen Cove marketplace link I found navigation simple and very efficient
TracyFum –
While researching avant garde digital experiences, I discovered a website that emphasizes experimental structure and visually creative formatting approaches creative experiment web space – The site feels uniquely structured, offering an artistic and experimental browsing experience that differs from conventional layouts
RandomNamehiexy –
pineharbortradeparlor.shop – Nice interface design makes navigation simple fast and quite pleasant
JamesGeori –
Users who prefer ocean aesthetic ecommerce systems often explore sites such as Wave Harbor Coastal Serenity Market Outpost where products are displayed in a light and relaxing format – The design ensures browsing feels smooth, visually pleasant, and easy to explore across all categories of the store.
RobertFrEpt –
While going through different commerce directories and vendor room platforms, I noticed a site that appears unfinished in terms of content updates, especially Autumn vendor cove room portal – The lack of any blog posts makes it feel like the site might no longer be active.
BrianFrErm –
After going through a variety of websites that felt cluttered and inconsistent, I came across <visit this page during my search, and it provided a good experience overall, with content arranged in a clear and easy-to-understand manner.
RobertUnden –
While comparing vendor platforms, this one clearly stands out for its modern feel and very simple navigation structure Sky Harbor listings page I appreciated how naturally everything flowed and how easy it was to explore
LarryCOR –
People who prefer minimal digital marketplaces often engage with sites like Orchard Lantern Trade Path Lane Hub where items are displayed in a structured format – The design ensures navigation feels intuitive, fluid, and easy to navigate throughout the platform.
RandomNamehiexy –
mintorchardretailatelier.shop – Definitely coming back here for the holiday season.
ltugehixn –
Gates of Olympus wouldn’t exist if it wasn’t for Sweet Bonanza. Yet, thanks to that, the Pragmatic Play team decided to upgrade and refresh the classic Bonanza and turn it up a notch. This results in higher value symbols, a couple of new bonus features, and the fact that the multiplier can be triggered in the bonus game as well. Something that Bonanza is clearly missing. The same goes for the Pay Anywhere feature. While both Bonanza and Gates of Olympus have that feature, the symbols are far more valuable at Gates of Olympus. If one slot series is popular across online casinos worldwide, it’s the Gates of Olympus slots by Pragmatic Play. Since its debut, this Zeus-powered franchise has captured players’ imaginations with great visuals, electrifying mechanics, and impressive win potential. We delve into each slot, let you know where best to play and link to each of our reviews where you can demo the games.
https://www.njmedicareadvisory.com/roll-x-by-smartsoft-a-quick-look-for-indian-players/
The Gates of Olympus Xmas 1000 slot game provides an exciting chance for players to secure substantial payouts, with the possibility of winning up to 15,000 times their initial bet. The allure of this game is heightened by the high multipliers available, ensuring that each spin brings a thrill and holds the promise of significant rewards. As a result, it has become highly favored by individuals seeking big wins through gaming entertainment. Pragmatic Play introduces Gates of Olympus Xmas 1000, an online slot that uniquely combines ancient Greek themes with Christmas festivities. This game is an excellent option for players who appreciate Greek mythology and enjoy the holiday spirit. In addition, it includes a range of unique features designed to enhance winning chances and provide a gaming experience that is both rewarding and enjoyable.
RobertTug –
Across ecommerce prototype reviews and sandbox testing environments, developers identified a navigation block containing elm harbor goods portal node within structured layout, yet image loading errors prevent proper product rendering across catalog sections – Elm trees are strong and symbolic, but the goods room is impacted by broken image links affecting user experience
JorgeDrime –
As I examined site consistency across platforms, I noticed go to this link – the similarities to another known site are so obvious that it feels like viewing a slightly altered copy rather than something original.
RandomNamehiexy –
Users browsing vendor-style websites typically look for clean layouts and visuals that guide them through content effectively Forest Meadow vendor listings page this platform makes it easy to identify relevant details and navigate sections smoothly without confusion
RandomNamehiexy –
sageharborgoodsgallery.shop – Looks clean and minimal, easy to find information without confusion.
RandomNamehiexy –
zencovegoodsgallery.shop – Simple interface clear structure makes finding information very quick indeed
TimothyRar –
During a general exploration of marketplace listings and discovery pages, I noticed something that stood out for its usability and clarity, particularly references including Harbor moss vendor access page – It seems like a decent site, and I’ll probably check it again soon since the browsing experience is easy and comfortable.
Timothyclins –
During casual research into digital vendor showcase systems and e-commerce marketplace layouts for UX inspiration and comparison across multiple examples, I found Plum Cove marketplace goodsroom entry placed within structured content – The interface is simple and readable, making it easy to understand everything while browsing smoothly through different sections.
BrandonSal –
People who prefer handmade ecommerce design often explore sites like Cove Wind Artisan Creative Exchange Hub where items are presented in a neat organized layout – The interface makes browsing feel smooth, visually balanced, and easy to navigate across all product categories.
RandomNamehiexy –
coralharbortradegallery.shop – Great browsing experience overall everything feels organized and easy today
Jasontal –
While researching modern web portfolios and personal introduction pages, I discovered a clean and structured profile that feels highly professional jackonson portfolio showcase site – The page offers smooth navigation and clear information presentation that makes browsing easy and efficient overall
PeterEdurn –
During browsing sessions across online commerce directories, I found a berry-themed platform featuring Berry cove market house entry link – It feels fresh and well-designed, though it’s odd that no contact page seems to exist.
LonnieMit –
After comparing different resources online, I came across visit here which provided a structured experience, helping users find things much faster and navigate through content easily.
AndrewLiemi –
When browsing vendor sites, design matters, and this one ensures a clean layout makes exploring products easy and visually pleasant overall Autumn Cove goods portal I liked how responsive everything felt
RandomNamehiexy –
Users who appreciate well organized shopping sites often browse sites such as Juniper Meadow Goods Flow Hub where products are presented in a clean format – The interface creates a browsing experience that feels intuitive, clear, and easy to navigate.
Jeffreybit –
Users exploring vendor-style platforms often prefer sites where everything is structured clearly to ensure smooth and comfortable browsing experiences Sky Harbor shop access point this one delivers exactly that with simple navigation and well arranged sections
Kennethraics –
While examining the content layout, I found visit this content area – the lounge name implies a premium experience, but the page offers nothing except a blank white background.
RandomNamehiexy –
While comparing vendor platforms, this one clearly stands out due to its nice visuals and layout that make browsing smooth and pleasant Berry Cove listings page I appreciated how visually consistent and easy it was to use
DouglasBes –
Online shoppers tend to favor websites that keep design simple and performance fast for better usability Sea Cove market hub this ensures a consistent browsing experience where users can move through sections smoothly and efficiently
Michaelmal –
While comparing different resources, I came across open this page which made it clear everything looks well structured, helping users move around without issues and maintaining a consistent layout throughout.
Terrellsmali –
During research into digital vendor directories and online trade gallery systems for UI inspiration and UX analysis across multiple platforms, I came across Sun Cove vendor display interface embedded mid-content – The browsing experience felt responsive and visually balanced, and I could move through sections easily while everything remained clear and attractive.
Edgarheamy –
what is semaglutide weight loss: semaglutide life – best online pharmacy no prescription
Quintonnib –
Users who enjoy practical ecommerce outlet layouts often explore sites such as Harbor Stone Outlet Commerce Hub where product categories are clearly defined – The interface emphasizes easy navigation and structured browsing, ensuring users can quickly find what they need without unnecessary distractions or complex layout elements.
ArthurClila –
After browsing through a number of cluttered and less appealing websites, I discovered click here now and appreciated how clean and refined it looked, clearly reflecting the effort behind its design and making the overall browsing experience enjoyable.
JamesLit –
Users who prefer outdoor themed ecommerce experiences often explore sites such as Forest Cove Nature Craft Outlet Hub where products are arranged in a clean and natural format – The design ensures browsing feels smooth, refreshing, and easy to navigate across the store.
RandomNamehiexy –
While analyzing digital storefront systems and vendor directories, I discovered Upland Cove curated listing space integrated into a minimalist layout that improves usability – The browsing experience feels smooth, steady, and very intuitive across multiple sections of content
HarryHoaps –
While exploring artistic and culturally mixed digital platforms, I found a site that merges different themes into a visually engaging structure jeddah brooklyn culture portal – The website feels unique and diverse, with an engaging presentation that blends cultural ideas in a creative and thoughtful manner
GregoryINfob –
While finishing up a long browsing session across various online vendor hubs and commerce directories, I stumbled on a simple-looking platform where Berry Harbor vendor room entry – This ended up being my last stop for today, and honestly it feels decent but nothing particularly special stands out.
Keithmus –
While exploring various marketplace pages for comparison, I came across visit this trade page – the name suggests a refined or active environment, yet the overall feel resembles a deserted storefront with little visible activity or engaging content present anywhere.
RandomNamehiexy –
rainharborvendorparlor.shop – Good organization easy navigation helps users find things efficiently today
Robertpep –
Many online marketplaces can feel cluttered, but this platform keeps a clean design that makes it easy to go through sections quickly Snow Cove product hub I liked how simple everything was and how fast I could find what I needed
RandomNamehiexy –
While evaluating different gallery-style platforms, structured content often plays a key role in user satisfaction Elmwood gallery directory the organization makes it easy to browse through sections while maintaining a consistent and enjoyable navigation experience overall
RandomNamehiexy –
sageharborgoodsgallery.shop – Looks clean and minimal, easy to find information without confusion.
DannyExege –
During exploration of curated marketplace designs and vendor lounge directories for usability testing and interface evaluation across sample systems I found Upland Cove commerce lounge entry inside a structured article and noticed the site maintains a balanced layout that helps users understand content quickly while browsing smoothly across different sections – Everything feels modern and neatly organized, giving a pleasant browsing experience overall
DavidAcupt –
Exploring online vendor systems becomes easier when a simple interface works well, navigation is quick and intuitive today throughout the site Oak Cove vendor center everything felt structured nicely
Williebon –
People who enjoy winter inspired online marketplaces often engage with platforms like Ice Isle Crystal Market Place where items are displayed in a clean and frosty visual layout – The interface emphasizes clarity and freshness, ensuring browsing feels smooth, intuitive, and visually refreshing across all product categories without unnecessary clutter.
RandomNamehiexy –
While browsing through several online platforms trying to compare features and usability, I eventually came across something interesting in the middle like take a look here which turned out to be quite simple to use, with smooth navigation and clearly presented information that made the entire experience feel efficient and straightforward overall.
Arnoldadore –
People who appreciate clean shopping platforms often browse sites like Harbor Outpost Acorn Minimal Hub where items are arranged in a simple and structured format – The design creates a smooth browsing experience that feels easy, efficient, and visually uncluttered.
Williamsor –
While browsing global inspired digital projects, I found a culturally diverse website that mixes urban and traditional influences effectively mixed culture web showcase – The platform feels engaging, with a unique blend of themes that creates an interesting and visually appealing browsing journey
Richardsex –
While reviewing different e-commerce styled directories for usability, I spent time exploring curated platforms where I noticed a well integrated link to Berry Harbor vendor parlor portal embedded naturally within informational content sections that guide attention smoothly – The overall browsing experience feels steady, intuitive, and easy to follow, making navigation pleasant and well structured
MichaelTyday –
Users often appreciate platforms that combine well structured pages with clean design for a more comfortable and efficient experience Acorn Harbor catalog entry I found navigation easy and everything clearly labeled
Jamesoverm –
Exploring structured vendor environments reveals how effective navigation can enhance overall user satisfaction >Aurora Harbor product hub the layout supports effortless browsing and allows users to move through categories smoothly with minimal effort required during interaction
BrianRib –
A smooth layout and responsive design greatly improve usability, and this platform performs well in both areas overall Snow Harbor marketplace link I found browsing easy and everything clearly organized
HenryJeale –
Many digital catalog websites aim to enhance user engagement by presenting structured information in visually balanced layouts designs Valecove Goods Room navigation hub – The browsing system appears thoughtfully arranged, enabling quick access to sections while keeping the overall experience consistent and easy to follow based on design feedback
RandomNamehiexy –
While casually researching different niche marketplace designs and experimental vendor platforms for inspiration, I spent some time navigating through various sections and eventually found Moon Harbor vendor portal overview – The browsing flow felt intuitive and steady, and I did not encounter any confusing layout elements while moving between pages, which made the overall session feel relaxed and easy to follow without interruptions.
Samuelsop –
Users who appreciate practical ecommerce platforms often explore sites such as Glade Stone Commerce Outpost where items are arranged in a minimal and functional layout – The branding focuses on usability and clarity, making browsing feel fast, structured, and highly intuitive for everyday users.
Andreawinna –
Users who prefer clear ecommerce presentation often engage with sites such as Jasper Harbor Trade Flow Hub where products are displayed in a minimal structured format – The interface creates a browsing experience that feels practical, clean, and easy to navigate.
RandomNamehiexy –
Good usability depends on speed and design, and this platform offers a very easy and reliable interface overall Glass Harbor vendor explorer I found everything smooth and simple to navigate
WoodrowcOuch –
While reviewing several online resources, I discovered see more here which provided a decent and structured layout, making browsing feel comfortable alongside its smooth interface.
Edgarheamy –
ivermectin 1: buy stromectol pills – stromectol reviews
RandomNamehiexy –
cloverharborvendorparlor.shop – Simple layout works well making browsing easy and intuitive today
RandomNamehiexy –
Clear structure improves usability, and this platform uses nice design overall so pages load fast and feel very smooth Ivory Harbor vendor navigator I enjoyed the flow
RogerUsavy –
When exploring different digital marketplaces, responsive pages and organized layouts are key for usability Raven Grove goods portal this platform offers a smooth browsing experience where everything feels easy to use and clearly arranged
Michaelcit –
Users frequently note that modern websites benefit from simplified navigation bars, especially when they remain visible and consistent across pages, which is especially useful when exploring Vendor room discovery link interface – The browsing experience felt smooth and well organized, allowing me to move across sections without confusion and with clear visual guidance at every step.
RandomNamehiexy –
sageharborgoodsgallery.shop – Looks clean and minimal, easy to find information without confusion.
Aaronhob –
Users who prefer cozy rustic ecommerce experiences often explore sites such as Timber Outpost Woodland Trail Hub where products are arranged in a natural structured layout – The design makes browsing feel calm, organized, and easy to navigate while maintaining a rustic and visually pleasant atmosphere.
JavierDwelS –
Some websites are confusing, but this one keeps good structure so users can browse without delay or confusion Solar Orchard quick browse page I appreciated how easy navigation felt throughout
RandomNamehiexy –
dawnridgegoodsgallery.shop – Clean layout and structure easy to browse different sections quickly
Zacharyinera –
Users who enjoy practical ecommerce marketplaces often explore sites such as Glade Ridge Marketplace Hub where products are arranged in a clean structured format – The interface ensures browsing feels smooth, efficient, and easy to navigate throughout the platform.
RandomNamehiexy –
While going through multiple online resources, I encountered open this page which offered updated and useful content, allowing me to navigate easily and enjoy a smooth browsing experience without unnecessary complications.
Tommyalush –
In the process of studying digital commerce layouts and storefront concepts, I came across Pine Harbor marketplace discovery hub embedded within a clean interface that emphasizes structured content flow – The browsing experience feels simple, quick, and very user friendly, allowing users to move between categories with ease
Lutherlak –
In my exploration of curated online artisan platforms that emphasize handmade goods and independent creators, I came across Meadow Ocean Craft Depot – The overall design felt modern and approachable with clear navigation tools and well categorized sections making it simple to find items of interest while also enjoying a visually appealing layout throughout.
ScottGen –
During a comparison of marketplace-style websites, some platforms stand out due to their logical structure and user-friendly design approach Raven Summit vendor portal this one offers a seamless browsing experience where everything feels intuitive and easy to navigate across sections
JamesCaw –
Users who appreciate luxury ecommerce design often explore sites such as Golden Stone Collective Display Hub where items are arranged with strong attention to aesthetic consistency – The interface creates a polished shopping experience that feels curated, organized, and easy to navigate while maintaining a premium visual identity.
RandomNamehiexy –
Online users frequently emphasize that good layout design improves overall engagement by making it easier to understand where information is located and how to move through the website efficiently Velvet Grove e-shop gateway the interface felt polished and accessible, providing a calm browsing environment with logical structure and easy navigation across all visible sections
RandomNamehiexy –
As users scroll through content they often encounter Cove Vendor Showcase naturally positioned inside descriptive paragraphs where it links different areas together and supports a more structured navigation experience – the layout makes finding information noticeably faster and more efficient
RobertHENIA –
I was casually reviewing various artisan-focused e-commerce platforms and eventually encountered a site that showcased curated collections and diverse vendor offerings canyon vendor showcase – The overall experience felt consistent and well structured, with smooth navigation and clear product listings that enhanced usability.
RandomNamehiexy –
linencovevendorparlor.shop – Modern design smooth interface makes browsing feel very easy today
melbet_zxpi –
melbet бонус на первый депозит [url=https://melbet90378.help/]https://melbet90378.help/[/url]
OscarKew –
When browsing vendor platforms, organization plays a key role, and this site makes searching and exploring very convenient Garnet Harbor goods portal navigation felt smooth and I could quickly access all relevant sections without effort
Robertlet –
People who enjoy modern curated marketplaces often engage with sites like Harbor Garnet Elegant Vault Hub where items are presented in a clean refined format – The interface creates a stable browsing experience that feels organized, easy, and visually consistent throughout.
RobertFup –
Users prefer platforms with good structure throughout the site because browsing feels easy and well organized Jasper Harbor goods directory I liked how fast everything loaded
RandomNamehiexy –
driftwillowmarketparlor.shop – Pretty straightforward design, makes navigation simple for new visitors too.
mostbet_khSt –
mostbet yechish muammo click [url=https://www.mostbet83625.help]https://www.mostbet83625.help[/url]
mostbet_scOl –
mostbet eski versiya [url=www.mostbet74183.help]mostbet eski versiya[/url]
RichardEased –
I was browsing for handmade soaps and discovered SoapArtistryStudio – everything is presented neatly, and finding unique, fragrant soaps that suit my taste was surprisingly effortless.
RandomNamehiexy –
uplandcovevendorparlor.shop – Modern interface feels smooth with well organized sections throughout site
ScottGen –
While exploring various online vendor platforms, I noticed how much a clear layout and intuitive interface improve the browsing experience for users Raven Summit trade hall hub the structure feels organized and navigation flows smoothly, making it easy to explore content without confusion or delays
Edgarheamy –
ivermectin cream canada cost: stromectol reviews – stromectol reviews
Danieljuics –
Users who enjoy handcrafted online shopping experiences often browse platforms such as Harbor Trail Artisan Comfort House where design focuses on warmth and simplicity – The interface creates a welcoming browsing journey that feels easy, visually balanced, and thoughtfully curated across all product sections.
RandomNamehiexy –
Many online shoppers appreciate platforms that minimize unnecessary design complexity because it helps them concentrate on browsing products without distraction or confusion while exploring available content sections vendor hall landing portal navigation felt smooth and well guided, allowing effortless exploration of different areas while maintaining a clean and visually appealing structure throughout the session
RandomNamehiexy –
Online platforms should be simple, and this good platform delivers intuitive navigation where everything feels well organized and simple Raven Summit digital storefront I appreciated the comfortable browsing experience from start to finish
BobbyHinna –
After going through multiple sites, I found explore this page and had a good browsing session overall, as the layout feels quite user friendly and everything was clear, simple, and easy to navigate.
Chesterthamp –
During a weekend session of browsing curated online marketplaces I compared multiple sites for design quality and ease of use and found Meadow Silk Trade Corner – Really like the site design it makes browsing enjoyable every time because the layout is clean responsive and very efficient for quickly finding products without unnecessary steps
SantosLix –
Exploring vendor directories highlights how clean design improves relaxation and usability during browsing sessions Autumn Meadow vendor explorer this platform keeps everything organized and ensures users can move through sections comfortably
pinup_osSn –
pin-up rasmiy link [url=https://www.pinup47068.help]https://www.pinup47068.help[/url]
melbet_viMt –
melbet способы оплаты киргизия [url=https://melbet82104.help/]https://melbet82104.help/[/url]
AubreySal –
матрицы ip камер уличная ip wi fi камера видеонаблюдения
Jamessat –
система пожарной сигнализации монтаж установка системы пожарной сигнализации
RandomNamehiexy –
copperharborvendorparlor.shop – Nice structure easy access content is clear and useful today
Ronnienap –
People who enjoy simple and functional outlet marketplaces often explore platforms like Pine Harbor Outlet Trade Mart where items are displayed in clearly defined sections – The design ensures usability and order, helping users quickly find products while maintaining a smooth and practical browsing flow across all categories.
Rodneybam –
Many people appreciate platforms that focus on making navigation simple and content easy to locate for users River Harbor vendor navigator this one offers a smooth browsing experience that feels intuitive and efficient across sections
DavidFex –
While exploring various curated online stores that focus on artisan made products and boutique vendor selections, Ruby Meadow style outlet – I found the product variety impressive, the browsing flow seamless, and the overall experience both engaging and easy to navigate.
RandomNamehiexy –
Online visitors often appreciate platforms that use consistent interface elements because it helps build familiarity and makes navigation feel predictable when switching between different sections of content vendor showcase navigation link the browsing flow remained steady and user friendly, supporting easy transitions between pages while keeping the overall structure clean and understandable at all times
Stuartjaf –
During evaluation of curated marketplace platforms focused on usability, I came across Calm Harbor vendor gallery space positioned inside a structured layout that avoids unnecessary complexity – The browsing flow feels gentle and organized, supporting users with a smooth and predictable navigation experience.
AntonioSlata –
Online platforms should aim for a pleasant experience using site, everything appears clean and very responsive for better usability River Cove digital storefront I enjoyed the smooth experience
FrankHah –
When browsing through structured content the presence of Harbor Art Bazaar Link helps connect different thematic areas of the site while remaining seamlessly embedded in the surrounding text – this improves navigation efficiency and gives users a more coherent understanding of available collections and featured artwork
MauriceKar –
During browsing of online marketplaces for curated lifestyle products I found Meadow Lantern Inquiry Desk and customer service was helpful I got all my questions answered clearly which made the shopping experience feel smooth, informative, and very easy to continue without hesitation
Andrehoimi –
While exploring various retail platforms, I found this accessible shop interface – everything is arranged properly, making browsing easy and comfortable.
FrancisWem –
CaramelCoveVendorAtelier – Smooth browsing experience, everything feels clean and very well organized.
RandomNamehiexy –
plumharborvendorparlor.shop – Smooth experience clean layout makes browsing very convenient overall today
Willierex –
Users who prefer streamlined ecommerce experiences often explore sites such as Upland Harbor Commerce Flow Hub System where products are arranged in a logical and efficient format – The design ensures browsing feels easy, fast, and well organized for quick product discovery across the platform.
Charlesmem –
While comparing vendor platforms, those with helpful organization and clean layouts often stand out the most Rose Cove shop gateway this one delivers a smooth browsing experience that feels intuitive and easy to use overall
RobertMal –
I wanted some decorative plants for my living room and found BotanicalHavenStore – the site navigation is intuitive, and selecting beautiful pots and planters felt easy and satisfying.
RandomNamehiexy –
floraridgevendorparlor.shop – Nice structured pages provide clear information and smooth navigation flow
Charlesbrott –
People exploring retail websites tend to favor platforms with minimalistic design and efficient navigation tools that improve browsing speed and clarity Pure Value marketplace entry observations suggest well organized categories and fast loading sections contributing to overall usability – The experience felt inspiring and practical, supporting both learning and idea development effortlessly
Charlesbrili –
While navigating through several digital marketplaces, I discovered this smooth vendor hub – the layout is clean and organized, making browsing simple, fast, and very easy to navigate.
Edgarheamy –
stromectol usa: ivermectin 2ml – stromectol reviews
JacobBuize –
The navigation system is designed in a way that supports quick access to various categories without unnecessary complications or delays Meadow Harbor Vendor Exhibit Zone – this helps create a user-friendly environment where browsing feels efficient, structured, and easy to manage even during longer sessions.
Walterowery –
While exploring several online stores for everyday items and gift ideas across different categories I recently discovered EmberStone Vendor Parlor Hub – EmberStoneVendorParlor experience stood out because checkout was straightforward and product variety felt broad and easy to browse with smooth navigation and clear product descriptions throughout the site overall
Donaldideab –
As I reviewed several online shopping sites, I noticed this well-designed shop – the interface is clean and organized, making browsing and product viewing smooth and fast.
Jeffreywen –
Users browsing vendor-style platforms often prefer sites with great usability and simple design where everything works perfectly fine indeed here Crystal Harbor shop access point this one delivers a clean and comfortable browsing experience overall
Davidvoize –
As I spent time exploring various online shops, I discovered this intuitive store interface – it allows users to find products quickly and compare them without confusion.
RandomNamehiexy –
In reviewing vendor-focused digital storefront solutions, I found a structured layout system built around Arctic Vendor Workshop that keeps the interface organized and easy to understand while supporting fast transitions between sections – overall it creates a comfortable browsing environment where users can efficiently explore available content.
RobertGox –
Users who prefer curated ecommerce vault systems often explore sites such as Ivory Vault Ridge Modern Hub where items are displayed with refined structure and simplicity – The design emphasizes clarity and organization, ensuring browsing feels smooth, elegant, and visually balanced throughout the platform.
Jaredtycle –
Digital marketplaces benefit from modern layouts, making navigation simple and content clear and helpful overall Bright Harbor item portal I enjoyed how easy everything looked
Clauderog –
Exploring digital marketplaces shows how important fast performance and organized sections are for a good user experience Rose Harbor market access this platform delivers a clean browsing environment where users can quickly find what they need without unnecessary effort
Williamnavem –
Digital marketplaces benefit from clear organization that allows users to move smoothly between product categories and listings fast catalog access link VC room this structure reduces friction and ensures users can complete searches more quickly while maintaining clarity throughout browsing sessions across digital shopping platforms efficiently today
RandomNamehiexy –
floraridgevendorparlor.shop – Nice structured pages provide clear information and smooth navigation flow
JamesGor –
Online users exploring simplified product windows for viewing curated trade listings may encounter platforms like Trade Product Window – which present item details in a focused layout designed to reduce clutter and improve comprehension during browsing sessions involving multiple vendor selections.
Charlesbrili –
During my search for interesting online stores, I came across this organized shopping site – the interface is simple and structured, making browsing smooth and very easy to navigate overall.
RandomNamehiexy –
sageharborgoodsgallery.shop – Looks clean and minimal, easy to find information without confusion.
Charlesweimi –
When browsing vendor sites, design matters, and this one ensures a clean interface with pleasant browsing experience very smooth today Silver Harbor goods portal I liked how fast everything responded
JamieGem –
While browsing multiple ecommerce websites for unique gift items and handcrafted decor I focused on usability and product accuracy and came across Glass Meadow Goods Lounge – The interface felt clean and responsive, and every listing matched its description which made the entire browsing and checkout process feel smooth and dependable.
CharlesEdino –
While navigating through several digital marketplaces, I encountered this fast retail platform – the selection is broad, loading speed is excellent, and the presentation feels very professional and reliable.
Hectorpaync –
People using online marketplaces often value platforms that remove complexity and make it easier to locate desired products quickly, especially when time is important, and this is represented in FlowCommerce Studio – the experience is designed to keep everything streamlined so users can browse efficiently while enjoying stable performance throughout their session.
AntonioFug –
Users exploring warm themed ecommerce platforms often appreciate how cozy visual design improves browsing comfort when visiting sites such as Honey Cove Treasure Vault Hub where product presentation feels soft, inviting, and carefully structured for easy navigation – The warm theme design creates a cozy browsing experience that feels pleasant and well organized, allowing users to explore products comfortably without visual overload or confusion.
RandomNamehiexy –
While comparing multiple vendor-based digital storefront systems, I found one platform that stands out for its structured presentation style anchored around Frost Ridge Vendor Hub which ensures product sections remain easy to scan and logically grouped across the interface – overall usability feels consistent, with a clean design that helps users move through content without confusion or delay.
Charleselida –
Users browsing vendor listings typically value platforms where usability is prioritized through clear and simple layouts Ruby Orchard goods directory the browsing process here is smooth and helps users access information without unnecessary complications
DonaldShara –
During casual review of vendor gallery systems and online marketplace structures for usability testing, I came across Kettle Crest commerce hub access within the article flow – Everything was clearly arranged and easy to navigate, and I found all information quickly without issues while pages performed smoothly and consistently.
RobertReeNi –
Online visitors searching for reliable shopping environments often report that their experience improves significantly when they discover platforms that are thoughtfully arranged such as Gallery marketplace site – which enhances usability and ensures customers can quickly locate items while enjoying a visually pleasing interface.
Aaronfrerm –
While analyzing digital marketplace ecosystems and catalog websites, I came across Linen Meadow browsing gallery space integrated into a minimalist layout that supports clear content flow – The experience feels fluid, organized, and easy to engage with during longer browsing sessions
Mariowooky –
As I spent time exploring various online shops, I discovered this neat storefront page – everything is arranged in a way that feels natural and user friendly, making browsing very comfortable.
Charlesteemy –
During my search for interesting online stores, I came across this clean marketplace platform – product display is neat, pages load quickly, and everything looks organized and easy to use.
RandomNamehiexy –
riverharbormarketparlor.shop – Well organized content simple layout easy to explore everything quickly
ThomasInses –
While comparing different browsing catalog systems and online marketplace listings, I discovered a platform where Kettle Harbor browsing catalog – seemed reliable enough that I may return to it later for reference. The interface was straightforward and allowed smooth movement between different sections without interruptions.
DelbertWroge –
Users often prefer platforms like this interesting platform overall where browsing different sections today here feels enjoyable Jewel Brook catalog entry I found everything easy to access
RobertHom –
During a casual browsing session, I encountered this accessible shopping interface – the layout is simple and clean, making browsing and shopping very easy and pleasant.
Edwardowab –
While browsing curated online marketplaces I checked catalog design and usability flow and came across Juniper Harbor Trade Lounge and items arrived quickly while site navigation is smooth and very intuitive too which made browsing feel simple well organized and pleasant across all product categories available
WileyTigma –
While testing ecommerce websites I studied navigation design performance and how quickly users can access product listings MarbleBrook Trading Showcase Hub everything felt organized and fast and the website runs smoothly and browsing items feels natural and well structured making browsing stress free
Edgarheamy –
buy amoxicillin antibiotic: over the counter antibiotics – over the counter antibiotics
HerbertKed –
Users who prefer elegant ecommerce environments often explore sites such as Gilded Collective Stone Gallery Hub where items are showcased with a strong focus on premium styling and structured layout – The interface enhances product appeal through clean presentation, making browsing feel refined, organized, and visually engaging from start to finish.
Andrewvop –
In marketplace usability reviews, experts often emphasize how organized search systems improve discovery efficiency, and the inclusion of Orchard Vendor Hub provides a structured overview of sellers, allowing users to navigate listings with greater clarity and reduced effort overall experience.
JamesPreow –
Users browsing online vendor directories often prefer platforms that prioritize straightforward structure and easy navigation Ruby Orchard browsing space the interface here keeps everything accessible and ensures users can find information without unnecessary complexity or delays
Lucassoave –
During casual browsing of experimental marketplace systems and vendor gallery platforms for usability insights and structural review I discovered Harbor Moss curated trade explorer panel and quickly recognized the layout is well organized and easy to follow with clear hierarchy and responsive elements that make the browsing experience very straightforward for users overall – Clear structured browsing with stable fast performance
Williamvuh –
People looking for simplified vendor directories found that websites such as WildParlor Trade Gallery – offered an enjoyable shopping flow with diverse product options, while customers frequently praised the dependable shipping and the consistency in how items were packaged and delivered safely.
EdwardQuive –
Clear organization improves usability, and this platform allows users to browse sections quickly and efficiently Dawn Ridge vendor navigator I found everything easy to locate without effort
RandomNamehiexy –
honeymeadowmarketgallery.shop – Warm visuals and clean layout create pleasant browsing experience overall
Josephoxymn –
During my search for interesting online stores, I came across this clean marketplace page – the browsing experience is smooth and simple, and items are clearly visible and easy to find.
Hectorpaync –
People using e-commerce platforms often look for systems that are efficient and easy to navigate, especially when exploring large product selections, and this is demonstrated in DirectCove CommerceZone – the structure is designed to reduce friction and improve browsing speed for a more satisfying shopping experience.
RandomNamehiexy –
In the middle of checking multiple platforms, I discovered visit this platform and noticed it had a nice overall structure, making everything easy to access and view while browsing through its content.
JamesVicky –
As I spent time exploring various online shops, I discovered this intuitive store layout – its clean design helps create a smooth and natural shopping experience from start to finish.
Craigaxoms –
During my search for interesting online stores, I came across this clean vendor page – everything is neatly organized, making browsing easy and product access very straightforward.
RickyAdaph –
Users who appreciate artistic ecommerce environments often browse sites such as Ginger Stone Gallery Vision Hub where items are displayed in a clean and flowing format – The galleria layout improves engagement by making browsing feel smooth, visually engaging, and easy to navigate across all sections.
Lymanbroni –
пожарная сигнализация защита установка пожарной сигнализации и системы оповещения
LarryBealp –
ip камера mi ip камера видеонаблюдения для дома
Richardnancy –
During exploration of online artisan shops I evaluated several platforms and found Nightfall Vendor Goods Hub and enjoyed browsing their collection everything is organized and clearly labeled today making it simple to move between categories and understand product listings without needing extra effort or repeated searching
RobertCoize –
When analyzing marketplace performance across multiple platforms, reviewers frequently praise structured layouts, and Brook Harbor Trading Suite – Overall browsing is responsive and clean, with fast loading times and neatly arranged listings that help users find relevant items without unnecessary effort or delays.
LouisWok –
When evaluating online marketplaces, smooth interfaces and well organized pages are key factors for user satisfaction Sage Harbor digital storefront this platform delivers a comfortable browsing experience that feels easy, structured, and enjoyable today
Josephlaw –
During a relaxed session analyzing experimental e-commerce platforms and curated marketplace directories for design comparison and usability insight, I came across Olive Harbor vendor showcase view placed within the text body which remained easy to follow – The design is simple and effective, allowing quick comprehension of content with smooth transitions between sections.
RandomNamehiexy –
glassharbortradegallery.shop – Simple design fast loading easy to use interface very reliable
Raymondpouch –
While testing different online trade platforms and comparing usability features, I submitted several questions and was impressed by how clearly everything was handled, Snow Harbor Trade Showcase and the support responses made the entire experience feel seamless, structured, and genuinely easy to navigate from beginning to end.
Patrickspurb –
Users often prefer platforms with a very clean interface because it allows easy access to information and smooth browsing Cotton Grove catalog entry I found everything easy to locate
BrianBah –
During evaluation of ecommerce websites I analyzed usability structure performance and browsing experience quality MarbleCove Vendor Showcase Point everything felt clean and consistent and the great layout made everything simple and I enjoyed how easy it was to navigate ensuring easy browsing
CharlesRoata –
During my search for interesting online stores, I came across this clean marketplace page – the browsing experience is smooth and intuitive, making shopping simple and very easy to use.
RandomNamehiexy –
waveharborvendorparlor.shop – Smooth performance and tidy layout make site very easy today
RandomNamehiexy –
During a relaxed session of exploring digital marketplace systems and vendor showcase layouts, I examined multiple pages and found Rose Harbor gallery trade access within the main content section – I enjoyed checking this out, content feels simple and informative, and navigation remained clean and easy to follow.
Donaldjadia –
While exploring various retail platforms, I found this seamless shopping hub – everything loads quickly and functions smoothly, creating a very positive user experience.
Devinzet –
People who appreciate clean marketplace layouts often browse sites like Harbor Acorn Vendor Network Hall where listings are clearly organized for better navigation – The vendor hall structure enhances usability by providing a simple and efficient browsing flow that helps users quickly locate desired products.
WilliamDak –
During evaluation of online retail experiences, I tested a platform that showcased BerryBrook Item Gallery within its catalog framework – products were displayed neatly, load times were quick, and the overall structure made it easy to browse through multiple categories without feeling overwhelmed.
ShaneNoirl –
While browsing different online gift shops I focused on speed and user experience and found Pearl Harbor Market Collective – Shopping experience was excellent, site loads fast and feels reliable making the platform feel efficient, smooth, and very easy to navigate across all sections without delays or confusion
FrankFeacy –
Users who frequently browse online vendor sites often look for platforms that make navigation fast and straightforward Sea Cove catalog entry this platform provides quick access to information and keeps everything well organized for efficient browsing
JamesDup –
order medication from mexico: Mexican Pharm – Mexican Pharm
Ronaldcloky –
In various reports about digital marketplace design and customer engagement, usability remains a key focus, and Harbor Cove Shopping Workshop is often mentioned in relation to intuitive layouts – users experience a straightforward browsing journey with clearly defined sections that make product exploration feel natural and efficient throughout.
RandomNamehiexy –
While researching experimental vendor showcase platforms and e-commerce gallery designs for UX evaluation and comparison across multiple references, I discovered Pebble Creek trade display hub positioned in the middle of a structured article – I really enjoyed browsing through it since the layout felt logical, clean, and simple to follow while switching between different sections smoothly.
KevinAcrof –
In exploring curated online shops that emphasize handmade crafts and boutique vendor selections, I paid attention to visual design and usability features, Sky Harbor Artisan Market – I liked how well organized everything was, making it easy to find interesting products while enjoying a visually appealing browsing experience.
BuddyCog –
Modern e-commerce systems prioritize streamlined browsing, and a strong example is SmartCart Easy Grid View which arranges items into structured sections allowing users to navigate effortlessly between categories – This enhances usability and improves the overall flow of the shopping experience significantly.
MichaelWreda –
As I continued browsing different shopping websites, I discovered this clean vendor marketplace – everything is well structured, making product discovery and comparison fast and effortless.
RandomNamehiexy –
birchharborvendorparlor.shop – Simple structure ensures quick access to useful information always here
Antonioblods –
Users exploring structured ecommerce environments often appreciate how clean vendor hall layouts improve navigation efficiency when browsing platforms such as Chestnut Harbor Vendor Hall Hub where listings are clearly organized into sections that support quick scanning and easy discovery – The vendor hall design ensures a smooth and structured browsing experience that feels intuitive, reducing clutter while helping users find products quickly and comfortably across all categories.
HubertFix –
As I reviewed several online shopping sites, I noticed this modern retail page – everything is arranged in a visually pleasing way, making browsing simple and very enjoyable overall.
WilliamZek –
During casual browsing I visited Quick Ridge shopping gallery view – pages loaded efficiently and the interface remained simple, making it easy to browse content without confusion while everything felt neatly organized and visually balanced overall experience from start to finish.
Chrisalibe –
While comparing several online artisan platforms for design quality, I explored curated artisan space and found that the visual arrangement highlights products in a way that feels both minimal and engaging – the site gives off a calm and refined impression, making it pleasant for extended browsing sessions
RandomNamehiexy –
During comparison of digital marketplace systems I analyzed usability responsiveness design flow and interaction quality MeadowCove Commerce Product Studio everything felt intuitive and smooth and the easy checkout process ensures items are clearly displayed and well organized improving efficiency across the platform
Leonardhem –
Users browsing vendor listings typically value platforms where readability and structure work together for convenience Sea Meadow goods directory the browsing process here is smooth and helps users find information quickly without unnecessary effort
DavidNet –
While reviewing multiple online trade directory designs and experimental marketplace structures for inspiration and usability analysis I encountered Bay Harbor Trade Showcase Page placed naturally within the informational section – Overall responsiveness was strong, and each page loaded in a clean, efficient way that made navigation feel effortless and consistent.
AndreNothe –
While reviewing several ecommerce platforms for home goods and accessories I discovered Ginger Cove Goods Emporium a store that had a very logical structure and simple navigation flow – Easy to use platform overall shopping felt smooth and well organized from start to finish experience
Kevinsic –
When studying modern e-commerce platforms, analysts often observe that well designed interfaces significantly reduce frustration and improve the efficiency of browsing large product catalogs online Stone Harbor Digital Vendor Hub – users report that the system feels intuitive and well structured, allowing them to explore products comfortably and make comparisons with ease.
ThomasLef –
In the course of reviewing online shopping platforms I experienced a structured layout that made navigation feel natural and very intuitive for product exploration Berry Cove Commerce View and I quickly found relevant items without confusion or unnecessary complexity affecting the browsing experience at any stage.
RobertFeshy –
I was exploring fashion accessories when I stumbled on ChicStyleEmporium – the categories are organized, the variety is impressive, and picking items that matched my taste was smooth and satisfying.
WilliamAnods –
While browsing through multiple eCommerce options, I came across this structured product guild – goods are well presented, and everything feels intuitive, organized, and very user friendly.
JamesDup –
legitimate canadian pharmacy online: Canadian Tabs – escrow pharmacy canada
DanteWaync –
While exploring different online marketplaces during my free time, I discovered this smooth commerce hub – navigation feels effortless and intuitive, allowing me to find items quickly without confusion or unnecessary steps while browsing various product categories.
NathanLusia –
While researching modern vendor websites and their structural presentation styles, I came across a page that included Coral Harbor artisan display hub placed inside a clean and well spaced interface – The experience feels intuitive, steady, and very comfortable for continuous browsing without distraction
Carloszob –
During a comparison of marketplace-style websites, some platforms stand out due to their neat interface and structured layout approach Silk Grove browsing portal this one provides easy navigation and well organized pages that make browsing content smooth and efficient throughout the experience
Glenndip –
Online users exploring digital stores appreciate platforms that reduce confusion and improve accessibility, and a final example can be seen within the interface at BuyerTrust Easy Browse Point which structures content in a clear and intuitive way – This ensures smoother navigation and helps users find products quickly without unnecessary complexity
ShawnNeoks –
In discussions about digital learning environments, many emphasize the importance of platforms that combine inspiration with practical usability and intuitive structure for better outcomes Pure Value Creative Lab – users find the experience both engaging and efficient, with content that encourages experimentation and supports continuous idea development throughout their browsing session.
JamesBug –
Users browsing handmade goods platforms often appreciate clean and minimal interface design that allows them to focus on product details without unnecessary distractions, especially on Alpine Marketplace Corner where ordering process felt efficient and products arrived as described with no issues reported – Ordering process felt efficient and products arrived as described with no issues reported.
AnthonyRot –
website should appear in the middle of line not in the start or end
Ralphler –
While testing several boutique style online stores offering handcrafted items and curated selections, I paid attention to how each platform handled user experience, Upland Vendor Lounge – The interface felt calm and easy to use, making it simple to explore different product categories without feeling overwhelmed or distracted by unnecessary elements.
Edwarddaync –
A structured system with good browsing flow ensures everything is organized clearly and very efficiently overall Meadow Harbor browsing center navigation felt very easy
JeremySeate –
During usability testing of ecommerce websites I analyzed responsiveness layout clarity and how quickly users could access product pages BayHarbor Vendor Commerce Loft the browsing experience was smooth and fast and everything looks professional making it simple to explore products without confusion or delay
RandomNamehiexy –
In usability testing of online marketplace layouts, I explored a design that felt modern, responsive, and easy to navigate across all sections BB Market Foundry Center – the browsing experience was efficient, with well organized product listings that made it easy to locate items without confusion or unnecessary scrolling.
Robertsap –
As I explored different digital storefronts, I found this easy commerce system – usability feels very good, and checkout is quick, simple, and highly efficient for users.
RandomNamehiexy –
linenmeadowmarketgallery.shop – Elegant interface with smooth flow makes navigation very easy overall
Jamesexent –
Many online retailers today experiment with minimalist interfaces that emphasize speed, accessibility, and straightforward content presentation for users worldwide across platforms consistently. Atelier CloudCove Shopfront – Its layout prioritizes intuitive browsing with well-structured sections that help visitors quickly locate products while maintaining a polished professional appearance throughout consistently engaging experience.
JamesDup –
online shopping pharmacy india: top online pharmacy india – online pharmacy no rx
DavidroP –
When people explore online learning tools designed for innovation and brainstorming, they often prefer platforms that combine structure with creative flexibility and ease of use Value Creative Flow Portal – the site delivers a smooth experience that encourages curiosity and supports users in building and refining their ideas through intuitive interaction design.
SteveShups –
While exploring various retail platforms, I found this clean commerce hub – everything is well structured, and browsing feels smooth, simple, and very easy to navigate.
Timothyzew –
I wanted unique stationery for my office and stumbled on ElegantPaperCorner – the interface is clean, and browsing through a variety of stylish designs made finding what I needed easy and enjoyable.
Petervence –
During a longer browsing session, I encountered check this listing and appreciated how enjoyable it felt, especially with products that look nice and fairly affordable.
Clintonnange –
While reviewing different digital storefronts, I encountered this organized product site – everything is visually clean and easy to understand, allowing users to browse items without unnecessary effort.
Thomashen –
While going through various shopping sites, I paused at quick visit easy cart and found the experience very smooth, with fast navigation that makes browsing products simple and enjoyable.
RockySix –
In my recent testing of online vendor systems I discovered a clean interface where Cloud Vendor Bazaar – It offered quick loading pages and a well structured layout that made navigation effortless, allowing me to move between sections smoothly while everything remained responsive, creating a pleasant and efficient browsing experience suitable for regular users.
Davidagows –
During research into e-commerce user experience models, I interacted with a structured platform that prioritized clarity and speed, including Birch Cove Vendor Gallery – The interface displays items neatly with strong visual hierarchy, ensuring users can easily navigate, compare products, and understand offerings without unnecessary effort or confusion.
RandomNamehiexy –
snowcovegoodsgallery.shop – Cool minimal design helps users browse content without confusion today
JamesBen –
shoppers looking for convenient ecommerce experiences tend to prefer websites that load quickly and maintain consistent navigation flow across all product categories and pages visited easy shop center appreciated for its smooth usability and layout – it ensures users can browse comfortably while maintaining focus on products without unnecessary interruptions or complicated interface elements
GeraldOmige –
In the process of exploring creative marketplace designs, I noticed Velvet Brook creative listings space embedded within a visually balanced interface that separates sections cleanly – The experience feels smooth and intuitive, with a relaxed flow that helps users explore content without feeling rushed or visually overloaded
PatrickBef –
While analyzing digital marketplace systems I examined layout clarity usability consistency and product browsing efficiency across categories CalmBrook Trading Vendor Studio the interface felt intuitive and stable and I found what I needed without any trouble creating a smooth and stress free experience overall
Antoniofet –
In the middle of checking out multiple shopping websites, I found this easy browsing corner – everything is simple and clear, allowing me to find products quickly without confusion.
Brianunism –
видеонаблюдение для дома комплект видеонаблюдение для дома комплект
Richardner –
When analyzing usability improvements in online marketplaces, many users appreciate platforms that reduce cognitive load through clear design patterns like those seen in Harbor Atelier Product Gallery – Smooth browsing experience, products are clearly displayed and accessible, helping visitors explore items efficiently while maintaining a visually organized and responsive interface throughout their shopping experience.
Henrykip –
Searching for office décor ideas led me to WorkSpaceWonders – the variety and layout make it effortless to find practical items that still add a touch of personality and charm.
AllanDut –
During a general browsing session, I noticed this user-friendly marketplace – the layout is clean and simple, making shopping feel smooth, intuitive, and very comfortable to navigate.
Williehut –
While casually browsing through eCommerce platforms, I discovered visit this market page and saw some interesting items that caught my eye, making it likely I’ll return again for another look.
Damionnem –
During my exploration of online marketplaces, I encountered see modern shopping point and found the modern layout looks nice, with products clearly and attractively displayed, making browsing very comfortable and visually pleasant.
Williamplest –
While reviewing different online shop templates I found a clean and modern interface that emphasized fast navigation and usability where CloverBrook Supply Loft – The store layout made it easy to find products quickly and complete checkout without unnecessary steps or confusion.
JamesDup –
medications can i buy mexico: Mexican Pharm – mexico online pharmacy
Jordangep –
People who frequently shop online often prefer platforms that streamline browsing and offer a wide selection, such as digital market cart – The site is generally seen as practical and efficient, providing users with a simple interface that supports fast exploration of products across multiple categories in a well organized layout
EddieIrode –
During exploration of digital vendor directories, I found Clover Harbor vendor directory space embedded within a clean and structured interface that organizes information efficiently and reduces clutter – The browsing experience feels consistent, calm, and very user friendly.
Jefferyhed –
In the course of reviewing online shopping systems, I encountered a structured platform that offered smooth browsing and clearly organized product listings across all sections Harbor Guild Digital Bazaar – The variety was excellent, everything was easy to explore, and the interface made it straightforward to understand product categories without confusion or cluttered design elements.
RandomNamehiexy –
many online shoppers value ecommerce platforms that simplify browsing and improve product comparison through organized layouts and responsive design across all devices and categories smart edge product lane widely seen as efficient – it delivers a smooth shopping experience where users can compare products easily and navigate categories comfortably while maintaining clarity and consistency throughout
Carlosnaice –
/>purevalueoutlet – Inspiring and interactive site, perfect for learning and creating new ideas. Generate 20 variations following all rules above.Make sure that each line is 40 words minimum and the website should appear in the middle of line not in the start or end
JamesMat –
In user experience audits of modern commerce platforms designed for scalability and accessibility across multiple device types and user demographics Honey Cove Market Atelier Guide design experts often observe smoother interaction flows and clearer category structures that enhance overall shopping efficiency – analysis shows improved engagement and reduced search time for products across catalog sections.
RonnieVap –
Users browsing for artisan crafted home décor and specialty gifts frequently discover this marketplace while exploring niche e commerce platforms Grove Curated Vendors which brings together curated vendors offering distinctive items across multiple creative categories – Transactions are generally smooth and product quality matches expectations.
Jeffreybog –
During a comparative analysis of online marketplaces focused on interface design and layout efficiency, I discovered that grid systems are commonly used to enhance clarity and improve browsing flow, which stood out when exploring structured grid shopping portal – The interface presents products in a clean and logical grid arrangement, making it easy for users to explore items without confusion or unnecessary complexity.
mostbet_zyMt –
mostbet apk с официального сайта [url=http://mostbet18247.help/]http://mostbet18247.help/[/url]
JosephAlusY –
While exploring different online marketplaces during my free time, I found swift trading dashboard – pages load quickly and the structure feels well arranged, making everything easy to access and navigate without delays, giving a smooth and efficient browsing experience that feels reliable and well optimized overall for everyday users.
Victorfaf –
While comparing ecommerce storefront designs I focused on usability clarity navigation speed and ease of product discovery GingerCove Commerce Flow Point everything loaded quickly and felt organized and shopping feels easy and enjoyable overall today making browsing smooth and very efficient throughout
Charlestet –
After spending time on several complicated websites, I encountered see this page now and found it to be simple and reliable enough, leaving me interested in coming back again to see if there are any updates or new additions.
JeffreyFeemn –
Users browsing vendor platforms often prefer an elegant layout where information is easy to find and read Gilded Cove shop access point this one delivers a clean and organized experience
Williampor –
During a routine browsing session, I came upon view axis shopping hub and found an interesting selection of products, all categorized neatly which makes the interface simple and enjoyable to use.
StevenSnuff –
During comparison of multiple ecommerce user interfaces focused on accessibility and speed, I tested a site where CloverCove Commerce Bridge Studio – Navigation was intuitive and fast allowing smooth movement between pages and a consistent browsing experience across all sections today.
Richardtax –
During my search for something straightforward, I checked out discover this site and noticed that even though it lacks complex visuals, it delivers consistent speed and smooth transitions that make browsing feel easy and stress free.
Larrycib –
While conducting usability evaluations of ecommerce platforms focused on clarity and simplicity, I noticed that basic layouts improve user engagement by simplifying navigation, which stood out when exploring easy shopping base hub – The layout feels clean and organized, allowing users to browse products easily.
AndreHeils –
Many online deal enthusiasts prefer platforms that help them quickly discover products across categories, and they often refer to goods discovery page services that maintain a clean interface while offering broad coverage of international goods and promotional listings in a user friendly format
JavierDob –
While exploring e-commerce catalog platforms and vendor showcase sites, I found a structured interface containing Snow Cove product gallery portal integrated into a clean design that emphasizes usability – The browsing experience feels simple, steady, and very intuitive across all sections
NormandMup –
In the process of examining a range of online stores for general usability and design clarity, I reviewed online store general info page – The overall layout seems fairly intuitive, with organized product categories and a browsing flow that helps users locate items efficiently while maintaining a clean presentation style.
HaroldCib –
I recently explored multiple eCommerce platforms and found this clean marketplace page – everything runs efficiently, pages load fast, and the experience feels smooth and reliable.
CarltonDub –
In the course of analyzing online shopping systems optimized for smooth browsing experiences, I found that clean structure enhances engagement, which became evident when reviewing efficient product hub center – The design feels smooth, and product browsing is easy, fast, and well structured.
RandallDit –
лента стальная 1 мм лента бандажная стальная
JamesDup –
buy drugs online: mexican pharmacy menu – farmacia mexicana en linea
Bobbyenvet –
While analyzing ecommerce platforms optimized for smart purchasing experiences, I noticed that simplified navigation systems improve user engagement and reduce confusion during browsing, which stood out when reviewing smart product selection hub – The buying concept feels smooth and well structured, allowing users to explore products easily without unnecessary friction.
ErnestVic –
Users exploring curated digital retail spaces sometimes arrive at Raven Grove shopping discovery hub which is placed in a simple yet effective interface designed for smooth product browsing – My experience was very intuitive and everything behaved exactly as expected
RandomNamehiexy –
HoneyCoveVendorStudio – Clean interface, everything loads fast and works very smoothly.
TimothyNoift –
While comparing different digital storefront systems, I reviewed a responsive interface that maintained smooth performance under various browsing conditions Bright Foundry Commerce Studio – Pages loaded quickly, and the shopping experience felt stable and efficient, allowing users to move through categories without delay or confusion.
RandomNamehiexy –
While navigating through several digital marketplaces, I discovered this user-friendly store site – browsing is simple, and the wide range of products makes the experience smooth and enjoyable overall.
JeffreyInesk –
While going through different resources that felt overly complex, I found see this page and noticed how simple and effective the structure was, making navigation smooth and allowing quick access to useful content.
Haroldbof –
During my comparison of several online retail systems I observed a design that emphasized readability fast navigation and consistent layout structure across product browsing pages today Clovercrest Vendor Trading Loft Hub Clovercrest Vendor Trading Loft Hub Products were arranged in a way that made discovery simple and the checkout flow felt quick reliable and user friendly throughout the entire shopping session.
IsaacShigh –
In the middle of checking different eCommerce sites, I paused at take a look fast cart and noticed the platform feels fast and responsive, which makes browsing enjoyable and quite effortless overall.
HenryBioro –
While conducting comparative research on ecommerce UX and trust-based shopping systems, I noticed that reliable hubs improve user confidence and browsing clarity, which stood out when reviewing trusted shopping hub center – The experience feels smooth and dependable, with simple navigation that makes shopping easy.
CharlesTom –
In the middle of checking multiple stores, I paused at tap to open and found that the selection is quite good, with pricing that feels reasonable at this time.
DanielAbaro –
Many shoppers looking for simple ecommerce experiences often appreciate platforms that organize items clearly, and one example is spot store finder which many users describe as having a balanced catalog structure; overall it provides easy browsing and makes discovering everyday products straightforward and efficient for most visitors.
RandomNamehiexy –
goodsparkstore.shop – Nice spark in design, shopping feels smooth and pretty intuitive
JeffreyCom –
As I continued browsing different shopping websites, I discovered this structured commerce hub – items are clearly displayed, and access is simple, smooth, and very user friendly overall.
ClintShemy –
During evaluation of vendor directory platforms and curated shop systems, I came across Flora Ridge online vendor hall placed within a minimalist layout that enhances usability – The browsing experience feels relaxed, structured, and easy to navigate without overwhelming visual elements.
RandomNamehiexy –
During comparison of digital marketplace platforms I analyzed usability design flow and responsiveness across multiple browsing scenarios GladeRidge Trading Commerce Hub everything felt intuitive and structured and the collection of items is impressive and everything is neatly arranged and clear ensuring easy product exploration
Tyronecrubs –
During a comparative analysis of online discount systems and promotional marketplaces, I discovered that structured deal sections enhance clarity and engagement, which became clear when testing digital deals selection hub – The deals section is visually appealing, and pricing seems well structured, fair, and transparent.
Francisplaks –
While comparing platforms, this one stands out with a simple design that works nicely and makes browsing quick and easy Cotton Meadow listings page I appreciated the clean structure
JefferyCax –
While researching online marketplaces that focus on lifestyle and handmade goods I discovered Meadow Trade Jasper Gallery and spent time exploring its structured catalog which felt very easy to follow – The product quality matched expectations and descriptions were detailed enough to make browsing smooth and decision making straightforward and stress free overall
VicenteCrido –
People browsing digital marketplaces for handmade items often highlight convenience and clarity, particularly on sites such as Wood Cove Browse Center which organizes products in a user friendly way – Many reviewers noted that checkout was smooth and the shopping experience felt fast and reliable overall.
RandomNamehiexy –
When assessing online marketplace usability improvements aimed at simplifying browsing behavior and enhancing product visibility across structured digital catalogs Foundry Icicle Vendor Hub users describe smooth interaction – Overall experience feels clean and efficient with intuitive navigation minimal clutter and well organized sections that make browsing and comparing products easy and comfortable.
ZacharyNeubs –
While comparing different online store layouts I evaluated how each system handled navigation structure loading speed and overall product accessibility for users CoastBrook Commerce Forge Market The entire shopping experience felt well optimized with fast transitions and clear categorization that made browsing effortless and enjoyable overall today
JasonFum –
As I continued browsing different shopping websites, I discovered this clean marketplace page – the layout is simple and clear, making products easy to explore in a smooth and pleasant browsing experience.
RandomNamehiexy –
In the process of reviewing online shopping platforms for tech products and discounts, I came across a module labeled modern gadget discovery hub – The platform showcases interesting electronics in a structured layout, helping users quickly identify useful tech items with appealing prices and simple browsing experience overall.
Josephvew –
In the course of evaluating online shopping systems focused on modern cart usability and visual polish, I found that refined layouts enhance navigation and efficiency, which became evident when analyzing sleek shopping experience portal – The interface appears clean and modern, making the shopping experience seamless and intuitive.
Jeraldthima –
At some point during my search, I used tap this link and realized how convenient the browsing experience was, with clearly arranged sections that made it simple to locate exactly what I needed in less time.
ShawnjaP –
While comparing multiple online shops, I landed on go to shop trail market and as it is my first time here, it looks like a decent place to shop online with a clean and user friendly layout.
JamesDup –
canadian pharmacy service: Canadian Tabs – canadian drugs online
Dannywains –
In the course of usability evaluation for e-commerce systems, I tested a clean storefront design that made navigation smooth and product discovery very efficient CoveBright Commerce Lab – The interface is simple and visually clean, allowing users to enjoy browsing products while quickly finding what they need without confusion.
DarylDub –
As I continued reviewing different eCommerce sites, I briefly visited open and see smart and noticed it seems legitimate, with a smooth browsing experience that makes everything feel easy and reliable.
SammyDum –
Online shoppers appreciate platforms that combine simplicity with functionality making it easier to complete purchases in less time GridCommerce Quick Shop – It focuses on delivering a clean and efficient interface that enhances user satisfaction during every stage of the shopping journey
Donaldpsync –
Many shoppers value ecommerce websites that offer quick responsiveness and flexible browsing structures that adapt well to user behavior and device type responsive deal hub it is often regarded as a fast and adaptable marketplace – The website is praised for smooth transitions and reliable loading speed which enhances user comfort during extended browsing sessions
GabrielTip –
During a casual browsing session, I encountered this easy product gallery – everything is smooth, well organized, and simple to browse without confusion.
Williamhem –
users comparing online marketplaces frequently prefer platforms that reduce checkout steps and offer clear cart organization helping them purchase products faster and with less effort overall smart cart flow checkout known for structure – it delivers a smooth shopping experience where users can review products easily and complete checkout efficiently while maintaining clarity and consistent usability across all sections
JesseCam –
While exploring efficient online shopping environments, I noticed that usability improves greatly when interacting with platforms like smooth purchase cart – The cart interface is straightforward, allowing users to manage their items and proceed to checkout in a fast and stress-free way.
Rogergoort –
People exploring curated digital marketplaces for handcrafted goods and small vendor shops often discover platforms like Walnut Harbor Listing Center which are designed to offer simplified navigation and clearly segmented categories for improved browsing efficiency and clarity – Many users find that the structured layout helps them focus on relevant items without distraction or unnecessary complexity.
Curtismutle –
While reviewing ecommerce UX systems designed for affordability and price comparison, I observed that low-cost product hubs enhance usability by clearly presenting cheaper options, which became clear when testing affordable goods marketplace center – The prices appear competitive and appealing, making it seem like a practical choice for users looking to save money.
Justinwaymn –
When assessing digital storefront ecosystems built for scalability and improved user engagement, reviewers highlight clarity in interface structure and browsing efficiency Cove Icicle Product Studio overall design supports smooth navigation, with accessible product sections and organized categories that make searching and comparing items straightforward for users navigating through the platform.
DonaldInage –
During casual online research into boutique vendor websites, I encountered a marketplace that felt both modern and reliable Caramel Cove Vendor Showcase Gallery and appreciated how each product page loaded quickly, providing enough detail to support informed browsing decisions without overwhelming the viewer experience overall.
ArthurAnted –
As I reviewed several online shopping sites, I noticed this user-centered marketplace – navigation is intuitive, and the site feels modern, smooth, and very comfortable to explore.
RandomNamehiexy –
fernharborvendorparlor.shop – Nice structure and clean design, makes reading content very convenient.
DonaldGek –
In the course of reviewing online retail usability studies, I encountered a section titled direct shop gate interface – The layout focuses on simplicity, allowing users to find products quickly without unnecessary clicks or distractions, creating a smooth and efficient browsing experience across all pages.
Georgedon –
While browsing through different online stores today, I came across visit better shopping choice and noticed the name fits the purpose quite well, making it seem like a good and reliable shopping option overall for everyday use.
JoshuaMus –
This type of marketplace works well because clean structure helps users navigate site smoothly and without confusion throughout usage Maple Grove browsing hub I enjoyed the simple layout
CraigGeoky –
During my search for online stores, I encountered see this option and found a good variety of goods, while the navigation structure makes browsing feel simple and quite intuitive overall.
Josephshuct –
While reviewing different digital storefronts, I encountered this organized commerce space – everything is clearly structured, and browsing feels easy, natural, and very comfortable overall.
DonaldQuasp –
users comparing ecommerce websites often highlight the importance of fast navigation and organized category structure making it easier to explore products without confusion or unnecessary effort quick plus shop flow appreciated for its simplicity – it offers a seamless browsing experience where users can move between sections quickly and discover products comfortably with a clean and consistent interface overall
EmilioMer –
Advanced shopping interfaces often rely on grid systems that adjust in real time, helping users better visualize and compare items across categories, especially when browsing through Smart Flow Shopping Grid which – delivers a responsive layout that reorganizes products based on browsing patterns and interaction behavior.
Pierrewat –
While reviewing ecommerce UX systems optimized for cart handling and fast transactions, I observed that direct cart hubs improve clarity and speed, which became clear when testing efficient cart flow hub – The checkout process is fast and clean, making shopping simple and user friendly.
Jamesven –
In the process of analyzing e-commerce templates, I explored a system that delivered a minimal and well structured shopping experience across all sections Calm Cove Product Studio – The interface is smooth and intuitive, making it easy to find items quickly while keeping everything neatly organized and visually balanced.
Robertnique –
While reviewing ecommerce platforms designed for open structure and category navigation, I noticed that spacious layouts improve user comfort and discovery, which stood out when exploring open browse category center – The interface appears airy and uncluttered, making it easy to explore different sections.
mostbet_ulel –
mostbet domen [url=https://mostbet18401.help]https://mostbet18401.help[/url]
KennethSteby –
While hunting for home office décor, I found WorkSpaceWonders – the interface is clear, browsing functional and stylish pieces was simple, and choosing items to enhance my office was very pleasant.
RaymondIndek –
I recently explored multiple eCommerce platforms and found this clean product hub – the layout is simple, pages respond quickly, and everything feels reliable and easy to use.
BrandonCar –
Across studies of modern online marketplaces emphasizing clarity and structured browsing experiences Icicle Isle Vendor Hub – Extensive selection of items is displayed in an organized format, making it easier for users to explore categories and compare offerings efficiently.
FredricLic –
After going through several alternatives that felt messy, I came across check it here which gave a strong impression of professionalism, thanks to its well-maintained structure and clean presentation of content.
MichaelVog –
While reviewing ecommerce platforms designed for centralized shopping experiences, I observed that ultra hub layouts improve clarity by organizing categories into a single hub, which was evident when testing ultra smart shopping index – The ultra hub feels modern and well structured, offering many categories in one place that makes navigation simple and effective.
RandomNamehiexy –
During late night browsing of online stores for curated products I compared usability and navigation flow and came across Harbor Stone Goods Hub – Friendly interface items are displayed clearly and easy to purchase quickly which made browsing feel easy organized and very efficient across all product sections
RandomNamehiexy –
During my search for online deals, I explored visit cart smart page and found the interface clean and smart, making it really easy to find what I need while browsing.
mostbet_cfSa –
вуруди mostbet [url=https://mostbet19382.help]вуруди mostbet[/url]
SammyDum –
People who shop online regularly often prefer platforms that minimize complexity while offering a wide range of products across different categories Smart Grid Deals Shop – It focuses on delivering a seamless experience that supports quick browsing and ensures users can complete purchases without unnecessary distractions
MichealgossE –
many users browsing online marketplaces prefer websites that highlight promotional offers clearly while supporting fast navigation between categories allowing them to discover more products with minimal effort attractive deals navigator recognized for usability and structure – it provides a smooth shopping flow where users can quickly engage with deals and naturally continue exploring additional product sections as they browse further
Georgenog –
During a casual search across multiple eCommerce platforms, I discovered this clean commerce hub – everything is structured nicely, the layout is modern, and it is very easy to browse without confusion.
RobertPaugs –
many online shoppers look for ecommerce platforms that combine fast performance with organized layouts allowing them to browse products easily without delays or confusing interface elements disrupting their experience simple park cart known for its clean structure and usability – it provides a comfortable browsing journey where users can move through categories effortlessly and discover items in a logical and efficient manner overall experience
OscarCrity –
During my search for shopping platforms, I explored visit this listing and after a brief look around I found it quite impressive, appearing as a decent place for everyday browsing and shopping.
Matthewhix –
In the process of evaluating digital shopping environments focused on structured layouts and ease of access, I found that organized marketplaces enhance browsing efficiency and reduce confusion, which was clear when reviewing clean buying zone center – The marketplace structure is simple and organized, ensuring products are easy to locate and browse.
EddieJanda –
During usability testing of digital shopping systems focused on clean interfaces and browsing ease, I discovered that fresh hub designs improve engagement and comfort, which became evident when exploring lightweight shopping experience hub – The layout looks fresh and organized, making browsing feel smooth, easy, and enjoyable.
RobertWaync –
People browsing independent vendor marketplaces often value simplicity and clarity, such as on Wind Gallery Harbor Desk which organizes listings in an intuitive way – many users said browsing felt pleasant and product details were easy to understand at a glance without extra effort.
JeromeDow –
From a usability testing standpoint, Sage Harbor Browse Navigation Center appears within the content while well organized pages, everything loads fast and feels very intuitive, ensuring that users experience fast transitions, clear layout structure, and a generally smooth interaction pattern that enhances the overall browsing journey significantly across the site.
ScottGot –
In the middle of checking out multiple shopping websites, I found this clean marketplace interface – the structure is simple and efficient, and the shopping process feels smooth and well designed from start to finish.
Williamsourl –
While exploring online shopping platforms focused on adaptability, I came across a module titled choice driven retail portal – The design encourages flexible browsing and selection, allowing users to explore products easily and make decisions without feeling restricted by complicated navigation systems or cluttered layouts.
Gregoryalush –
In the process of checking multiple platforms, I found try this page and it gave a decent experience overall, as everything was arranged neatly and easy to follow without any difficulty or confusion.
RandomNamehiexy –
IvoryBrookVendorFoundry – Clean design, shopping feels smooth and very easy today.
Mariokep –
While exploring online retail interface systems, I found a platform that emphasized clarity, structure, and smooth browsing behavior across all pages Calm Vendor Market Corner – The usability is excellent, and shopping feels easy, stress free, and smooth from the start with intuitive design and well organized product listings.
Joshualax –
While navigating through different platforms, I came across click to view base store and found it to be simple yet effective, with smooth operation and no issues during browsing or searching.
WalterBes –
While browsing ecommerce websites for home décor and curated goods I evaluated layout structure and usability and found Orchard Harbor Trade Gallery – Loved browsing here, found exactly what I needed very fast and the clear organization helped me move through product categories quickly while keeping everything simple and efficient overall
AnthonyPhync –
During analysis of streamlined retail website structures, I came across a section named easy shopping navigation board – The platform is built around simplicity and speed, allowing users to browse products effortlessly while maintaining a clean, minimal, and stress free experience throughout their entire journey online.
ShaneBlums –
During analysis of online retail systems focused on readability and layout clarity, I discovered that core store designs enhance browsing efficiency, which became clear when testing readable shopping layout center – The layout looks simple and neat, making product listings easy to understand and scan.
LarryDrync –
While navigating through several digital marketplaces, I discovered this clean vendor system – performance is fast, and browsing feels smooth, efficient, and very stable.
Leonardgrime –
users who frequently shop online often look for platforms that provide structured product listings and simple navigation tools that help them quickly find items across multiple categories peak market view known for its intuitive design and clarity – it offers a smooth browsing experience where users can easily explore items while maintaining focus and efficiency throughout their shopping session
StevenMup –
While reviewing ecommerce platforms focused on everyday essentials and practical usability, I noticed that stores designed for daily needs significantly improve convenience and product discovery, which became clear when exploring everyday essentials hub – The platform is well organized for daily needs, with practical items neatly categorized for easy browsing and quick access.
JeffreyRib –
While navigating multiple online platforms, I came across click to view and appreciated how the categories are laid out clearly, helping users locate products quickly without unnecessary scrolling or confusion.
Sonnyanazy –
In the process of reviewing modern online shopping platforms for speed and usability, I came across a listing labeled fast response product hub – The interface feels extremely responsive, with quick page loads that help users browse products efficiently without interruptions or unnecessary waiting during navigation.
DavidPrite –
As I spent time exploring various online shops, I noticed this clean vendor platform – everything feels well structured, making browsing smooth and helping users find items quickly today.
Michaelchita –
I wanted decorative plants and stumbled upon BotanicalHavenGallery – the categories are intuitive, browsing the beautiful selection was easy, and selecting pieces that brightened my home was very satisfying and enjoyable.
ScottTrant –
While browsing casually through different stores, I came across browse smart shop hub and found a nice variety of products, which made looking through different options feel easy and pleasant.
JamesGrify –
In assessments of modern vendor platforms experts frequently highlight the importance of clear navigation fast loading times and well structured product catalogs for better usability Ivory Cove Product Grid users can browse efficiently with minimal effort and easily compare items across different categories
Willierer –
During a late evening search for ecommerce stores offering handcrafted and lifestyle items I compared multiple websites for design and usability and discovered Olive Orchard Vendor Gallery and checkout was simple and the product quality exceeded my expectations today which made browsing effortless and the entire shopping process feel well organized and trustworthy overall
JamesDup –
pharmacy website india: buy prescription drugs from india – legal online pharmacy
JohnnyPut –
As part of my online browsing routine, I came across this simple yet effective shop – its layout keeps everything accessible, ensuring a smooth experience when browsing through various items.
Roberthen –
While analyzing ecommerce UX designs centered on structured layouts and navigation ease, I observed that line-based shop designs improve browsing comfort and clarity, which was evident when reviewing easy navigation shopping center – The layout feels clean and organized, making it simple to locate products.
RobertIcods –
many users appreciate digital stores that emphasize cart organization and intuitive navigation helping them browse products more efficiently while maintaining a clean and structured shopping environment smart place cart navigator known for simplicity – it provides a comfortable shopping experience where users can easily manage selections in their cart and explore categories without unnecessary complexity or interruptions during browsing
HarrySic –
Online retail platforms are increasingly designed to reduce friction in browsing by organizing large inventories into structured categories that improve search efficiency and usability WideMarket Flow Center – Wide selection available here comes with competitive pricing, giving customers a practical way to explore products and select items that best fit their needs and preferences
RandomNamehiexy –
ForestCoveCommerceAtelier – Clean layout, products are easy to explore and understand.
AntonioArola –
In analyses of streamlined digital marketplaces and simplified UI structures, references such as streamlined field marketplace view often appear within commentary sections – The platform is usually seen as a clean browsing environment where users can access product categories without distractions or heavy interface elements slowing down navigation.
Davidfarne –
In the process of evaluating digital commerce platforms focused on direct buying efficiency, I found that streamlined checkout systems enhance satisfaction and usability, which became evident when reviewing efficient order flow hub – The platform is simple and direct, making navigation clear and the buying process smooth.
JamesAssup –
Users prefer platforms that offer a nice experience overall, browsing content is simple and very pleasant without unnecessary complexity Pine Harbor catalog entry I found everything easy to locate
Justinlek –
While browsing through a few online shops for practical products, I came across visit this store and felt that it offers a nice range of everyday essentials, making it something I might casually suggest to friends later.
Byronlow –
While reviewing ecommerce platforms optimized for browsing flow and usability, I noticed that stacked interfaces make product discovery more intuitive by reducing clutter and improving structure, which stood out when exploring smart layered stack index – The design feels smooth and easy to navigate, allowing users to scroll through products effortlessly and efficiently.
Philipcef –
During my time checking different online stores, I encountered this accessible marketplace page – everything is well organized, making browsing simple and enjoyable.
EdwinLedge –
In the middle of checking different eCommerce sites, I paused at take a look speak store and found that the products seem interesting, while the descriptions are clear and easy to understand for quick browsing.
Billyfax –
In discussions about user friendly e commerce platforms, many reviewers highlight the value of simple navigation structures that reduce friction during browsing sessions, and here Ridge Vendor Market Point the system maintains a well organized layout that helps users effortlessly explore listings while keeping everything logically arranged and easy to follow across different product sections.
Georgetic –
While conducting usability research on ecommerce systems emphasizing cart flexibility and checkout clarity, I noticed that adaptable cart designs improve user engagement, which became evident when analyzing smart cart options portal – The cart feels flexible and practical, while the checkout process is straightforward and quick for everyday use.
RandomNamehiexy –
moderndealsstore.shop – Modern design with appealing deals, overall browsing experience feels smooth
FloydTrend –
During a weekend search for artisan ecommerce platforms I evaluated different websites for catalog clarity checkout speed and customer service and discovered Silk Grove Goods Hub – Great selection shipping was quick and customer support was friendly too and the overall platform felt well structured easy to use and very comfortable for browsing multiple categories
Antoniohah –
During a casual browsing session, I encountered this easy shopping atelier – everything is clearly displayed, the selection is strong, and shopping feels very simple overall.
Anthonyter –
While reviewing ecommerce systems designed for clean navigation and user-friendly structure, I noticed that shopping hubs improve clarity and reduce confusion, which stood out when exploring easy shopping navigation hub – The browsing experience is smooth, and all sections are clearly organized for easy access.
Delmartreli –
Users exploring different marketplace reviews and curated shopping lists often see mentions like shopping variety center integrated into paragraphs discussing catalog breadth and navigation design – It is typically portrayed as a broad retail space that brings together multiple categories for convenient browsing
Anthonyfielf –
I recently checked out several online marketplaces and noticed this dependable store layout – the purchasing flow is smooth, with each page loading correctly and guiding users through checkout efficiently.
EdwinPak –
While conducting usability research on ecommerce websites with structured navigation systems, I observed a section titled easy access port index – The port style layout keeps everything organized and simple, allowing users to explore categories smoothly and find products without unnecessary distractions or confusing interface elements.
DouglasFap –
While casually checking new eCommerce platforms, I encountered visit this page now and even though it was my first time there, the organized interface made it easy to navigate and instantly likable.
Lorenlah –
While browsing through multiple eCommerce options, I came across this friendly product page – the design is clean and simple, making the shopping experience smooth and very easy to use.
HerbertPholf –
As I continued exploring various online stores, I landed on browse trend goods store and saw appealing trending items that make me think I might try ordering something from here soon.
Jeffreyamofs –
When examining modern vendor platforms designed for efficiency, scalability, and improved user interaction through simplified navigation and fast response times, Brook Commerce Foundry Space stands out because fast loading pages create a smooth shopping experience that feels consistent, reliable, and easy to manage across different browsing scenarios.
EduardoGof –
During a comparative study of online marketplaces emphasizing speed and usability, I discovered that fast cart systems enhance browsing comfort and engagement, which became clear when reviewing rapid access shopping center – The platform responds well and loads quickly, making the shopping corner highly efficient.
EdgarWrirm –
During evaluation of modern online apparel stores, I came across a page labeled fashion trend showcase portal – The interface highlights stylish clothing items in a visually appealing manner, creating a fresh and trendy shopping environment that feels easy to navigate and pleasant for everyday browsing.
JamesDup –
online drugs order: Mexican Pharm – Mexican Pharm
GeraldAmili –
Users prefer platforms with strong layout design because navigation is easy and user experience remains smooth today Harbor Stone goods directory I liked how fast everything loaded
AlbertCyday –
I recently explored multiple eCommerce platforms and found a href=”[https://frostbrookvendorfoundry.shop/](https://frostbrookvendorfoundry.shop/)” />this organized vendor interface – everything is well designed, and the shopping experience feels smooth, simple, and easy to navigate.
DonaldNob –
In the process of evaluating online retail systems focused on cart operations and checkout flow, I found that structured usability improves clarity and engagement, which became evident when testing digital checkout cart hub – The open cart solution is functional, and shopping steps feel easy, simple, and well organized.
Geraldkat –
People searching for convenient household shopping options often rely on sites such as essential living shop when selecting products for daily home use – It is typically viewed as practical and provides an easy way to access common home necessities in one place
MartinLob –
While exploring different ecommerce sites for gift ideas and decorative products, I found Gilded Grove Goods Route Finder and appreciated how easy it was to navigate, with well-structured sections that made everything understandable quickly and improved overall browsing flow.
JamesRiz –
Modern e-commerce users often value efficiency above all else when completing online transactions, especially when browsing multiple categories in one session, and a strong example is FastLane EasyCart Shop – The platform is designed to keep checkout steps minimal so users can move quickly from cart to confirmation without confusion or delay
Thomasmof –
In the course of evaluating online retail platforms focused on usability and structured design, I found that smart hub systems improve shopping efficiency by streamlining navigation, which was evident when analyzing smart retail navigation portal – The platform feels well structured and efficient, allowing users to browse products smoothly through an intuitive and organized interface.
ManuelFex –
While reviewing different shopping websites, I encountered this easy-to-use shop – the arrangement of products is clear and logical, allowing visitors to browse through selections without unnecessary distractions.
Williamscone –
As I explored different eCommerce websites, I stopped at enter point goods store and noticed everything is neatly arranged, making browsing through categories feel convenient and straightforward.
RobertRef –
In between reviewing multiple eCommerce platforms, I explored discover this value shop and found pricing that looks competitive, so I intend to explore more products later today when I have free time.
DavidFause –
During a comparative study of online retail systems emphasizing cart optimization and seamless checkout design, I discovered that structured cart solutions enhance usability and speed, which stood out when analyzing smart shopping cart portal – The platform delivers efficient cart functionality, ensuring browsing and checkout remain smooth and easy throughout the experience.
Edgargautt –
Many reviewers of online retail systems emphasize how important it is for platforms to maintain a balance between visual simplicity and functional depth in order to support effective product discovery and user satisfaction Cove Digital Atelier Hub – Navigation is smooth and intuitive, allowing users to move between sections effortlessly while browsing products.
DorianBOR –
users comparing ecommerce platforms often highlight the importance of responsive page loading and structured navigation systems that allow them to browse products quickly and efficiently across multiple sections link cart explorer view known for usability – it delivers a seamless browsing experience where users can click through pages effortlessly while maintaining clarity and smooth navigation throughout their shopping session
BillywaW –
During a general browsing session, I came across this clean commerce portal – pages load quickly, the experience is nice, and everything looks organized and clean.
WilliamMum –
In the process of analyzing digital deal platforms focused on speed optimization and usability, I found that fast hubs enhance user experience and efficiency, which became evident when reviewing fast promo savings portal – The fast deals hub loads quickly, and the offers feel engaging, attractive, and time saving.
Patrickbuh –
When exploring consumer shopping guides and digital retail summaries, people sometimes see references like market saver station – The platform is often associated with affordability focused browsing and a selection of goods aimed at helping users find reasonable prices across common product types.
HowardkeD –
During casual exploration of online marketplaces for home accessories I checked different platforms and found Rain Harbor Shopping Vault which impressed me with its clear structure and responsive interface that made browsing quick and simple – Items arrived promptly the website was intuitive and the entire process felt smooth efficient and very user friendly overall
Rickytab –
In the process of evaluating online retail systems for design quality, I observed a module labeled comfort nest product hub – The interface uses a cozy design approach that makes browsing feel natural and easy, helping users explore categories without stress or unnecessary complexity affecting their shopping flow.
DustinVak –
During analysis of online retail platforms focused on simplicity and user experience, I discovered that minimal cart systems improve navigation efficiency and satisfaction, which became clear when testing simple purchase portal – The design is very easy to follow, ensuring a smooth shopping experience without confusion.
JasonFluip –
During my exploration of online fashion platforms, I encountered see this clothing store and found the prices look reasonable, while the clothing designs appear modern and stylish for everyday fashion use.
Josephmusia –
A structured layout where good interface design makes browsing straightforward and highly convenient overall improves experience Oak Meadow browsing center everything felt very accessible
Thomassal –
While browsing through various online marketplaces today, I came across visit this shop point and noticed some interesting items that caught my attention, making me think I might return later to explore more products in detail.
AlfredjoynC –
Across many digital retail studies focused on improving browsing efficiency and reducing friction in user experience flows, experts often point out the importance of clear categorization and responsive design systems Harbor Gallery Product Atlas – The layout is visually clean and well structured, making product discovery smooth and easy to follow.
RandomNamehiexy –
people searching for online shopping solutions often prefer direct navigation websites that eliminate unnecessary steps helping them browse products faster and complete shopping more efficiently across categories direct shopping explorer hub widely seen as practical – it delivers a seamless browsing experience where users can easily find items and navigate categories without confusion or unnecessary complexity during interaction flow
Devinasync –
While exploring various online marketplaces, I found this well-crafted shop – the layout appears clean and structured, giving off a professional vibe that makes browsing both easy and pleasant.
DennyTwefe –
People who enjoy online shopping often choose platforms that focus on smooth browsing and reliable deal availability where easy marketplace nest hub appears in content and it reflects a system built to enhance browsing efficiency while helping users quickly discover products and complete transactions across various everyday shopping categories with ease.
pinup_orMa –
pin-up slotlar bonus [url=https://www.pinup39174.help]https://www.pinup39174.help[/url]
JamesDup –
Canadian Tabs: pharmacy com canada – Canadian Tabs
Charlesswise –
In studying ecommerce interfaces inspired by natural branching systems, I observed that user engagement improves when browsing platforms like smart branch market point – The smart branch structure organizes shopping paths efficiently, helping users transition between product categories in a smooth and predictable way.
GeraldopIns –
Users looking for budget conscious shopping solutions often review platforms that emphasize simplicity, and a notable example is budget friendly hub which compiles deals in an organized format; overall it is described as smooth to navigate and helpful for people aiming to find affordable options across global markets
Glennextes –
People who prefer structured online shopping environments often choose marketplaces that provide clear categories and regularly updated promotions where daily deal access hub appears in content – it highlights a user friendly system that simplifies browsing and ensures customers can quickly find relevant discounts across various product types.
AlvinSof –
As I explored different e-commerce pages, I came upon this smooth shopping link and found interesting products listed, with the browsing experience feeling fast, easy, and conveniently straightforward.
Josephbub –
During a casual evening of exploring new ecommerce websites, I found a marketplace that offered a surprisingly wide catalog of goods, and while reviewing product pages I encountered Harbor Coast Shopping Parlor placed within a seamless layout, and the overall impression was that checkout was straightforward, with good variety and a relaxed browsing experience that felt dependable and user-friendly.
Jameslon –
While conducting comparative research on ecommerce UX and smart marketplace design, I observed that structured systems improve navigation and user satisfaction, which was clear when testing smart shopping category hub – The marketplace is neatly organized, allowing quick access to products across different sections.
Willieclutt –
While exploring ecommerce systems focused on improved navigation clarity, I came across a module titled branch flow marketplace hub – The tree structure organizes products in a way that enhances understanding and makes browsing categories efficient and easy for users across all sections of the platform.
CraigFeria –
During my browsing session across multiple sites, I encountered this blunty themed page and after checking it out, it surprisingly feels quite interesting overall, with a simple but engaging structure.
RussellJed –
As I continued exploring different online stores, I landed on browse shop rise market and saw a good first impression, with a clean design that makes navigation feel easy and comfortable throughout browsing.
JesseMop –
While checking humanitarian racing campaigns, I noticed karting support mission hub and interesting concept overall, seems well organized and quite engaging today, offering a structured view of events designed to support charitable efforts through sport. – It feels clear and community focused.
RandomNamehiexy –
openmarketshop.shop – Open market vibe, lots of items available in one place
AlbertoGrany –
When analyzing online shopping behavior, experts frequently mention that simplicity in interface design directly improves usability and encourages longer browsing sessions Jewel Brook Vendor Hub – Users enjoy an easy and comfortable browsing experience, with smooth navigation across clearly structured product sections.
DonaldPat –
While casually browsing for products online, I discovered visit this page now and saw that the pages open fast, with a decent layout that keeps the shopping experience calm and simple to follow.
DennyTwefe –
Consumers frequently searching for online deals tend to prefer platforms that provide smooth navigation and active discounts where quick nest shopping hub appears in guides and it reflects a structured system designed to simplify browsing while helping users easily compare products and complete orders quickly with a hassle free experience overall.
Thomasnup –
In studying online retail platforms emphasizing fair pricing structures, I observed that simplicity in deals improves usability when exploring systems such as useful savings hub portal – The marketplace offers reasonable pricing and practical deals that support smarter purchasing decisions for everyday buyers.
Eddiegob –
Researchers examining digital commerce platforms frequently assess how layout design impacts user purchasing behavior and browsing comfort port cart explorer referenced in studies – Users benefit from a clean structure that supports efficient product exploration.
Blakedef –
In the middle of exploring various shopping sites, I came across this user-friendly platform – its easy navigation and well-organized product listings create a smooth and pleasant browsing experience.
Georgesearf –
While reviewing ecommerce UX systems designed for discount visibility and savings clarity, I observed that deal corner layouts enhance shopping decisions by emphasizing reduced prices, which became clear when testing discount value deal portal – The deals look appealing and well structured, giving the impression of a platform that is ideal for budget conscious shoppers.
Damonalore –
During my evaluation of online vendor platforms, I found a clean and modern look, everything works well and loads quickly across all pages and categories Opal River browsing portal navigation felt intuitive and stable
StuartTaurl –
In the process of exploring e-commerce platforms, I came across this straightforward shop link and noticed that the products appear useful, with a clean layout that makes the browsing experience feel smooth and uncomplicated overall.
Joshuafen –
During my search for unique artisan marketplaces I compared several platforms for reliability and product transparency when I discovered Coral Meadow Trade Showcase – I found the product details to be highly accurate and shipping speed exceeded expectations making the overall experience smooth trustworthy and genuinely satisfying from start to finish without any issues
RandomNamehiexy –
While conducting comparative research on ecommerce checkout systems and cart design efficiency, I observed that smart cart corners improve usability by keeping checkout steps organized and minimal, which was clear when testing intuitive purchase cart center – The layout feels practical, with a smooth and simple checkout flow that supports easy purchasing decisions.
StevenWholi –
People who appreciate aesthetic fashion often search for brands that offer curated clothing collections focused on modern simplicity and expressive personal style Modern Apparel Collection Hub – featuring a fashion platform dedicated to stylish clothing and aesthetic inspired designs that blend elegance and comfort while offering versatile wardrobe pieces for individuals with a taste for contemporary trends
Zacharyhom –
Across various online shopping guides, references such as are sometimes placed in the middle of explanatory text – It gives the impression of a diversified retail platform designed to showcase many product categories in a single accessible location.
WilliamSpult –
As I continued browsing different web pages, I noticed this online personal hub and found it while browsing, and the content seems pretty decent, with a simple design that helps keep everything readable and easy to understand.
JackieTic –
While browsing general e-commerce pages, I came across straightforward shop platform and the shopping experience here looks simple, clean, and surprisingly intuitive overall, offering users a minimal interface that reduces friction during browsing. – It feels practical, clean, and easy to use.
Thomasdib –
During comparative browsing of online retail systems, I encountered a section labeled shopdock product directory hub – The layout is simple and clean allowing users to navigate categories efficiently without unnecessary complexity in design making browsing smoother for everyone overall experience.
Glennextes –
Many consumers prefer online shopping environments that offer structured categories and clearly displayed promotions for improved browsing efficiency where deal finder shopping corner appears in content – it reflects a marketplace designed to simplify product discovery while ensuring users can quickly access discounts and complete transactions with ease and confidence.
Roberttus –
While casually browsing electronics stores, I discovered visit this gadget shop and saw that the tech items look interesting, but I am hoping the real quality is consistent with the descriptions provided online.
JohnnieSex –
While reviewing ecommerce systems designed for step-based product journeys and guided navigation, I observed that structured browsing enhances usability and satisfaction, which was evident when exploring step guide discovery portal – The step-based browsing feels clear, and product discovery is simple, structured, and intuitive.
StanleySmalp –
In the process of evaluating digital marketplaces focused on global cart systems and product accessibility, I found that unified cart models enhance usability and browsing efficiency, which became evident when reviewing global online cart portal – The design follows a global cart concept, making a wide range of online products easy to browse and compare.
Jamesdut –
Digital commerce comparisons frequently highlight differences in checkout efficiency and how effectively websites guide users through payment completion steps checkout efficiency tool when examining real-world user interactions and cart testing scenarios – The flow feels consistent and designed to minimize confusion during purchase finalization.
JohnnyNal –
People who enjoy structured digital shopping often look for marketplaces that provide clear product variety and a nice browsing vibe making it easier to explore categories efficiently Violet Harbor Market Flow Hub – providing a clean marketplace where merchant lane design enhances product visibility and ensures smooth browsing for users navigating multiple categories in one place
Jamesutili –
As I continued exploring home product websites, I encountered this simple goods hub and appreciated how easy it is to navigate, with everything structured in a way that supports quick and hassle-free browsing.
Josephtic –
Many users exploring digital stores often prioritize platforms that combine verified deals with structured browsing systems where value online deals hub appears in informational content and it reflects a structured system designed to improve browsing speed while helping users quickly access products and enjoy a seamless and efficient shopping journey across categories.
JamesDup –
п»їlegitimate online pharmacies india: Indian Meds Delivery – overseas pharmacy no prescription
StevenWholi –
People interested in contemporary fashion frequently search for brands that blend minimal design with stylish clothing pieces suitable for versatile everyday wear and creative self expression Aesthetic Clothing Collection – presenting a modern fashion website that showcases curated apparel collections focused on elegance simplicity and trend inspired designs created for individuals who appreciate refined and stylish wardrobe choices
Richardzew –
During analysis of structured ecommerce layouts, I came across a section labeled axis retail browsing hub – The design organizes products neatly in a logical flow, making it easy for users to explore items without confusion or unnecessary complexity in the interface design.
JamesGew –
While exploring online marketplaces, I stopped at explore kitchen tools shop and found the kitchen tools selection looks very useful, making me think I could pick something for home use.
Thomasrib –
While spending time exploring different online marketplaces, I came across something interesting like this efficient product site – browsing through the pages feels smooth, and finding items is quick and straightforward without any unnecessary complications or delays.
Shannonwhoms –
As I explored different websites, I noticed this brownback clone link and after reviewing it briefly, it looks quite decent overall and seems like a platform that could be worth exploring further to understand what it offers in more detail.
SheltonSmoli –
While reviewing unusual digital concepts, I encountered this baby bonus experimental site and it seems like a niche idea, but still quite interesting overall, presenting something that feels different yet fairly easy to grasp.
BrianSault –
Shoppers looking for efficient e-commerce experiences frequently prefer platforms that combine affordability with smooth navigation tools where quick savings hub portal appears in descriptions and it represents a system designed to simplify browsing while helping users discover budget friendly items and complete transactions without unnecessary delays or confusion.
Charleslut –
many digital buyers prefer ecommerce websites that enhance user experience through simple navigation and well organized category structures making product discovery faster and more efficient across all sections quick shop zone guide often appreciated for clarity – the platform delivers a smooth browsing experience where users can explore products easily while enjoying a consistent layout that supports stress free navigation and efficient category movement throughout
Simonsouri –
During a comparative study of online marketplaces emphasizing modern design and usability, I discovered that corner layouts enhance engagement and simplify shopping, which became clear when reviewing clean modern cart hub – The design appears sleek and organized, making the shopping experience feel easy and user friendly.
Kennethduema –
In between reviewing different discount stores, I explored discover this deals page and felt that the offers are attractive enough to consider buying something from here quite soon.
Thomasnup –
During analysis of structured online deal platforms, I noticed that transparent pricing boosts engagement when using systems such as value driven market hub – The offers seem practical and fairly priced, making it easier for users to identify relevant products without confusion.
Randyartek –
users comparing ecommerce websites often look for platforms that provide quick navigation and clearly structured categories making it easier to browse large inventories without confusion plus browse lane appreciated for its usability and flow – it supports smooth movement between categories while maintaining a consistent and easy to understand shopping interface overall experience
RaymondUnfon –
While reviewing various retail websites, I found this quick browsing store and liked how the layout responds instantly, making shopping feel fast, smooth, and convenient for users who prefer simple and direct navigation.
JamesSerly –
Online buyers who appreciate modern e commerce designs often explore platforms that use clean interfaces and creative vault themed product organization for easier shopping Crown Cove Digital Vault – featuring a user friendly layout combined with an innovative vault style concept that helps shoppers find products quickly while enjoying a visually structured and simplified online retail environment
StevenWholi –
Individuals exploring new fashion ideas often prefer online platforms that showcase modern clothing with aesthetic inspired designs suitable for everyday styling Modern Elegance Fashion Hub – presenting a curated clothing platform that emphasizes stylish apparel aesthetic design principles and wearable fashion collections tailored for individuals seeking balanced and contemporary wardrobe inspiration
Eduardokix –
Consumers who appreciate online shopping often choose platforms that simplify navigation and highlight fast transaction systems where easy cart deal center appears in descriptions and it reflects a system designed to improve efficiency while helping users easily find products and complete purchases with minimal effort and maximum convenience.
Lloydvef –
During my search for online stores, I explored visit this all goods page and noticed it is a nice all-in-one store, with varied items that make browsing feel simple and efficient.
KevinSouff –
While reviewing different ecommerce platforms focused on navigation systems and user experience design, I noticed that route-based structures often improve how users discover products efficiently, especially when browsing large catalogs, which became clear when analyzing smart route shopping hub – The route based navigation feels very intuitive, helping users find items easily through clear pathways that make browsing smooth, structured, and naturally simple across all product categories.
TimothyDrave –
Online buyers often appreciate platforms that bring together different product categories while maintaining clear structure and easy navigation where combined shopping hub appears in guides describing user friendly design – it reflects a system that allows customers to explore various goods and complete purchases smoothly without confusion.
Georgekaw –
As I continued checking online discussion content, I noticed debate analysis portal and thought it was interesting, definitely catching my attention for a short while due to the structured and opinion-driven nature of the writing.
Charlescug –
While browsing hospitality booking pages, I came across tango themed accommodation hub and hotel related content appears helpful, informative, and easy to navigate, with details presented in a way that feels clear and accessible for travelers. – It feels organized and practical.
GregoryHen –
While performing a final comparative scan of agri ecommerce portals, I reviewed a section called field harvest marketplace center – The field inspired browsing structure ensures users can navigate categories smoothly and discover products without unnecessary complexity overall experience is clean.
Williamdoora –
While analyzing ecommerce platforms optimized for variety and user accessibility, I noticed that all-in-one store systems improve engagement by offering everything together, which stood out when reviewing all products in one portal – The store feels comprehensive, with many different items available in one place for easy exploration.
RichardCor –
While exploring various retail platforms, I found this efficient store layout – everything loads quickly, making the shopping process smooth and dependable.
RalphAccen –
Главные новости: https://stritstroy.ru
ClairFon –
While reviewing ecommerce marketplaces focused on performance efficiency, I observed that fast-loading pages enhance usability, which was clear when testing quick commerce portal hub – The quick online market is responsive, and pages load fast and smoothly without lag.
ShaunDyday –
As I browsed through multiple online shops, I stopped at check it out and found that the mobile accessories are designed with a clean modern look that feels quite appealing overall.
JessieFek –
As I explored e-commerce options, I came upon this uncomplicated store link and found it effective in simplifying the shopping experience, making it more accessible and easier for everyday use.
JefferyMup –
Individuals who enjoy efficient online marketplaces often look for platforms that offer smooth shopping flow with many different goods available in one place making browsing more intuitive and user friendly Silk Valley Multi Goods Hub – featuring a structured shopping experience where diverse products are displayed together in one marketplace designed to provide smooth navigation and easy discovery across all categories
StevenWholi –
Individuals passionate about modern fashion often explore websites that present curated clothing lines featuring aesthetic inspired designs and stylish wearable pieces Aesthetic Wardrobe Boutique – showcasing a fashion platform that highlights modern clothing collections focused on elegance simplicity and trend aligned designs created for individuals who value expressive yet minimal personal style choices
mostbet_mfKi –
mostbet plinko oyun [url=https://mostbet2015.help]https://mostbet2015.help[/url]
StephenAtove –
While comparing multiple eCommerce platforms, I landed on go to easy pick shop and noticed that picking items is simple, with a layout that helps make browsing organized and efficient overall.
MartyUtila –
Many digital shoppers appreciate platforms that offer organized product listings and intuitive navigation fast checkout arena This improves overall user experience and speeds up browsing time for all users today – Design structure supports efficient exploration of multiple categories generally
PhilipBef –
Many users exploring digital stores often prioritize platforms that combine speed with clean layouts where value quick buy hub appears in informational content and it reflects a structured system designed to improve browsing speed while helping users quickly access essential goods and enjoy a seamless and efficient shopping experience overall.
RoscoeTieds –
Modern shoppers often appreciate platforms that remove traditional barriers in cross border shopping and provide direct entry to global product listings in a simple format global trade shopping portal making it easier to browse and purchase items from multiple countries without unnecessary complications – It highlights the increasing importance of frictionless international e-commerce experiences for users worldwide.
JamesDup –
pharmacy com canada: Canadian Tabs – Canadian Tabs
StephenCak –
As I reviewed different informational platforms, I discovered this clean email overview site and liked how simple everything is arranged, making it easy to navigate and understand without any confusion.
Petereneft –
In the process of analyzing digital commerce platforms focused on layout clarity and usability, I found that stacked systems enhance browsing by presenting products in a clear sequence, which became evident when exploring organized stack product hub – The layout looks clean and structured, making browsing feel clear, efficient, and easy to follow overall.
Larryhaity –
In the process of exploring dessert ideas online, I came across this Fabulicious sweets inspiration page and everything looks delicious here, making the site feel very appealing, with a layout that feels modern and appetizing.
TrevorNip –
many online shoppers prefer websites that simplify browsing through guided category flows helping them find products quickly while maintaining a clean and organized interface throughout trail shopping path explorer widely appreciated for usability – it offers a structured browsing experience where users can follow navigation steps easily and enjoy a consistent and efficient shopping environment overall
HoraceKam –
During a comparative analysis of ecommerce savings platforms, I found a listing called discount product discovery portal – The interface is structured to highlight appealing prices and promotions, encouraging users to explore further while maintaining a smooth and simple browsing experience across all categories.
Harveytaulk –
While reviewing ecommerce systems designed for step-based product journeys and guided navigation, I observed that structured browsing enhances usability and satisfaction, which was evident when exploring step guide discovery portal – The step-based browsing feels clear, and product discovery is simple, structured, and intuitive.
Edgarcop –
In between reviewing different platforms, I explored discover this site and found that the interface runs smoothly, with products organized in a way that simplifies searching.
Charlescruit –
During my exploration of online shopping sites, I encountered this pleasant browsing hub and found it enjoyable because of its clean design and well-arranged categories that make product searching straightforward and efficient.
StevenWholi –
Fashion lovers seeking updated wardrobe inspiration often explore brands that present minimalist aesthetics combined with trendy and versatile clothing options for everyday use Contemporary Fashion Gallery – providing a digital space showcasing stylish clothing collections and modern aesthetic designs that highlight individuality creativity and comfort while aligning with current fashion trends and lifestyle preferences
Robertpaick –
Customers exploring e-commerce platforms often compare pricing and service quality and on certain pages you might find value savings marketplace highlighted within descriptions that emphasize affordable household goods and dependable delivery services designed to improve everyday shopping experiences for budget conscious buyers everywhere.
GregoryFut –
While navigating through different eCommerce platforms, I came across click to view trend shop and noticed a selection of trendy products that make the site look like a fun place to shop.
Andrewcok –
Shoppers who value creative online stores often look for platforms that use trading post themes to make browsing feel refreshing and engaging while still maintaining a simple and structured shopping experience Orchard Quartz Select Goods Post – offering a structured marketplace where a trading post inspired layout adds freshness to browsing and helps users explore products in a smooth and intuitive way
Jeffreylar –
Many digital shoppers value ecommerce sites that focus on clean presentation and structured browsing systems that make product discovery more intuitive organized shop deck – The design keeps listings arranged in a logical flow so users can move smoothly between categories while maintaining a clear sense of structure throughout the entire shopping process
DavidhiX –
While reviewing ecommerce platforms designed for tech enthusiasts and digital consumers, I noticed that structured layouts improve product visibility, which stood out when exploring smart gadget marketplace portal – The digital shopping point feels modern and engaging, with appealing tech products that draw user interest.
melbet_yxKi –
site oficial melbet [url=http://melbet07892.help]site oficial melbet[/url]
mostbet_zzOn –
mostbet kaszinó apk letöltés [url=mostbet2022.help]mostbet2022.help[/url]
Andrewpag –
Online buyers who enjoy convenience often choose platforms that combine simplicity with organized deals where easy online deals portal appears in guides and it reflects a structured system designed to streamline browsing while helping users quickly find affordable products and complete purchases with ease and confidence across categories.
JamesFauMn –
During my search across travel resources, I discovered this outdoor camp hub and it actually looks like a fun and useful resource to browse, providing useful insights in a clean and easy-to-read format.
JamesPlarf –
As I continued browsing digital entertainment sites, I noticed this Dragged Gaming content page and gaming content seems fun, modern, and fairly engaging to explore, offering a clean structure that enhances usability and flow.
PhillipZex –
Online retail environments are increasingly judged on how well they handle fast browsing sessions, especially when users are exploring multiple offers or seasonal promotions within a short time frame fast track shopfront – feedback often highlights that the interface remains responsive, making it easier to complete shopping tasks quickly and comfortably.
Brucesof –
While analyzing ecommerce platforms optimized for quick cart interactions, I came across a listing titled fast cart browsing hub – The interface ensures immediate response to user actions, making cart management and product browsing seamless, efficient, and free from unnecessary delays or slow loading times.
Pabloamibe –
While conducting usability evaluations of fashion ecommerce platforms focused on style and deals, I noticed that curated hubs improve shopping experience and visual engagement, which stood out when reviewing modern fashion savings portal – The clothing section feels appealing and stylish, and the fashion deals look trendy and well presented.
WilliamReumn –
During my search through retail websites, I encountered this simple shopping platform and it appears to focus on convenience, providing an easy way to access everyday products in a clean and minimal interface.
DavidSal –
In the middle of browsing different online platforms, I paused at take a look hub and found the experience smooth and reliable, as I didn’t encounter any issues while navigating through the content.
RandomNamehiexy –
Shoppers who regularly look for discounts often choose platforms that simplify browsing and highlight cost saving opportunities where best price cart hub appears in content and it reflects a structured environment designed to make online shopping easier while ensuring users can find the most affordable options quickly and effectively.
StevenWholi –
People exploring online fashion stores often prefer platforms that combine aesthetic design with practical clothing collections suitable for everyday modern lifestyles Minimal Fashion Style Hub – offering a curated selection of stylish clothing that reflects contemporary aesthetics and clean design principles while focusing on comfort versatility and modern wardrobe essentials for fashion conscious individuals
MickeyNop –
While reviewing ecommerce platforms optimized for smooth user journeys and structured browsing, I noticed that flow-based layouts enhance usability by maintaining continuity, which stood out when exploring continuous shopping flow hub – The navigation remains smooth throughout various sections, making it easy for users to browse and explore products.
Vincentchoca –
During a longer browsing session, I encountered check way store hub and found a simple shopping flow with a user friendly design that makes browsing easy and convenient.
JerryMes –
Users exploring different ecommerce options often value platforms that guide them through structured paths, such as route based catalog – It presents products in an orderly format that makes browsing more predictable and helps users locate items without unnecessary effort or confusion.
StevenRak –
Shoppers who enjoy visually pleasant online stores often prefer platforms that use lounge aesthetics to enhance browsing flow and create attractive product presentation across all sections Velvet Valley Calm Market Lounge Hub – offering a structured shopping environment where lounge inspired design creates a relaxed browsing experience that helps users explore products comfortably and efficiently
KevinKnips –
Ivermectin First: ivermectin 3mg – Ivermectin First
PhillipOthem –
Shoppers searching for reliable e-commerce platforms often value websites that provide daily deals and smooth browsing experiences where smart daily deal center appears in content and it reflects a system designed to enhance usability while helping users quickly browse products and complete purchases without unnecessary complications or confusion in the process.
GeorgeFoumb –
During review of online retail interfaces with creative visual identities, I observed ocean ripple shop gateway – The design presents a wave inspired aesthetic that feels modern, organized, and easy to navigate while maintaining strong visual consistency across different pages of the marketplace.
Robertsup –
While browsing healthcare and cosmetic treatment websites, I noticed this elegant clinic site and liked how the clean structure and simple navigation made the experience smooth, comfortable, and genuinely easy to follow.
JamesAnype –
During my search through current events pages, I encountered this Fast With Gaza news site and content appears focused on updates, presented in simple readable format, with information laid out clearly for quick reading and awareness.
DavidFoela –
While analyzing digital retail ecosystems focused on cart performance and checkout reliability, I noticed that seamless interaction design improves overall shopping satisfaction, particularly in multi step purchasing flows, which became evident when examining seamless cart experience – The platform feels stable and user friendly, ensuring that cart actions remain smooth, predictable, and easy to control throughout browsing sessions.
Jameslib –
While conducting comparative research on ecommerce UX and cart systems, I observed that flexible cart functionality improves navigation and satisfaction, which was clear when testing simple cart switch center – The platform makes it easy to swap products inside the cart without disrupting the flow.
Donaldwof –
While browsing through bargain-related platforms, I noticed this offer hub page and it seems like a decent place to find rotating deals that may change over time, encouraging repeat visits for updated savings.
JeremyphYnc –
Shoppers exploring online marketplaces often value platforms that simplify browsing and improve overall shopping speed where fast access product hub is included in content describing convenience – it highlights a system designed to help users find what they need quickly while maintaining a smooth transition from browsing to checkout across all sections.
StevenWholi –
People exploring modern apparel often seek fashion platforms that combine aesthetic inspired clothing with stylish and versatile wardrobe collections for daily wear Minimalist Style Clothing Hub – providing a curated selection of modern fashion pieces that reflect clean aesthetics contemporary design and wearable comfort designed for individuals who appreciate simple elegant and trend conscious wardrobe options
RicardoLob –
During a long session of checking different shopping platforms, I paused midway to explore check this store and found the interface clean enough with a fair variety of items, making it something I might return to in the future.
DonaldRor –
many online shoppers exploring general ecommerce platforms often appreciate websites that combine variety with simple navigation making it easier to browse multiple product categories without confusion or delays during everyday shopping sessions total shop hub explorer often described as a convenient marketplace – the platform provides a wide selection of products while maintaining a clean and structured browsing experience that helps users find items quickly and comfortably across all categories available
RandomNamehiexy –
goodsmixstore.shop – Mixed goods selection is useful, plenty of options in one store
Michaeldrism –
Individuals who prefer simple browsing experiences often appreciate platforms that organize products using merchant lane systems that create logical and easy to follow category structures Harbor Jasper Smart Lane Market – featuring a clean online store where products are displayed in a merchant lane format designed to enhance browsing clarity and make shopping more efficient for everyday users
Byroncaund –
People who shop online regularly often choose websites that offer secure checkout processes and reliable cart features where quick trusted cart center is featured in content and it highlights a system designed to improve browsing flow while ensuring users can quickly access products and complete purchases safely across all categories without confusion.
Cecilmug –
In the process of studying digital shopping experiences focused on category flexibility and usability, I found that structured choice systems improve browsing efficiency, especially when users explore different product types, which became evident when analyzing flex product navigation hub – The platform offers variety and enables smooth switching between categories, making shopping feel simple, intuitive, and well structured overall.
Davidstind –
While browsing lifestyle and hobby puzzle platforms, I came across colorful art puzzle gallery and puzzles look creative, colorful, and quite enjoyable for visitors overall, with a style that feels cheerful, artistic, and designed to capture attention through detailed illustrations and bright visuals. – It feels like a relaxing creative escape.
Jefferyseila –
While reviewing various parenting content sites, I encountered this mom lifestyle hub and came across it and found the topics quite relatable today, with posts that feel very grounded in everyday family life.
DanielBed –
While conducting usability research on ecommerce systems emphasizing performance and smooth navigation, I noticed that fast shopping zones reduce waiting time and improve engagement, which became evident when analyzing quick response shopping center – The shopping experience is fast, and pages load smoothly with consistent and reliable responsiveness.
KevinKnips –
Ivermectin First: Ivermectin First – buy ivermectin uk
Michaelatomb –
While going through multiple online retail platforms, I discovered this efficient product hub and found that its structure is thoughtfully designed, so finding items doesn’t require much effort and everything feels logically placed and easy to access.
WilfredOwets –
Many consumers value digital marketplaces that ensure safe interactions between buyers and sellers through verified systems where reliable purchase hub cart appears in guides – it highlights a platform built to deliver secure shopping experiences while maintaining simplicity and ease of use across all transactions.
StevenWholi –
Individuals searching for fashion inspiration often turn to platforms that emphasize aesthetic clothing collections and modern design focused apparel for everyday wear Contemporary Aesthetic Wear Hub – offering a curated selection of stylish clothing that blends modern fashion trends with elegant simplicity and versatile wardrobe pieces designed for expressive personal styling and daily comfort
Marcosdex –
In the middle of checking different marketplaces, I paused at take a look value shop and found several reasonably priced options, which makes it worth coming back to explore again later.
Waltercix –
While conducting usability research on online deal-based marketplaces, I observed a section titled digital savings shopping portal – The design emphasizes affordability and clarity, allowing users to quickly browse tech products while enjoying a smooth experience focused on well priced online shopping options overall.
Terrynuava –
While browsing religious gathering information platforms, I noticed iftar support community site and information here seems community focused, helpful, and well structured content, presenting details in a clear format that makes understanding community events simple and accessible. – It feels structured and easy to follow.
JamesAbupt –
Individuals who enjoy browsing online deals often prefer outlet stores that emphasize clarity structured categories and a decent selection of useful products Cloud Cove Bargain Outlet Hub – presenting a simple and efficient shopping platform focused on ease of navigation and practical product listings designed to help users quickly locate affordable items in an organized digital space
LarrySpona –
Online shoppers often prefer platforms that simplify purchasing processes and provide smooth transaction experiences where easy buy shopping hub appears in listings and it highlights a system designed to help users quickly select products and complete purchases with minimal effort while enjoying a seamless and efficient browsing experience across multiple categories.
RobertJut –
During my review of festive event platforms, I found this Christmas event guide and it feels like a nicely put together site with good information, clearly presenting details in a way that is simple to follow.
Darrickpoill –
While reviewing digital shopping platforms focused on cart zones and fast checkout processes, I observed that clarity and structure improve user experience, which became clear when testing smart cart zone center – The open cart zone appears clean, and checkout is simple, fast, and easy to complete.
Homervep –
Consumers exploring digital shopping options frequently choose platforms that enhance speed and clarity when they use fast track cart system while shopping online – It reflects a streamlined environment focused on reducing checkout time and improving overall user convenience.
Mariodrulk –
As I reviewed different support-oriented websites, I came upon this clear counselling link and noticed how effectively it communicates important information in a way that feels caring, structured, and accessible to a wide audience.
StevenWholi –
Individuals interested in trendy clothing often explore online fashion platforms that highlight aesthetic inspired designs and modern wardrobe essentials Fashion Aesthetic Collection Space – presenting a curated selection of stylish apparel focused on modern design trends aesthetic appeal and wearable comfort for individuals who value creativity simplicity and elegant fashion expression
KevinKnips –
best online pharmacy no prescription: medicine online order – medicine online order
JamesHeinc –
While browsing football tournament information sites, I noticed global match results tracker and sports related updates feel exciting, timely, and easy to follow, offering structured updates that feel useful for staying informed on ongoing competitions. – It feels smooth and easy to read.
JasonTug –
As I reviewed various online shops, I came upon this well-structured marketplace and found the layout very effective, allowing users to locate items easily with minimal effort and a smooth browsing experience.
Lindseycip –
Shoppers who value security in online purchasing often look for platforms that make cart navigation simple and safe where quick secure cart portal appears in guides and it reflects a structured system designed to improve usability while helping users quickly compare products and complete transactions without unnecessary delays or complications.
Richardageme –
Shoppers who value creativity in online shopping often enjoy platforms that use market studio design to make product listings more visually appealing while maintaining clean structure and easy navigation Willow Kettle Artistic Market Studio Hub – offering a charming e commerce environment where products are presented with creative studio inspired design enhancing visual appeal and providing users with a smooth and enjoyable browsing experience across all categories
Jamesgueve –
Online consumers often seek platforms that prioritize speed and ease of use when buying routine goods where simple goods network appears in descriptions focused on practical shopping – the site emphasizes accessibility and convenience, allowing users to browse daily essentials and complete orders with minimal effort or confusion during the checkout process.
Leroykax –
While exploring various websites for ideas, I encountered visit this site – It gives off a really nice impression right away, with a layout that feels thoughtfully arranged and visually consistent, making the experience feel smooth and pleasant.
ThomasZep –
While reviewing a range of educational websites, I found this engaging resource and liked how it explores a specialized topic while maintaining a clear and approachable writing style that keeps the reader involved.
StevenWholi –
People exploring modern apparel often seek fashion platforms that combine aesthetic inspired clothing with stylish and versatile wardrobe collections for daily wear Minimalist Style Clothing Hub – providing a curated selection of modern fashion pieces that reflect clean aesthetics contemporary design and wearable comfort designed for individuals who appreciate simple elegant and trend conscious wardrobe options
mostbet_ruMi –
mostbet instalare din surse externe [url=http://mostbet40596.help/]http://mostbet40596.help/[/url]
mostbet_bcen –
mostbet sportovní nabídka Česko [url=www.mostbet32570.help]www.mostbet32570.help[/url]
DennisalimA –
During a general browsing session, I encountered check it out – It feels clean and modern overall, and browsing is smooth and well organized, making navigation simple and comfortable.
DonaldPah –
While going through theoretical philosophy blogs, I came across chaos interpretation discussion site and unique concept presented here, thought provoking and quite intriguing overall, with ideas that feel exploratory, deep, and slightly paradoxical in nature. – The tone feels thoughtful and analytical.
Victorden –
People searching for reliable e-commerce solutions often prioritize platforms that reduce effort and simplify access to essential household goods instant shopping cart center making it easier for customers to complete purchases quickly while maintaining access to a wide range of products.
Larrycib –
While conducting usability evaluations of ecommerce platforms focused on clarity and simplicity, I noticed that basic layouts improve user engagement by simplifying navigation, which stood out when exploring easy shopping base hub – The layout feels clean and organized, allowing users to browse products easily.
Kennethmat –
During my search through apparel platforms, I discovered this style clothing page and it looks like a solid place to check out different styles, with a collection that seems both diverse and easy to navigate.
Stevenbab –
People who prefer curated shopping experiences often enjoy platforms that organize products in boutique hubs where everything is arranged neatly to suit various customer preferences and needs Grove Harbor Daily Goods Hub – providing a clean and efficient e commerce platform where curated items are displayed in a boutique style layout designed to help users browse easily and discover products suited for everyday use and convenience
StevenWholi –
Fashion enthusiasts frequently look for online brands that offer stylish collections designed around modern aesthetics and versatile clothing options for daily wear Contemporary Style Clothing Hub – providing a curated fashion experience featuring elegant apparel and aesthetic inspired outfits designed to support modern lifestyle preferences while emphasizing creativity and wearable design innovation
KevinKnips –
dog medicine: Vet Pharm First – online pet pharmacy
DanielFag –
During a general browsing session, I encountered check it out – After taking a quick look, the site layout appears clean and simple, making it easy to navigate through different sections comfortably.
DonaldShern –
In the middle of reviewing health research content, I discovered information clarity page and found the presentation very easy to digest, with a logical flow that helps readers follow the material without confusion or difficulty.
Kevinhiexy –
besttrendstation.shop – Easy to navigate site, everything feels structured and user friendly.
Jeffreybog –
During a comparative analysis of online marketplaces focused on interface design and layout efficiency, I discovered that grid systems are commonly used to enhance clarity and improve browsing flow, which stood out when exploring structured grid shopping portal – The interface presents products in a clean and logical grid arrangement, making it easy for users to explore items without confusion or unnecessary complexity.
DennyTwefe –
Many consumers exploring online deals often prefer platforms that offer clean layouts and easy browsing tools where quick shop deals center is included in descriptions and it highlights a system designed to improve browsing efficiency while ensuring users can easily access products and enjoy a smooth and intuitive shopping journey overall.
CarltonDub –
While evaluating online shopping platforms focused on smooth navigation and usability, I noticed that simplified systems enhance engagement and clarity, which stood out when analyzing streamlined commerce portal – The design is smooth, and product browsing feels quick, simple, and easy to use.
EdwardDES –
During a general browsing session, I encountered check it out – It has a simple layout, loads quickly, and feels easy to navigate, making the browsing experience smooth and user-friendly overall.
HenryBioro –
While reviewing ecommerce UX systems optimized for reliability and ease of use, I observed that trusted hubs improve clarity and reduce friction, which became clear when testing secure shopping portal hub – The browsing experience feels reliable and smooth, making navigation simple and user friendly.
Felixcar –
Shoppers who frequently buy online tend to favor websites that simplify the entire purchasing experience where smooth checkout cart hub is referenced in guides – it represents a user centered design approach that reduces friction, making it easier for customers to move from browsing to completing their orders in a fast and efficient manner.
BrendonJuign –
Online electronics buyers appreciate platforms that simplify deal searching while keeping listings updated and easy to understand Gadget Smart Store – It provides organized electronics deals helping users compare products easily while benefiting from updated and affordable pricing across categories daily online
Jamespaugh –
While going through peaceful informational platforms, I noticed this Elphin Bothy knowledge page and the site feels calm, informative, and very pleasant to browse through, offering content that is neatly arranged and easy to read.
StevenWholi –
Individuals interested in stylish clothing often browse online fashion platforms that emphasize modern aesthetics and carefully curated apparel collections designed for versatile wear Elegant Style Fashion Space – offering a curated selection of modern clothing that reflects aesthetic design principles and contemporary fashion trends while providing wearable pieces suitable for both casual and expressive personal styling choices
Melvinedime –
As I continued checking entertainment resources, I encountered this music showcase site and it felt pretty engaging, keeping me browsing for a while because the content was presented in a simple and appealing way.
EdwinCew –
Individuals who prefer energetic digital marketplaces often appreciate platforms that use trading post layouts to deliver dynamic browsing flows with varied product selections that improve user interaction and exploration Harbor Wave Commerce Flow Hub – featuring a structured shopping environment where trading post inspired visuals enhance product display and create a dynamic browsing experience that helps users navigate categories easily and enjoyably
DylanSoype –
During a quick search session, I noticed this useful link – It appeared to be an interesting platform, and browsing through it felt smooth, simple, and easy without complications.
Williamnab –
While going through various regional community platforms, I discovered this friendly town site and appreciated how it gives a comforting and welcoming impression, making it easy for newcomers to feel at home and well informed.
Davidquobe –
In discussions about online shopping usability, many users emphasize clear structure and intuitive flow when accessing platforms like CartArena Explorer Hub Shop – A cohesive design approach makes it easier to browse products and reduces friction during navigation across different sections.
Bobbyenvet –
During a comparative study of online marketplaces with smart purchasing features, I discovered that intelligent buying systems help users navigate efficiently and make quicker decisions, which became clear when exploring smart selection shopping hub – The platform provides smooth and simple navigation that enhances usability and overall browsing experience.
Tyronecrubs –
During a comparative study of digital marketplaces emphasizing deals and promotions, I discovered that structured pricing layouts significantly enhance shopping experience, which stood out when reviewing discount offers browsing hub – The deals section appears attractive, and prices are organized in a clear and reasonable manner.
RandomNamehiexy –
In reviewing vendor showcase websites focused on usability, I observed a platform built around Frozen Ridge Showcase Point that maintains a consistent visual hierarchy and smooth browsing behavior – the interface feels intuitive and helps users quickly access relevant product sections without distraction.
KevinKnips –
Ivermectin First: stromectol 3 mg price – Ivermectin First
Josephvew –
While reviewing ecommerce systems designed for modern cart optimization and user experience, I observed that polished layouts improve clarity and navigation flow, which was evident when testing modern cart experience portal – The interface feels minimal and sleek, offering a seamless shopping experience that is intuitive and smooth.
Michaelkep –
Many online shoppers prefer websites that create a friendly and simple browsing experience especially when they browse Meadow Outlet Cotton Shop – It feels like a comfortable online place where everything is easy to find and the browsing process is smooth and stress free.
RandomNamehiexy –
People looking for efficient online shopping experiences frequently prefer platforms that highlight stylish design and smooth navigation where ultimate urban shopping hub is featured in content and it highlights a system designed to improve usability while ensuring users can quickly discover products and enjoy a seamless and satisfying shopping experience overall.
StephenMic –
While exploring different online platforms earlier today, I came across check this page – The structure feels nice overall, giving a calm and tidy browsing experience that makes it easy to move through sections without feeling overwhelmed.
Donaldempiz –
Many users exploring digital shopping platforms prefer systems that constantly refresh deals and introduce new product opportunities where looping product deals portal is included in content highlighting dynamic retail environments – it supports a shopping experience where customers can always expect updated selections and changing promotions with each visit.
Williamevape –
In the process of exploring online project hubs, I came across this Elkhart project data page and project information seems structured, useful, and clearly presented overall today, with content that feels structured and easy to interpret.
StevenWholi –
Fashion focused users often seek brands that highlight clean aesthetics and modern clothing designs that can be styled easily for different occasions and personal looks Trendy Outfit Collection Hub – presenting a digital fashion destination offering stylish apparel and curated aesthetic collections that emphasize simplicity elegance and modern design appeal for individuals seeking fresh wardrobe inspiration
MichaelRiB –
During my review of digital group spaces, I came across this squad connection site and found it refreshing that it remains active and updated, suggesting a steady and engaged community presence.
Jimmytit –
People who enjoy structured online retail experiences often look for platforms that present products in merchant mart layouts with well defined categories for improved usability and browsing speed Canyon Goods Icicle Mart Space – providing a clean and organized shopping platform where products are grouped into categories using a merchant mart concept designed to enhance navigation and make online shopping more efficient and user friendly
ErniePah –
While exploring various community-focused platforms online, I came across this advocacy resource and it left a strong impression, as the content feels purposeful, thoughtfully structured, and clearly aimed at delivering meaningful information in a well-presented and accessible manner.
Matthewvef –
Самое интересное: https://tele-bot.ru
MichaelKense –
While checking out different platforms, I stumbled upon click here now – The arrangement of content is clear and logical, making it easy for users to explore and find what they are looking for without unnecessary hassle.
Curtismutle –
In the course of evaluating online shopping systems focused on price efficiency and savings opportunities, I found that affordable product hubs enhance usability by simplifying deal discovery, which became evident when analyzing affordable product browsing center – The pricing looks competitive and budget friendly, making shopping feel economical and practical.
Davidquobe –
Users frequently mention how important fast loading and clean design are when reviewing modern e-commerce sites including CleverCart Arena Web Store – Smooth transitions between pages and stable performance contribute to a reliable and enjoyable shopping experience overall for most users.
JesseCam –
While analyzing digital storefronts focused on reducing complexity, I found that streamlined cart functionality improves engagement when interacting with systems like minimal shopping basket – The design keeps everything simple, ensuring users can easily understand how to add, remove, and purchase items efficiently.
JamesOwero –
Online consumers searching for dependable shopping platforms often evaluate assortment and pricing and they may notice daily use products shop mentioned in comparisons – it highlights a collection of practical goods aimed at supporting routine household tasks and general lifestyle needs efficiently.
Michaelkep –
Many shoppers prefer platforms that offer stress free browsing and clean layouts especially when they visit Meadow Cotton Shop Outlet – The site feels welcoming and well structured making browsing easy comfortable and enjoyable for users exploring different products.
Andrewvop –
In discussions focused on improving online marketplace layouts, many experts mention that clearer categorization enhances usability, and the embedded element Market Explorer Suite helps present listings in a more intuitive structure, allowing users to find relevant vendors more efficiently overall experience.
RandomNamehiexy –
While exploring online tech stores focused on discounts and gadgets, I discovered a section labeled useful electronics browsing hub – The interface highlights interesting devices in a clean format, making it easy for users to find practical tech products and explore deals without confusion or clutter.
Billymiz –
While casually browsing through different platforms, I discovered go to this page – The design feels interesting overall, and everything is clear and not overwhelming at all, making browsing easy and pleasant.
DavidNut –
People who shop online regularly often choose websites that provide rapid browsing and diverse product listings where fast deal shopping center is featured in content and it highlights a system designed to improve browsing flow while ensuring users can quickly access products and complete purchases across all categories without unnecessary delays.
EstebanKax –
Online shoppers today often search for reliable platforms that update discounts frequently and help them compare offers efficiently across many product categories and seasonal promotions Daily Saver Hub One – The platform emphasizes consistent bargain updates, allowing users to discover fresh deals every day while browsing through a wide range of affordable online shopping options designed for convenience and speed
RandalEnami –
While checking conceptual insight resources online, I noticed philosophy reflection discussion hub and content feels reflective, detailed, and somewhat thought provoking overall tone, with structured ideas that encourage careful consideration and deeper thought. – It feels steady and reflective throughout.
StevenWholi –
Fashion enthusiasts exploring modern style often look for online brands that combine contemporary aesthetics with wearable clothing collections designed for everyday elegance and confidence in personal expression Modern Style Fashion Hub – offering a curated fashion platform featuring stylish apparel and aesthetic driven collections that reflect current trends while emphasizing individuality comfort and refined design for a modern lifestyle audience
OliverRix –
Many online shoppers prefer platforms that focus on trend updates and usability especially when they browse Trend Station Hub Digital It is a nice platform for trends where products feel updated and quite useful making the browsing experience smooth and efficient overall.
JosephWaG –
While going through entertainment and game platforms, I discovered this online singles experience game and it seems fun and unique compared to typical websites online, with a concept that feels creative and slightly unexpected.
BruceRindy –
People interested in creative retail experiences often enjoy platforms that elevate standard shopping into an artistic journey through thoughtful presentation and curated design aesthetics Goods Atelier Orchard Hub – featuring a visually refined online marketplace where products are arranged with artistic intention and creative design elements making the shopping experience feel more immersive and aesthetically pleasing
Raymondgum –
While browsing upscale accommodation listings, I noticed this elegant lodge site and the overall design gives a relaxing and luxurious impression that makes the property feel truly high-quality and welcoming.
Robertnique –
In the process of evaluating digital shopping environments focused on openness and category exploration, I found that open corner designs enhance usability and reduce confusion, which was clear when reviewing spacious browse experience center – The layout looks clean and open, allowing users to explore categories easily without visual pressure.
KevinKnips –
worldwide pharmacy online: foreign online pharmacy – reputable overseas online pharmacies
Blakejed –
Consumers who frequently shop online often look for platforms that connect them with trustworthy sellers in an organized environment where secure marketplace link hub appears in content – it reflects a system designed to enhance safety and usability while helping users quickly find products and complete purchases without unnecessary complications.
Pierrewat –
While conducting comparative research on ecommerce UX and cart optimization systems, I noticed that direct cart hubs improve conversion flow and clarity, which stood out when testing quick cart checkout center – The platform delivers a fast and clean checkout experience that feels smooth and easy to use.
RobertVag –
During a general search session, I came across explore the platform – The first look reveals a neat and modern layout that appears intuitive, helping users interact with the site in a simple and efficient way.
KevinExags –
E commerce design today emphasizes usability performance and intuitive navigation for better engagement CleverCart Online Corner Store – The browsing experience is simple and enjoyable Everything loads quickly and users can move between pages easily making the platform feel well optimized overall experience fully refined.
DonaldGek –
During evaluation of various online store systems for navigation quality, I came across a section labeled streamlined gate shopping view – The interface is clean and structured, ensuring users can browse products quickly and easily while maintaining a stress free experience throughout the entire shopping process.
Bryanemoks –
Shoppers frequently prefer e-commerce sites that combine usability and organized presentation especially when accessing Smart Cove Berry Goods Shop – I enjoyed checking it out because everything is nicely structured and the browsing experience feels simple and efficient overall.
RobertCoize –
Many marketplace evaluations highlight the importance of clean design, and Harbor Vendor Network – The platform maintains steady performance with fast loading content and logically grouped items that create a comfortable browsing environment for users exploring multiple categories at once.
Santosreift –
During a casual browsing session across various websites, I noticed visit this link – I like how everything is arranged, and it makes finding items effortless while keeping the browsing experience simple and easy to follow.
StevenWholi –
Fashion enthusiasts looking for stylish clothing often prefer brands that offer curated aesthetic collections reflecting modern trends and versatile design approaches Contemporary Wardrobe Fashion Hub – offering a curated fashion platform featuring modern clothing collections and aesthetic inspired designs that emphasize elegance versatility and comfort for individuals seeking refined and expressive personal style choices
Raymondblund –
In the middle of browsing event directories, I encountered this Edinburgh event listing page and event information looks lively, well organized, and easy to understand, with a presentation that feels clean and simple to navigate.
BrianNax –
People searching for practical shopping solutions often prefer platforms that offer clear layouts and quick buying options where affordable buy zone hub is featured in descriptions and it highlights a system designed to simplify browsing while ensuring users can easily find products and enjoy a seamless and efficient shopping experience overall.
ScottWholo –
Online users often prefer e-commerce websites that focus on speed and efficiency especially when they access Zone Dynamic Cart Market Shopping experience feels smooth and the cart system works really fast today allowing users to enjoy quick actions without unnecessary loading delays.
Michaelarora –
During my browsing of regional information sites, I discovered this destination info hub and found the content helpful, especially for someone new to this topic, making it easy to understand the area without prior knowledge.
EddieJanda –
During a comparative analysis of online marketplaces focused on visual clarity and usability, I discovered that fresh hub layouts improve browsing flow and comfort, which stood out when exploring easy fresh shopping index – The interface feels clean and modern, making browsing smooth, light, and simple for users.
Davidrorry –
While browsing through several design examples today, I stumbled across creative hub link and I have to say the presentation stands out nicely, with a refined layout and thoughtful color choices that make the entire experience feel smooth and visually engaging overall.
Davidskima –
People who value clarity in online shopping often seek platforms that use district inspired organization to simplify product discovery and enhance navigation flow Golden Cove District Product Hub – providing a structured shopping experience focused on goods district layout design that helps users browse efficiently while maintaining a visually clean and accessible interface
Jeffreysom –
Shoppers who value convenience often choose online stores that provide clear connections between buyers and sellers in one organized space where secure deal link hub is featured in guides – it emphasizes a marketplace designed to ensure safe transactions while offering easy navigation and quick access to various product listings for everyday shopping needs.
Matthewhix –
While reviewing ecommerce UX systems optimized for structured shopping and product clarity, I observed that organized marketplaces improve usability and reduce friction, which became clear when testing simple buying zone hub – The marketplace is well arranged, making product discovery smooth and straightforward.
MichaelVog –
While analyzing ecommerce platforms optimized for variety and centralized structure, I noticed that ultra hub models enhance usability by simplifying product access across categories, which stood out when reviewing smart ultra discovery hub – The platform feels modern and easy to use, offering many categories in one place that makes browsing intuitive and well organized.
GeorgeSmimi –
In modern online shopping environments users often prioritize clean interfaces and smooth flow especially when visiting Atelier Silk Ridge Goods The design is minimal and navigation feels smooth making the visit pleasant and allowing users to browse without distraction or complexity.
Richardfet –
During some light online research, I ran into view this link – The platform seems useful, and the content is presented in a clear manner that makes everything easy to understand at a glance.
StevenWholi –
People exploring modern apparel often seek fashion platforms that combine aesthetic inspired clothing with stylish and versatile wardrobe collections for daily wear Minimalist Style Clothing Hub – providing a curated selection of modern fashion pieces that reflect clean aesthetics contemporary design and wearable comfort designed for individuals who appreciate simple elegant and trend conscious wardrobe options
Ronaldcloky –
Across different studies of marketplace usability and consumer behavior online, experts often highlight interface simplicity, and Harbor Commerce Studio Exchange appears in conversations about efficient browsing frameworks – overall interaction feels straightforward with fast access to categorized listings that help users maintain focus while exploring various product options available.
RichardVip –
Modern shoppers often look for intuitive navigation and clean layouts when visiting platforms like ZoneCart Digital Store – The browsing experience is smooth, content is well structured, and users can quickly locate items without experiencing delays or visual clutter.
KevinAnego –
While reviewing multiple online resources, I stumbled upon explore here – The interface is smooth and well built, and it is easy to explore content while keeping navigation clear and user friendly throughout.
Leonardwab –
Online shoppers often seek platforms that feel simple yet functional, providing them with all necessary tools to browse and purchase without confusion or delays, and such a service is FlowNest Store – It is designed to maintain a balanced shopping environment where usability and product accessibility work together for a smoother experience.
Michalejuive –
While exploring advocacy and informational websites, I came across this Florida Can Do Better page and the website presents optimistic messaging, clear goals, and simple layout design, making the content feel approachable and easy to understand at a glance.
RaymondTat –
Online buyers who value affordability often look for platforms that highlight special offers and discounted collections where extra value cart center is included in descriptions and it highlights a system designed to improve usability while ensuring users can quickly find products and enjoy a seamless and cost effective shopping experience overall.
Jamestug –
Many users browsing digital marketplaces value strong deals and transparent pricing especially when they visit Center Dynamic Deal Hub Deals here are attractive and prices appear fair and competitive online helping users shop efficiently and feel confident about their purchase decisions.
KevinKnips –
ivermectin brand name: Ivermectin First – stromectol price
ShaneBlums –
During a comparative study of online retail systems focused on readability and clean interfaces, I discovered that core store layouts enhance user experience by reducing clutter, which stood out when analyzing clean listing shopping portal – The design appears simple and well structured, making product listings easy to read and understand without confusion.
LelandmUt –
In the process of browsing website portfolios, I came across this SpeazleBud landing page and I like the overall presentation, feels modern and straightforward, with a layout that feels fresh and easy to engage with.
Michaelbip –
While going through several informational pages earlier today, I came across this campaign resource and it stood out because the content is organized clearly, making it easy for readers to follow along and understand the message without confusion or unnecessary complexity.
WalterCow –
Online users searching for fast shopping solutions often gravitate toward platforms that reduce friction in purchasing and improve speed where seamless buy hub appears in content describing efficient systems – it emphasizes a user friendly environment where transactions are processed quickly and buyers can enjoy a smooth experience from start to finish without complications.
StevenMup –
During a comparative analysis of online retail systems centered around daily necessities, I discovered that structured stores enhance shopping efficiency and user satisfaction, which stood out when analyzing daily essentials shopping center – The site focuses on practical everyday items, all well categorized to make finding products simple and straightforward.
Williamsourl –
During a comparative study of online shopping platforms focused on choice based navigation, I found a page labeled flexible goods selection hub – The interface presents products in a structured yet adaptable way, allowing users to explore and choose items freely with a smooth browsing experience overall.
Lennyblign –
People who prefer clean digital marketplaces often appreciate commerce hub platforms that combine wide selection with smooth navigation for easier browsing and better usability Velvet Ridge Select Commerce Hub – providing a structured shopping environment where products are grouped in a hub system that enhances browsing flow and allows users to find items quickly and easily across categories
BrianUnfat –
Many shoppers appreciate platforms that combine organized structure with ease of use especially when they land on Raven Retail Grove Guild The design is interesting and simple making it quite user friendly and allowing smooth browsing through products and categories without unnecessary obstacles.
StevenWholi –
People who enjoy aesthetic fashion often look for curated clothing brands that combine modern design elements with stylish and versatile apparel collections Modern Style Apparel Hub – offering a fashion platform that features elegant clothing collections inspired by contemporary aesthetics and designed for individuals seeking comfortable stylish and expressive wardrobe options for everyday use
Ronaldimals –
During some general browsing, I noticed open this link – It offers fast loading pages, and the overall experience feels responsive and user friendly, keeping navigation clear and seamless.
Kevinsic –
Across many evaluations of vendor marketplace platforms, consistency in design and navigation is often cited as a major factor that enhances user trust and overall browsing satisfaction Stone Collective Harbor Experience – users find the platform easy to navigate, with clear structure and fast access to product information that supports efficient comparison and selection.
AlbertQuina –
While browsing through various online tools, I noticed visit this site – After trying it out, I found the navigation to be well-optimized and easy to use, with no issues while moving through different sections.
Charlesecorb –
In modern shopping environments, clarity and usability are essential factors, especially when users interact with Deal Discovery Station – The platform provides a seamless browsing experience with organized content and fast navigation that helps users efficiently locate relevant offers.
MatthewFrieP –
While checking fun commentary and humorous reflection sites, I came across fun commentary discovery page and the content feels relaxed and mildly comedic, offering a simple browsing experience that encourages curiosity without requiring too much attention or focus. – Feels like a quick, lighthearted internet stop.
Roberthen –
While analyzing ecommerce platforms designed for organized browsing and clear navigation paths, I observed that line-based layouts improve user experience significantly, which became evident when testing organized shopping line center – The structure feels clean and well arranged, allowing users to find products easily and without hassle.
PatrickNex –
People interested in browsing diverse inventories across multiple online categories frequently discover product variety directory placed within search pathways offering them a structured way to evaluate different product selections efficiently and clearly while shopping from various devices seamlessly anytime anywhere – Layout consistency improves user confidence during browsing.
Davidspult –
Shoppers who value convenience in online purchasing often look for platforms that make browsing simple and intuitive where quick global deal hub appears in guides and it reflects a structured system designed to improve usability while helping users quickly compare products and complete transactions without unnecessary delays or complications.
Oscarskity –
As I continued checking niche informational pages, I discovered this southwest coast details hub and it seems like a niche site but still quite informative overall, offering structured information that still feels practical and easy to understand.
Jasonspash –
Consumers interested in electronic add ons often look for online stores that provide organized deal sections and clear product listings where t affordable electronics hub point allows users to browse gadgets efficiently while ensuring access to budget friendly options and a smooth shopping journey across multiple categories of tech accessories.
Kennethnep –
In the process of exploring luxury product websites, I came across this stylish jewelry hub and it impressed me with its clean organization and sophisticated design that enhances the overall perception of the collection.
Davidfarne –
While evaluating modern ecommerce platforms focused on streamlined purchasing systems and user-friendly navigation, I noticed that direct buying flows significantly improve efficiency and reduce friction in shopping journeys, which became clear when exploring fast purchase flow hub – The platform offers a direct buying experience with straightforward navigation that feels clear, efficient, and easy to use from start to finish.
KevinKnips –
Vet Pharm First: online vet pharmacy – pet med
Sonnyanazy –
While reviewing online stores focused on fast performance design, I discovered a module titled quick access retail index – The platform ensures responsive interactions and fast page loads, creating an efficient browsing experience where users can explore products without unnecessary waiting or interruptions.
StevenWholi –
Individuals searching for fashion inspiration often turn to platforms that emphasize aesthetic clothing collections and modern design focused apparel for everyday wear Contemporary Aesthetic Wear Hub – offering a curated selection of stylish clothing that blends modern fashion trends with elegant simplicity and versatile wardrobe pieces designed for expressive personal styling and daily comfort
RobertFlelo –
Shoppers frequently appreciate platforms that deliver fast performance and clear layouts especially when visiting Drift Orchard Trading Hub Pages load fast and content is presented in an organized way making browsing simple efficient and enjoyable for users who want quick access to structured product information.
Dannywaync –
Shoppers who value clarity and elegance in online shopping often prefer platforms that use clean design principles combined with structured product organization inspired by atelier aesthetics Ridge Atelier Product Space – offering a sophisticated shopping environment where products are displayed with refined structure and elegant presentation helping users navigate listings easily while enjoying a visually balanced and professional online store experience
Stevesaurl –
While exploring several online options, I came across visit here now – It has a clean design style, and nothing feels cluttered while browsing through sections, which makes the experience smooth and clear.
BruceNek –
Digital shoppers often look for platforms that streamline the buying process while offering trustworthy product listings, and this is evident in SafeDock Marketplace – The service focuses on delivering a secure and easy shopping experience where users can explore a wide range of goods without worrying about complexity or unreliable information.
Gabrielattit –
As I continued checking film-related portfolios, I discovered this Folie a Deux cinematic page and film related content appears artistic, engaging, and thoughtfully presented style, with presentation that feels expressive and visually smooth.
Georgetic –
While reviewing ecommerce UX systems optimized for cart management and checkout experience, I observed that flexible cart structures enhance navigation and usability, which became clear when testing intuitive cart shopping center – The cart feels easy to customize, and the checkout process seems quick, clear, and straightforward.
ShawnNeoks –
In analyses of digital creativity tools, the balance between usability and inspiration is often highlighted as a key factor in successful platform design and user satisfaction Value Outlet Creative Hub – users enjoy a seamless browsing experience that supports both structured learning and open-ended exploration of innovative concepts and ideas.
Charlesfef –
Many digital shopping environments succeed when they reduce friction and improve usability, especially when users visit Goods Arena Efficient Store as it helps them browse smoothly and find relevant items without unnecessary delays or complications.
Edgardub –
As I continued reviewing various platforms, I found check this resource – The site is quite straightforward, and the browsing experience stayed easy and clear without any confusing or complicated structure.
AlbertPen –
People browsing for updated product collections frequently come across helpful pages featuring dynamic retail gateway which supports smooth navigation and allows users to explore different product types with greater ease while maintaining a clean and structured shopping environment online today easily
WillieShoda –
People who frequently shop online tend to prefer websites that focus on fast browsing and clear deal structures where quick shopping nest center is featured in guides and it highlights a system designed to simplify shopping while ensuring users can quickly discover products and enjoy a smooth checkout process across all categories.
Shanetut –
While going through web directories, I noticed this central UK info page and had a good first impression, as the content appears organized and useful, making the browsing experience feel smooth and straightforward overall.
Jaimetrast –
Online shoppers who value convenience often explore platforms that bring together diverse product categories in one place for smoother navigation and better accessibility online buyer center helping users quickly locate essential goods while comparing prices and features across multiple listings – It shows how centralized shopping hubs improve efficiency and reduce time spent searching for products.
Michaeltus –
In the process of checking various entrepreneurship guides, I discovered this clear advice resource and found that it delivers practical information in a way that feels relevant and easy to implement.
Anthonyter –
In the process of evaluating digital commerce platforms focused on structured browsing and clarity, I found that shopping hubs enhance usability and satisfaction, which became evident when reviewing clean browsing flow center – The platform is well designed, making it easy to move smoothly between different shopping sections.
StevenWholi –
Individuals passionate about modern fashion often explore websites that present curated clothing lines featuring aesthetic inspired designs and stylish wearable pieces Aesthetic Wardrobe Boutique – showcasing a fashion platform that highlights modern clothing collections focused on elegance simplicity and trend aligned designs created for individuals who value expressive yet minimal personal style choices
Byronlow –
During a comparative study of online retail platforms focused on layout optimization and usability, I discovered that stacked interfaces enhance browsing flow and make navigation more intuitive, which became evident when reviewing easy stack browsing portal – The marketplace design is structured for smooth scrolling, allowing users to find items quickly and easily.
Rogerbic –
Many shoppers prefer platforms that focus on clean design and usability especially when they visit Goods Frost District Seaside Hub The layout is neat and well structured making browsing easy comfortable and visually clear for users across all sections.
EduardoGof –
While reviewing ecommerce UX systems optimized for speed and responsiveness, I observed that quick cart layouts improve usability and reduce waiting time, which became clear when testing fast load cart portal – The interface responds instantly, making the shopping experience smooth, quick, and enjoyable.
ArronVon –
As I explored various websites, I came across learn more here – The site is well structured, and navigation feels natural and straightforward, which makes browsing smooth and comfortable from start to finish.
GeorgeSob –
While exploring sustainable fashion archives, I discovered Alexandra Tolstoy preloved edit and the collection appears thoughtfully assembled with a refined sense of style that makes browsing feel engaging and intentional for modern shoppers. – It gives a sophisticated yet approachable impression overall today.
Rickyvax –
People seeking practical online retail experiences often prefer platforms that present products in a structured and easy to navigate format for faster browsing and decision making Harbor Product Merchant Hub – providing a user friendly shopping platform focused on organized listings simple navigation and efficient browsing designed to make everyday product discovery and purchasing smooth and convenient for all users
KevinKnips –
Vet Pharm First: Vet Pharm First – Vet Pharm First
Robertdyday –
In competitive online retail spaces, users often choose platforms that offer intuitive navigation systems and fast loading pages for a better shopping experience Goods Express Station – Streamlined design helps shoppers quickly move through categories and access relevant items while maintaining clarity and reducing unnecessary effort during browsing sessions overall.
JesusDag –
Online shoppers searching for curated product listings often come across Curated picks space which organizes items thoughtfully and allows users to explore selections more efficiently while maintaining a visually clean layout that improves overall shopping experience – emphasizes structured and helpful browsing.
DavidroP –
When exploring online spaces designed for innovation and conceptual thinking, simplicity and clarity often determine how effectively users can generate and refine ideas Outlet Inspiration Workshop – the interface feels welcoming and easy to use, allowing users to move through creative resources without disruption or unnecessary complexity in navigation.
Briangauro –
People who shop online regularly often choose websites that offer updated promotions and clear product layouts where easy open deal center is featured in content and it highlights a system designed to improve browsing flow while ensuring users can quickly access products and complete purchases smoothly across all available categories.
BillyCom –
While navigating through various online resources, I encountered see more here – The platform feels clean and easy to use, with a simple structure that allows quick understanding of the layout and content.
Robertlog –
Many consumers exploring digital shopping platforms tend to value systems that provide verified safety and efficient support where reliable shopping assistance hub is featured in descriptions and it reflects a structured marketplace focused on ensuring secure purchases and offering helpful customer service for all users across different product categories.
StevenSap –
While going through supportive message websites, I discovered this inspirational support page and really like the message behind this, feels genuine and supportive, with a tone that feels warm and encouraging throughout the content.
StevenWholi –
Individuals interested in trendy clothing often explore online fashion platforms that highlight aesthetic inspired designs and modern wardrobe essentials Fashion Aesthetic Collection Space – presenting a curated selection of stylish apparel focused on modern design trends aesthetic appeal and wearable comfort for individuals who value creativity simplicity and elegant fashion expression
EdwinPak –
During a comparative review of online shopping platforms with structured navigation systems, I observed a section labeled easy navigation port hub – The interface is clean and minimal, ensuring users can browse products effortlessly while maintaining clarity and simplicity across all categories.
DavidFause –
While evaluating modern ecommerce platforms focused on optimized cart systems and streamlined checkout processes, I noticed that efficient cart solutions greatly improve user experience and transaction flow, which became clear when exploring fast cart solutions hub – The cart system feels highly efficient, making both browsing and checkout smooth, simple, and well optimized for users.
RandomNamehiexy –
Many shoppers appreciate platforms that focus on usability and clarity especially when they access Market Harbor Birch Network The structure is very organized and I like how it makes exploring convenient while ensuring a smooth and pleasant browsing experience overall.
HaroldFrunk –
Many online retail platforms focus on providing streamlined access to products, especially for users who prefer quick navigation, and one such platform is built to support organized browsing while ensuring that users can move between categories with ease and clarity Smart Deck Storefront built to support organized browsing while ensuring that users can move between categories with ease and clarity – It delivers a user-centered experience designed for efficiency and simplicity in shopping
StephenSpisa –
As I explored different retreat and travel accommodation websites, I noticed this scenic Fisherman’s Retreat listing and the location feels peaceful, scenic, and ideal for relaxing stays experience, with surroundings that appear calm, natural, and very inviting for guests.
JamesDaf –
Shoppers who value curated digital marketplaces often prefer websites that use boutique hall inspired layouts to present products in a clean organized and visually appealing way Glade Boutique Hall Showcase – featuring a refined e commerce environment that focuses on simplicity and curated product displays designed to make browsing easy efficient and enjoyable for users across different shopping categories
Bobbyapelf –
In competitive e-commerce environments, usability and visual balance play a major role in user satisfaction, especially when accessing CleverZone Product Space where categories are arranged clearly, allowing visitors to move smoothly through listings without feeling overwhelmed or distracted by unnecessary design complexity.
Richardner –
When reviewing vendor-focused digital platforms, usability experts often emphasize how consistent layouts and logical grouping improve browsing efficiency in systems like Hazel Vendor Atelier Depot – Smooth browsing experience, products are clearly displayed and accessible, providing users with a smooth interaction flow that reduces confusion and enhances overall shopping satisfaction during exploration.
Aaronbop –
During a casual search across different online resources, I noticed visit this link – It stands out for its tidy presentation, where each section feels properly aligned and contributes to an overall well-organized and appealing experience.
Arthurber –
While going through different informational campaign pages, I discovered this Simpsons-themed resource page and this looks meaningful and worth spending some time exploring, with content that seems organized in a way that invites further attention.
Thomasmof –
In the process of evaluating digital shopping platforms with emphasis on structured navigation models, I found that smart hub approaches improve usability by guiding users through clear browsing paths, which was evident when reviewing smart commerce discovery portal – The platform feels well organized and efficient, making shopping simple and structured while helping users navigate products without unnecessary effort.
DustinVak –
During usability testing of digital shopping systems focused on simplicity and clarity, I discovered that minimal cart structures improve satisfaction and ease of navigation, which became evident when exploring simple order experience hub – The design is clean and straightforward, making shopping easy and free from any confusion.
KevinKnips –
stromectol uk: ivermectin oral solution – Ivermectin First
AlvinSof –
While exploring different online shopping platforms today, I came across this quick market portal and found several interesting products listed, making the browsing experience feel fast, smooth, and conveniently easy for everyday shopping needs without unnecessary complications.
RodneyRep –
In modern online shopping environments users often prioritize usability and fast access especially when visiting Commerce Cove Marble Portal Hub The interface is simple and it works really well for quick browsing making it easy to move through different sections without confusion.
BartonDic –
Individuals who prefer simple and efficient online stores often appreciate platforms that use merchant lane setups where products are clearly sectioned for better navigation and smoother browsing flow Maple Merchant Coast Lane Hub – featuring a well organized e commerce platform where products are arranged using a merchant lane concept designed to improve usability and create a more structured and visually clear shopping experience for users
Jeremypax –
Many online shoppers appreciate websites that combine speed, clarity, and aesthetic balance when exploring new marketplaces, especially when they open Style Trend Hub – The browsing experience remains fluid and visually attractive, making it easy for users to stay engaged while moving through different product areas without unnecessary distractions.
Jameslon –
While evaluating modern ecommerce platforms focused on intelligent structure and efficient product organization, I noticed that smart marketplace setups significantly improve browsing efficiency and category discovery, which became clear when exploring intelligent shopping hub – The marketplace is smartly structured, with products well categorized and easy to locate, making the overall browsing experience smooth and efficient.
JamesMat –
In studies focusing on digital retail interface improvements and customer journey mapping across e-commerce systems Honey Cove Digital Bazaar Hub experts note that well structured browsing environments significantly enhance decision making – users benefit from clean organization and fast access to relevant listings.
Rickytab –
During an analysis of ecommerce platforms emphasizing user friendly environments, I discovered a category titled nest style retail portal – The interface creates a cozy browsing atmosphere where products are displayed in a gentle and organized way that helps users explore items without feeling rushed or overwhelmed.
mostbet_jrPr –
мостбет скачать на айфон [url=https://www.mostbet76480.help]мостбет скачать на айфон[/url]
Georgelib –
Users exploring digital marketplaces frequently appreciate well structured layouts and easy navigation especially when visiting Collective HarborStone Vendor Center The experience felt smooth and nothing was confusing while navigating which made it simple to explore products and sections without difficulty.
AntonioRot –
Shoppers often choose websites that provide a balance between product variety and ease of navigation, ensuring a better overall experience, and one such example is ValuePoint Store – It supports quick browsing and organized product categories that allow users to make faster and more confident purchasing decisions in their daily shopping routines
KevinKnips –
us pharmacy no prescription: Online Pharm First – top online pharmacy
JamesBof –
While going through different online pages, I stopped at check this page and checked it out today, finding the structure neat and the navigation experience straightforward and user-friendly overall.
EdwinCew –
Shoppers who value interactive online marketplaces often prefer platforms that use trading post layouts to provide dynamic browsing experiences with diverse product selections that improve shopping engagement Harbor Wave Market Flow Hub – offering a structured shopping environment where trading post inspiration enhances product variety and creates a dynamic browsing experience that supports easy navigation and efficient discovery across categories
Georgesearf –
While analyzing ecommerce platforms optimized for promotions and affordability, I noticed that deal corners enhance user experience by clearly highlighting savings opportunities, which stood out when exploring best savings shopping hub – The deals look attractive and well organized, giving the impression of a platform that is genuinely good for saving money while shopping.
Randymit –
Online shoppers often prefer platforms that provide clarity and intuitive structure for better navigation, particularly when accessing Trend Corner Flow Market – The website design supports easy browsing and helps users discover trending products quickly while keeping the experience smooth and visually balanced overall.
WalterNut –
During my search for helpful e-commerce directories and small business showcases online, I encountered a platform that stood out, especially when I reached Visit vendor marketplace portal which appeared to consolidate vendor information in a way that supports easy navigation through categories product highlights and seller profiles for better decision-making – it gave me a general impression of being a practical browsing tool for discovering independent sellers
RandomNamehiexy –
HoneyCoveVendorStudio – Clean interface, everything loads fast and works very smoothly.
DennisMit –
In reviewing several outlet themed online resources, I came across a page that felt structured and easy to navigate Hollow Creek landing page which gives users a clear path through sections and categories – The overall experience is simple and user friendly for browsing
JesseMop –
While browsing charity event directories, I noticed karting for support initiative and interesting concept overall, seems well organized and quite engaging today, offering a clean and easy to follow layout that connects motorsport activities with a humanitarian purpose. – The tone feels clear and impactful.
Normancal –
During evaluation of promotional listing websites, I came across promo listing explorer which simplifies deal discovery – this shopnetmarket.shop platform enhances search functionality, enabling users to quickly scan offers and compare options while maintaining a clean and easy-to-use browsing environment for everyday shopping needs.
StanleySmalp –
While conducting usability research on ecommerce systems emphasizing global cart functionality and international product access, I noticed that unified cart structures improve navigation and convenience, which became evident when analyzing international shopping cart portal – The platform presents a global cart style system with a wide range of online products available for easy browsing.
JamesBof –
As I explored different online sources, I came upon discover more here and noticed the content felt organized and easy to navigate, making the browsing experience simple and quite enjoyable overall.
WalterNut –
While exploring niche e-commerce communities and independent seller platforms, I encountered a reference to Elm Harbor curated shop hub which seems to compile vendor listings and product showcases in one accessible place enabling users to browse and compare offerings efficiently – I found it reasonably helpful for discovering curated products
Brucesen –
Individuals who enjoy relaxing online shopping experiences often prefer websites that combine lakefront aesthetics with market lounge design to create a peaceful browsing environment that feels easy and enjoyable Velvet Lounge Lakefront Goods Hub – featuring a structured shopping platform where products are displayed with calming lakefront inspired visuals designed to improve browsing comfort and provide a smooth and visually balanced online shopping experience
Philiptex –
While comparing online marketplaces designed for smooth user experience, I discovered smart deal cart corner which focuses on accessible product listings and fast browsing – Hyper Cart Corner provides a really easy shopping experience with affordable products and fast delivery, ensuring shoppers can quickly find what they need without unnecessary complexity or clutter in navigation.
ByronPef –
In modern e-commerce environments, users often prioritize clean design and intuitive navigation that improves usability, especially when visiting MartTrend Smart Shop – Everything feels logically arranged, making the shopping journey smooth, efficient, and visually clear across all pages and product categories on the site.
RandomNamehiexy –
When examining online retail platforms built for enhanced usability and optimized browsing workflows across diverse digital product ecosystems and vendor listings Trading Foundry Icicle Link feedback indicates high satisfaction – Overall experience remains simple and effective with fast navigation clear interface structure and well organized product displays supporting effortless comparison and exploration of available items.
KevinKnips –
worldwide pharmacy: medicine online – reliable online pharmacy
ConnieTam –
Online users appreciate neon styled shopping centers that offer smooth navigation and a wide selection of useful products for simple browsing Neon Cart Prime Hub Explorer improving experience – The platform is frequently noted for its organized structure and user friendly shopping flow
RobbyWrile –
Many shoppers prefer platforms that provide premium goods corners with solid product collections and smooth browsing and clean layouts for seamless navigation Premium Goods Market Flow Corner making usability better – The platform is known for its structured categories and fast browsing system
Robertthype –
Digital retail users often prioritize platforms that combine affordability with speed and reliable customer service for everyday purchasing needs online QuickEdge Savings Portal – This service focuses on delivering cost effective deals and fast processing times that improve overall user satisfaction during shopping activities.
Normancal –
While comparing e-commerce browsing platforms, I encountered efficient bargain browser that improves product discovery – this shopnetmarket.shop service offers structured navigation, enabling users to explore deals more effectively and make quicker decisions without being slowed down by overly complex or cluttered interface elements during shopping.
Stevenmon –
Users exploring digital marketplaces frequently value organized layouts and polished design especially when visiting Goods Forest Cove Atelier Hub The platform looks tidy and professional creating a clean impression that supports easy navigation and comfortable browsing through different product categories.
Glennkek –
Users often rely on structured e-commerce systems like rapid goods zones offering fast shopping zone with simple layout and useful product range, ensuring a smoother browsing experience that reduces friction and improves overall product discovery speed QuickBrowse Rapid Goods Zone Center – Designed with clarity and performance in mind, it enhances user flow and supports efficient product selection
DennisMit –
While checking different online directories for outlet-style content, I found a page that looked minimal and easy to navigate Hollow Creek showcase link which helps users focus on categories without distraction – The interface feels clean and user oriented at all times here online
Simonsouri –
In the process of evaluating digital marketplaces focused on modern cart usability and design clarity, I found that corner layouts improve engagement and reduce friction, which became evident when reviewing modern shopping flow hub – The design appears minimal and well structured, making the shopping experience easy and user friendly.
WilliamGon –
Digital shoppers appreciate platforms that emphasize clarity and structured product presentation style Online Style Bazaar – Clear organization of products allows users to navigate effortlessly while discovering items that match their preferences and maintaining an enjoyable browsing experience across all categories
HollisSof –
People exploring online discounts often value websites that prioritize clarity trust and consistent updates to available offers Value savings outlet ensuring they always have access to the latest price reductions across multiple shopping categories – A dependable source for finding meaningful discounts without unnecessary complications or misleading listings
Basiljep –
During a review of independent seller platforms and digital storefront aggregators, I encountered a link leading to Ember Guild commerce directory hub which appears to centralize multiple vendor listings, and my impression after checking it was that the layout is clean and easy to interpret – overall usability felt solid and simple
Justinwaymn –
When assessing digital storefront ecosystems built for scalability and improved user engagement, reviewers highlight clarity in interface structure and browsing efficiency Cove Icicle Product Studio overall design supports smooth navigation, with accessible product sections and organized categories that make searching and comparing items straightforward for users navigating through the platform.
PatrickBow –
Many online shoppers today prefer websites that offer clean structure and fast loading pages which improve usability during browsing sessions, particularly when they access CrystalHub Shopping Zone – Everything feels easy to understand and dependable, allowing users to find products quickly without unnecessary distractions or complicated navigation steps.
Miguelzex –
As I was going through several online pages out of curiosity, I found explore here and it seemed to contain useful information, which made me consider revisiting it again later for a deeper and more careful look.
RichardHetty –
Обновлено сегодня: https://alexstroy.su
KennethDiz –
Online consumers frequently choose platforms that provide curated picks with quick browsing so they can discover products without confusion or delay Neon Pick Easy Flow Hub enhancing experience – The website is often recognized for its structured layout and fast loading system
Robertheaby –
Последние публикации: https://stritstroy.ru
Henryfem –
In modern online shopping environments users often expect clarity and ease of navigation especially when visiting Forest Cove Market Atelier Everything is easy to find and the structure feels intuitive making browsing simple and efficient while allowing users to explore content without unnecessary complexity.
Jesuskip –
People who enjoy comparing different online deals often seek platforms that present information in an organized manner, and this link is one such example discount insight hub – it is structured to make browsing promotions easier, giving users a straightforward way to identify useful savings opportunities.
LouisNes –
Many buyers appreciate rapid style corner platforms featuring stylish items available here with quick browsing and smooth interface, ensuring smooth access to fashion products and a streamlined shopping journey ClearStyle Corner Flow Hub – Focuses on structured categories and efficient product display
Williamdoora –
During analysis of online retail systems focused on variety and user convenience, I discovered that all-in-one stores enhance usability by simplifying product access, which became clear when testing broad selection shopping hub – The platform provides a wide range of items, making browsing across categories smooth and efficient.
Lloydbem –
During a general scan of various e-commerce and outlet-style websites, I discovered a platform that seemed particularly well organized, with clear navigation menus, structured categories, and a layout that supports quick browsing without unnecessary complexity for everyday users Hollow Ridge online shop entry which loads quickly and keeps navigation simple and intuitive – Overall it delivers a smooth user experience that prioritizes clarity over decoration, making it easy for visitors to locate content without distraction or confusion.
RandomNamehiexy –
Users interacting with online stores often prefer fast and clear navigation systems that allow effortless movement between sections and product listings without disruption where Browse Cart Arena – this design supports efficient exploration by maintaining consistency across pages and helping users stay oriented during their shopping journey
KevinKnips –
Ivermectin First: buy stromectol – Ivermectin First
Darrelldeevy –
People browsing e commerce websites often look for clarity and smooth transitions between pages to improve their overall shopping experience and efficiency Global Goods Shelf – It is commonly seen as a platform that organizes products in a neat and accessible format making browsing more comfortable for everyday users
PatrickRal –
During a casual review of commerce listing platforms and small business directories I encountered a reference that led to Ivory Cove marketplace discovery page which was organized within a curated index and after briefly checking it I noticed the structure was minimal and clear – overall it felt like a useful platform and I enjoyed moving through its easy-to-read sections
MatthewPrusa –
While reviewing different websites, I stopped at learn more here and found the platform to be solid, with relevant content that was neatly arranged and easy to navigate overall.
BrandonCar –
Across multiple user experience reports on online retail platforms and marketplace design Isle Commerce Foundry Link – Diverse product catalog is arranged clearly, allowing users to navigate efficiently and discover items quickly across well structured categories.
DavidCEata –
Users exploring shopping platforms often prioritize structured layouts and fast performance especially when they visit Digital Arena Cart Hub – The browsing flow is smooth and intuitive helping users move between categories easily while enjoying a clean and efficient interface overall.
WillieQualo –
Online consumers frequently enjoy marketplaces that combine trendy product offerings with a simple interface design for a more seamless browsing experience Neon Style Bazaar Explorer Hub making browsing easier – The website is often noted for its modern layout and clear product organization that simplifies shopping
Petereneft –
While conducting usability evaluations of ecommerce platforms focused on layout structure, I noticed that stacked systems improve clarity by grouping products efficiently, which stood out when exploring efficient stack browsing hub – The design feels organized and structured, allowing users to browse items clearly and comfortably.
Davidlauth –
E-commerce platforms continue evolving toward more inclusive product systems that bring together multiple categories into a single efficient shopping destination UnifiedRange Commerce Hub – This structure ensures users can access a wide variety of products in one place while enjoying a seamless and convenient online shopping journey.
Albertlax –
Many online shoppers prefer websites that prioritize simplicity and elegant structure especially when they browse Gallery Jasper Harbor Trading The platform feels polished and carefully designed making browsing smooth easy and enjoyable while maintaining a clean and professional visual layout throughout.
CarmenGeock –
Online users appreciate rapid trend hubs that feature trend hub offering fresh items and easy navigation for users, allowing them to quickly explore trending items without confusion or delays FlowCart Rapid Trend Hub Portal – Designed for optimized browsing and responsive shopping experience
Wayneenuch –
In reviewing online shopping interfaces focused on simplicity, I discovered simple deals hub which structures product listings clearly – Simple shopping experience with clear layout and easy product access improves navigation flow by presenting items in an organized manner that helps users compare options quickly without being overwhelmed by unnecessary details.
Charleshut –
Users exploring e-commerce platforms often value simplicity and organized layouts that reduce confusion CartZone Express Market delivers smooth browsing with logical structure while helping customers locate products quickly through improved category segmentation and responsive interface design overall experience for users.
WalterArida –
Online buyers often look for platforms that balance functionality and simplicity while still offering a wide range of everyday useful items across multiple categories for convenience Product Station Point – The shopping experience is often considered efficient and smooth, allowing users to move from selection to checkout without complications or confusing navigation steps slowing them down
DanielRam –
While analyzing different online shopping platforms and their design approaches, I found a site that emphasized simplicity and clarity in its structure which made browsing feel natural and easy without unnecessary distractions or visual overload Honey Fern browsing store serving as a central access point for product categories and listings – The interface feels smooth and user friendly, offering a comfortable experience for everyday browsing activities.
Chrisbup –
During a casual scan of online commerce aggregators and artisan storefront directories I discovered a reference leading to Ivory Ridge vendor catalog portal which was embedded within a structured index page and after reviewing it briefly I found the navigation intuitive – overall it felt smooth and everything was clearly organized for easy browsing
RandomNamehiexy –
IvoryBrookVendorFoundry – Clean design, shopping feels smooth and very easy today.
MilfordMic –
While exploring different online resources, I landed on take a look and found some interesting bits of information that made the browsing session mildly useful and worth a quick look today.
DavidhiX –
While analyzing ecommerce platforms designed for digital and tech-savvy audiences, I observed that modern shopping points enhance usability through organized presentation of gadgets and tools, which became evident when testing digital product discovery hub – The site feels sleek and modern, showcasing tech-focused items that appear appealing and relevant to today’s users.
LouisTwige –
Online consumers frequently prefer platforms that gather modern trends and updated product selections in one central place so they can shop efficiently every day Neon Style Trend Explorer Hub making browsing smoother – The website is often noted for its structured design and visually appealing layout that simplifies shopping
HermanAbums –
Online users often appreciate platforms that combine usability with clean design especially when visiting Digital Cart Explorer Hub – Cart browsing feels efficient and well organized with products displayed clearly helping users enjoy a smooth and stress free shopping experience overall.
BrianSwOrN –
While browsing through various websites during my free time, I came across take a look at this site – Everything is laid out in a structured way, and the navigation feels simple and very user friendly.
Jasonexpef –
Users exploring vendor marketplaces frequently value fluid navigation and quick response times especially when visiting Flora Ridge Craft Vendor Hub The experience is smooth and pages transition without delay making browsing easy and comfortable across all sections of the website.
Edgarpneug –
Many shoppers appreciate rapid trend outlets that provide outlet deals on trending products with simple and clean structure, making online shopping more organized, efficient, and easy to manage FlowCart Trend Outlet Shopping Portal – Focuses on structured browsing and seamless checkout flow
PatrickCix –
Shoppers expect online systems that are fast, reliable, and easy to navigate during busy browsing sessions in digital commerce today Cart Express Link built for clarity – this service enhances efficiency by simplifying navigation and ensuring smooth transitions between product pages
KevinKnips –
ivermectin 1: Ivermectin First – generic stromectol
melbet_crMt –
melbet чат киргизия [url=http://melbet74825.help/]melbet чат киргизия[/url]
RubenEmowS –
Shoppers frequently value digital marketplaces that provide fast navigation tools and logically arranged product sections for smoother exploration experience StyleCart Vision Zone – the browsing environment emphasizes clarity and efficiency while helping users move easily between categories and discover relevant products with minimal effort required.
BruceDaync –
Digital shoppers often look for online stores that provide fast navigation and a wide range of products in a well structured and easy to understand format Product Zone Navigator making browsing more enjoyable and efficient when searching for everyday essentials – The platform is appreciated for its organized categories that simplify the overall shopping process
mostbet_xiOL –
mostbet maxfiylik siyosati [url=http://mostbet91372.help]http://mostbet91372.help[/url]
Thomasfab –
During my exploration of online retail directories and small business marketplaces I encountered Ember Brook curated marketplace hub which brings together vendor listings and product categories in a centralized browsing space – I found it moderately helpful for general browsing and discovery
Michaelreums –
In the process of reviewing different online retail catalogs, I encountered a platform that emphasized usability and clean design, helping users find what they need quickly through well-organized sections, including a href=”[https://indigoharborstore.shop/](https://indigoharborstore.shop/)” />Harbor Indigo shopping portal placed naturally within the content layout – The browsing experience is steady and efficient, with a layout that avoids clutter and keeps focus on product discovery.
MickeyNop –
While analyzing ecommerce UX designs centered on navigation consistency and usability, I observed that flow-based systems reduce friction and improve browsing flow, which was evident when reviewing smart browsing flow center – The design provides smooth transitions between sections, helping users explore products without confusion or delays.
JamesGrify –
In studies of e commerce usability experts emphasize the importance of simplified navigation and well structured content presentation for better engagement Icicle Cove Retail Space users find it easy to locate items and move between sections seamlessly without any difficulty today
JeffreyInaro –
Modern consumers expect digital stores to be responsive, well organized, and capable of delivering personalized shopping experiences across all devices efficiently always available Online Wave Mart reflects the growing trend of adaptive retail systems that respond to user preferences – Wave market brings fresh goods and intuitive navigation features that enhance usability and improve overall shopping satisfaction for users
Walterjoige –
Online shoppers who enjoy vibrant digital spaces often prefer platforms that showcase fresh items in an exciting trend zone with a clean and easy browsing layout for better discovery Neon Trend Explorer Zone Hub making browsing more enjoyable – The platform is often appreciated for its colorful neon inspired design and well structured categories that help users quickly find new and trending products
Jamespaild –
In e-commerce browsing experiences users often expect readable structure and clean formatting especially when accessing Commerce Hazel Cove Atelier The content is well presented making it comfortable to read through and allowing users to navigate smoothly without unnecessary distraction or confusion.
JimmyNAH –
Many users prefer digital shopping platforms that reduce effort and improve navigation clarity especially when interacting with Cart Center Smart Shop – The centralized layout makes browsing simple allowing users to handle cart options smoothly without feeling overwhelmed or distracted during their session.
CarltonHon –
Users benefit from platforms that provide instant access to trending items and simplified browsing structures for quick decision making needs Instant Trend Access Hub Direct – allowing faster engagement with new collections and smoother navigation across product categories effortlessly in a clean interface design flow system
Harryslole –
While comparing online marketplace websites, I noticed a platform that focused on simplicity and variety with a structured and easy to navigate layout BuyZone market product view positioned within the page flow – The site provides a wide selection of goods and ensures a smooth browsing experience without unnecessary distractions or delays.
RobertSopsy –
Users exploring e commerce websites often prioritize ease of use and well structured product listings Infinity Shop Navigator helping them locate items quickly and proceed through checkout smoothly – It is appreciated for its fast browsing experience and simple checkout process
FrankWhile –
Modern savings plazas bring together a variety of discounted products and promotional events making online shopping more efficient and enjoyable for users Modern Savings Plaza It serves as a centralized destination for finding ongoing deals and seasonal discounts helping customers shop smarter while exploring a wide range of categories conveniently
Keithfaurl –
During research into digital commerce hubs and independent marketplace directories I found Honey Cove vendor listing board which arranged shop information in a minimal and structured layout – overall the presentation was clear and made it easy to follow while casually browsing through different sections
MatthewOvele –
While testing different websites for usability, I stumbled upon click here now – The simple design works well, with pages loading quickly and maintaining a clean interface.
Willieclutt –
In the course of reviewing digital marketplaces for UX efficiency, I discovered a section called branch navigation shopping portal – The tree inspired structure allows users to move through categories logically, improving clarity and making product browsing smooth and easy to understand across all levels.
KevinKnips –
online pharmacy no rx: buy drugs online – online pharmacy without scripts
Phillipbiomy –
In reviewing different online retail templates I found a design that stood out due to its simplicity and clarity focus Inked Meadow catalog hub Inked Meadow catalog hub The browsing experience is smooth and intuitive allowing users to quickly access different categories and find relevant items without any confusion or unnecessary steps overall flow
Billyfax –
When analyzing modern online shopping experiences, usability and clarity are often considered key factors that influence satisfaction, especially when platforms are designed for quick browsing and comparison, and in this case Ivory Corner Trading Space users benefit from a straightforward interface that keeps navigation smooth and ensures product information is easy to access without unnecessary complexity or confusion.
MiguelTEX –
Many users appreciate platforms where cart systems are optimized for speed and clarity, ensuring a seamless checkout experience without unnecessary complexity Royal Cart Smooth Flow Hub – offering intuitive browsing structure, fast-loading pages, and a clean interface that enhances overall shopping satisfaction and usability across all devices
Garrettdyego –
Shoppers frequently appreciate websites that reduce visual noise and complexity especially when they visit Foundry Icicle Trading Brook The simplicity is clear and nothing feels cluttered which makes browsing feel relaxed and straightforward across all sections of the platform.
AnthonyJonse –
Many digital shoppers appreciate platforms that serve as reliable cart stations with smooth checkout systems and organized shopping flow for efficiency Next Cart Express Hub Station making shopping easier – It is frequently noted for its clean layout and fast loading cart system
Rolandjepsy –
Consumers who value time saving solutions often prefer stores that simplify browsing by grouping commonly used products into easy to access sections daily use marketplace – It is beneficial because it helps users complete everyday purchases efficiently while maintaining clarity and reducing unnecessary complexity in product selection
mostbet_abKn –
мостбет mines [url=http://mostbet73481.help/]мостбет mines[/url]
Calvinembob –
Many digital shoppers value platforms that offer simplicity and clarity in cart design especially when they land on CartZone Browse Market – The simple interface enhances usability and supports a smooth shopping flow making browsing easy and efficient across all sections.
Diegolesty –
Many digital buyers prefer websites that combine convenience with a wide selection of everyday products so they can complete purchases without difficulty CartFlow Navigator giving them a smoother browsing journey across different categories – The platform is generally noted for its well arranged layout that helps users move quickly between items and discover useful goods efficiently
Ronaldinink –
Shoppers interested in chic and modern styles often look for discount depots that combine fashion forward designs with affordable pricing and easy navigation features Chic Discount Depot It offers a curated collection of stylish products at reduced prices making it simple for users to upgrade their wardrobe and lifestyle without overspending unnecessarily
Jamesapeta –
While exploring curated digital storefront directories and vendor networks I came across Honey Cove vendor exhibit page which appeared in a grouped listing section and after checking it briefly I found the interface simple – overall it seemed like a decent platform and the browsing experience felt clear and minimally complex
RandomNamehiexy –
While evaluating ecommerce UX designs centered on cart usability and checkout optimization, I noticed that smart cart corners improve conversion efficiency by simplifying purchase flow, which stood out when exploring smart order cart portal – The design feels practical and user friendly, with a checkout flow that is smooth, simple, and easy to complete.
JamesHok –
As I explored various online platforms, I came upon discover more here and gave it a quick look, finding the interface clean and user friendly, with content arranged in a simple and accessible way.
Brianexatt –
During an extended review of fashion oriented ecommerce websites and boutique storefront designs I encountered a layout that felt modern and well organized Shop Iron Hollow collection which helped create an easy browsing flow with clearly separated categories and a calm visual hierarchy supporting quick product discovery without confusion
Jamesvence –
During general browsing activity, I noticed open this site – The straightforward layout makes it easy to find what you need across the pages.
JamesLaw –
Consumers interested in unified shopping platforms can explore experiences where Unified Shopping Hub appears within the browsing system, helping users access a wide variety of products in one place, with organized categories, simplified navigation tools, and a seamless interface designed to enhance convenience and reduce time spent searching for essential items online.
Jeffreyamofs –
In studies of vendor-based e-commerce systems prioritizing structured layouts, user engagement, and fast interaction response times, Foundry Brook Market Deck is noted since fast loading pages ensure shopping feels smooth, efficient, and very reliable across all stages of browsing and product comparison.
PatrickKah –
Users appreciate deal websites that maintain clean layouts and smooth navigation systems, helping them quickly locate the best offers available online Elegant Royal Deal Navigator Hub – providing intuitive browsing structure, organized promotional listings, and seamless interaction flow for a better online shopping experience across all platforms
RalphHax –
шкаф шкафы-заказать.рф
Virgilsen –
Users exploring modern shopping platforms often value speed and clarity in browsing systems that improve overall usability especially when they visit Orchard Merchant Mart Hub Pages load fast and content is displayed in a clear way making navigation simple intuitive and comfortable for users who want a smooth browsing experience without unnecessary delays or confusion while exploring products online.
Kennethbub –
Many digital users enjoy platforms that offer next generation buy hub experiences featuring smart deals and broad product variety for easy exploration Next Gen Buy Vision Hub Flow enhancing usability – The website is often appreciated for its clean interface and efficient browsing system
MonroeAgile –
Many users today search for reliable shopping platforms that provide consistent performance and a pleasant browsing experience across devices Online Deal Gateway – The system emphasizes accessibility and responsiveness, making it easier for customers to find what they need quickly and efficiently
Ramirowes –
шкафы купе по индивидуальным размерам современные шкафы на заказ
Jamesblage –
Users browsing digital trend platforms often appreciate structured layouts and simple navigation systems especially on Smart Trend Digital Corner – The trend section feels well arranged and browsing is smooth making it easy for users to move through content without unnecessary effort or confusion.
KevinKnips –
online pharmacy: no script pharmacy – worldwide pharmacy online
Cedricreamp –
Many digital buyers prefer websites that focus on showcasing discounts clearly so they can take advantage of limited time offers without confusion or delay Seasonal Saver Portal allowing them to browse deals efficiently and make faster purchasing decisions – The site is often recognized for its organized structure and regularly refreshed promotional sections that highlight active discounts
Robertnut –
Users who enjoy discovering limited time offers prefer platforms that highlight urgency and variety while keeping navigation simple and visually clean for better engagement Hot Offers Junction – This adaptation presents a junction of trending offers where shoppers can quickly access time sensitive deals presented in a streamlined format that enhances browsing speed and clarity
Darrenlop –
During my review of digital commerce hubs and small business marketplace ecosystems I encountered Ember Cove curated vendor listing portal which organizes various storefronts into categorized sections and I found the site performance quite responsive while the textual content remained clear and legible throughout – it worked well for simple exploration tasks
Richardzew –
In the course of reviewing ecommerce browsing systems, I discovered a section called axis flow product portal – The platform uses a logical arrangement of items that improves navigation and helps users browse efficiently without confusion or unnecessary design distractions across pages.
Robertalels –
I was casually browsing for something new and came across check this cool collection – Honestly, the variety here feels thoughtfully selected, and the pricing doesn’t seem over the top, which makes it quite appealing for someone exploring options online nowadays.
SamuelIllub –
Users frequently prefer well designed marketplaces that allow smooth exploration of quality goods with clear categories and fast navigation systems Royal Goods Experience Flow Arena – offering simplified browsing structure, efficient product discovery tools, and a user friendly interface that enhances online shopping satisfaction and clarity
Haroldchodo –
Shoppers often prefer digital stores that provide stable performance and clear navigation paths during product searches and purchases Seamless Cart Space ensuring users can browse comfortably while experiencing fast and reliable system responses throughout their session – The platform prioritizes simplicity and consistency for improved user engagement
Georgejab –
While scanning through various digital marketplace websites I encountered a platform that offered a clean and organized browsing experience Iron Leaf market showcase located centrally within the layout and providing easy access to product categories – The overall structure feels intuitive and user focused allowing smooth transitions between sections and clear understanding of available content
Edgargautt –
In studies focusing on e commerce usability improvements, experts frequently note that minimalistic interface design and logical category grouping help users locate products quickly without feeling overwhelmed by excessive visual clutter or complexity Cove Atelier Product Space – The experience is smooth and well organized, enabling efficient browsing and easy access to all product sections.
Jerryskymn –
Shoppers frequently appreciate websites that offer clean interface design and consistent functionality especially when they visit Cove Commerce Fern Atelier The platform feels well maintained and reliable providing a smooth browsing experience that is easy to follow and enjoyable across all product sections.
Michaelsox –
Shoppers today often look for digital marketplaces that simplify product discovery by organizing items into clear and easy to navigate sections Smart Goods Browser Hub making online shopping more efficient and less time consuming – The platform is recognized for its straightforward interface and smooth category transitions
ErnestFus –
As I explored different online sites, I reached open this resource and found it quite helpful, with a simple and pleasant interface that made navigation smooth and easy.
Williammuh –
In e-commerce browsing experiences users often prioritize simplicity and usability especially when accessing Smart Digital Deal Zone – The platform ensures intuitive navigation and smooth deal browsing that allows users to find offers quickly while maintaining a clean and efficient layout throughout.
Ernestbob –
People who enjoy unique shopping experiences often prefer platforms that present products in visually appealing and well organized categories for easier discovery Creative Goods Arena – It is portrayed as a creative shopping space where stylish items are displayed in an engaging structure helping users browse efficiently and find interesting products effortlessly
JamesJer –
During a general review of digital commerce listings and curated storefront networks I came across Flora Brook vendor discovery hub which appeared organized with clearly separated categories and readable formatting across pages – my impression was that it provided some interesting insights while casually navigating different vendor sections
Eugenerog –
I came across several stores before landing on click here to see – The shop has a smooth and simple browsing flow, and the items seem curated in a way that makes exploration feel natural and easy.
KevinKnips –
top online pharmacy: Online Pharm First – legitimate online pharmacy
Jamessig –
Consumers value digital marketplaces that maintain transparency, consistency, and dependable order management systems Transparent Order Reliability Zone – The system prioritizes honest product representation and stable service delivery to ensure customer trust and satisfaction.
Peterintap –
Digital shoppers prefer stations that provide clear updates and structured browsing systems, ensuring easy navigation and better product discovery overall Royal Goods Station Flow Hub – offering simplified interface design, fast loading pages, and efficient browsing tools that enhance the overall online shopping experience significantly
Thomascex –
Many digital business owners look for efficient tools to manage their stores, and I encountered e-shop configuration suite designed to streamline setup processes – it supports customization, improves backend usability, and helps ensure that online storefronts remain easy to manage while still offering advanced functionality for growing business demands.
CharlesAttix –
People browsing online marketplaces often prioritize websites that maintain updated catalogs and structured navigation systems for easier product discovery across categories Quick Browse Station Hub improving efficiency – The platform is known for its consistent updates and well arranged listings that support smooth and intuitive shopping experiences
KevinSouff –
During usability testing of digital retail platforms focused on navigation efficiency, I discovered that route-based design helps users explore products more naturally by providing structured browsing paths, which became evident when reviewing smart route navigation hub – The system feels clear and intuitive, making it easy for users to find products while maintaining smooth and logical navigation flow.
Floydsnado –
In modern online shopping environments users often prefer clean design and structured navigation especially when visiting Fern Vendor Cove Hub The layout is simple and I did not have trouble finding anything important while exploring different categories and vendor listings across the platform.
AlfredjoynC –
Across usability research on online shopping platforms, consistent design structure and predictable navigation are frequently identified as key factors in improving customer experience and retention rates Harbor Trading Showcase Hub – The selection is neatly arranged, allowing users to browse comfortably and understand categories at a glance.
RandomNamehiexy –
While reviewing several digital shop designs, I found a website that delivered both speed and aesthetic consistency across all pages Iron Petal retail page placed within the content area – The overall browsing experience is fluid and visually appealing, making product exploration straightforward.
Keithnex –
Minimalist shopping platforms are often preferred by users who want clean layouts and quick access to product categories without unnecessary visual clutter or slow loading elements interfering with navigation Minimal Style Goods Center – The minimal style center emphasizes simplicity and speed, offering fast loading pages and a structured catalog that helps users browse efficiently and comfortably
Stevenchato –
During a general scan of curated marketplace hubs and digital storefront systems I encountered Flora Brook commerce discovery index which grouped vendor listings in an orderly way making browsing easy – I found useful insights while casually navigating through the platform’s content
JordanGearm –
Online users often prefer e-commerce websites that reduce complexity and improve clarity especially when they access Digital Goods Smart Corner – The product listings are clean and organized allowing users to browse easily and complete shopping tasks without confusion or delay.
mostbet_ewst –
mostbet последняя версия apk [url=www.mostbet71852.help]mostbet последняя версия apk[/url]
RandellPEn –
Users who prefer organized online shopping experiences often look for platforms that offer fast navigation and clean product layouts Premium Goods Station Organized Hub Flow – The system delivers a simple interface that helps users browse categories efficiently and comfortably easily
AustinRoaxy –
While comparing different shopping websites, I stumbled upon visit this shopping spot – The store looks quite promising overall, with a variety of items available and pricing that appears to be balanced and sensible.
KennethCic –
Digital users often prefer trend platforms that provide simple layouts and fast access to classy items, improving overall browsing experience quality Smart Elegant Trend Corner Hub – focused on structured product listings, smooth navigation flow, and enhanced usability that makes online shopping more efficient and enjoyable for everyone
Phillipkiz –
Bargain focused users often rely on digital platforms that aggregate discounts and streamline the shopping experience for faster and more effective purchasing decisions Deal Rush Center – It is designed to accelerate deal discovery and provide users with a seamless interface that supports quick browsing and efficient access to valuable savings opportunities
DavidiNges –
Online shoppers frequently look for platforms that combine attractive design with simple navigation to explore trending items without effort Infinity Trend Flow Center improving experience – It is widely recognized for its smooth browsing system and visually appealing interface that supports easy shopping
JamesUphop –
During a light browsing session online, I visited click to view and found it to be a nice site overall, with clearly presented information and smooth page loading that made browsing simple and efficient.
Michealnig –
Shoppers frequently prefer websites that offer simplicity and structured spacing especially when accessing Brook Forest Foundry Trading Hub The design feels comfortable and well arranged allowing users to browse smoothly and focus on content without unnecessary clutter.
KevinKnips –
legitimate online pharmacy: Online Pharm First – online pharmacy no prescription
AlbertoGrany –
When evaluating modern online shopping platforms designed for accessibility and clarity, reviewers consistently note that structured product presentation improves usability significantly Brook Market Jewel Gallery – The experience remains very smooth overall, allowing users to browse comfortably and explore items without unnecessary complexity or confusion.
DonaldMit –
While passing time online and opening random pages, I reached visit daisystone link and had a quick look where everything appeared neat and easy today, creating a clear and pleasant browsing flow.
Stephentak –
Online visitors often prefer carefully organized websites that display products in a visually pleasing and structured manner Curated Style Spot the spot delivers curated styling options with clean browsing features helping users locate desirable items efficiently and comfortably across multiple categories
StevenGeord –
In the process of analyzing ecommerce outlet platforms, I came across a website that prioritized clarity and performance with a simple navigation system Petal Iron online outlet access placed within the content flow – The experience feels organized and stable, allowing users to browse without distractions while enjoying fast and responsive page interactions throughout.
Robertsargy –
Many online shoppers today prefer websites that offer simple navigation and fast performance especially when accessing PickMarket Smart Center – The interface is organized and intuitive making it easy for users to pick items quickly without confusion or unnecessary effort during browsing.
Stephentient –
I was exploring a few shopping websites when I noticed take a look here – The layout appears user-friendly and helps in navigating through different sections quickly, making it convenient to discover items without unnecessary effort.
JasonDic –
Online shoppers often prefer platforms that highlight curated picks since they reduce confusion and help users quickly locate relevant and useful products Premium Pick Market Curated Flow Hub – The interface is structured to support fast browsing and clear product discovery for a better shopping experience overall
JasonLib –
Many users appreciate shopping hubs that combine royal elegance with modern updates, ensuring a simple browsing journey with clearly arranged categories Royal Trend Flow Experience Center – providing intuitive navigation, clean layout design, and seamless browsing that enhances daily product discovery and overall user satisfaction significantly
EnriqueGEw –
Modern e-commerce trends highlight the importance of reducing friction in online shopping by offering simplified interfaces and well structured product categories for better usability CleanCart Simple Hub – It provides a minimal and user focused shopping experience designed to help customers navigate easily and complete purchases without confusion or unnecessary complexity
HoraceKam –
While analyzing digital marketplaces centered on promotions and reduced pricing, I encountered a section called deal explorer discount center – The layout highlights attractive discounts and structured product listings, making it easy for users to find value based items and explore further without confusion or unnecessary browsing complexity.
Andrewpievy –
In researching e-commerce browsing tools and product listing platforms, I encountered deals tree browser which structures deals into categorized sections for easier access – Shop tree market provides organized categories for shoppers and improves user experience by offering a clean interface that allows quicker comparison of products across multiple sections without confusion.
JustinJar –
People exploring online stores frequently prefer websites that provide instant updates on trending products so they can shop more effectively Fast Style Update Hub enhancing user satisfaction – The website is often described as user friendly with a focus on speed and organized browsing
CharlesDub –
I was casually browsing online when I found shop link here and it stood out for its simplicity – Browsing here felt smooth overall, and the products look nicely arranged, making the whole experience easy and pleasant.
RichardDef –
Users exploring online marketplaces frequently enjoy when product listings feel fresh and visually interesting, encouraging longer browsing sessions and return visits, particularly on copperpetal market access – browsing felt satisfying since items appeared intriguing and gave a reason to check the site again in the future.
Cecilhax –
Many users browsing digital stores value clear organization and simple navigation especially when they visit Orchard Granite Guild Market Hub The presentation feels solid and well structured making browsing easy and comfortable across all product listings and categories.
Douglassew –
While exploring different web pages, I came across discover creek store and noticed the presentation was simple and effective; I left a quick note – overall it gave a well organized browsing experience that felt smooth and readable.
Walterdut –
Online consumers often value premium styled platforms that balance aesthetics with efficient transaction systems ensuring smooth shopping from start to finish Premium Goods Post – This post style structure focuses on delivering high quality product listings with a simplified checkout process designed for user convenience
SidneyTalge –
While passing time browsing through websites, I came across cool shopping spot and it looked clean and inviting right away – The entire setup makes it feel like an effortless and pleasant place to spend a little time exploring.
Curtissmota –
During a casual search for new stores, I encountered explore more here – The site feels well-arranged and the pages load fast, making the overall browsing experience quite enjoyable.
WilliampeN –
Users exploring modern trend-based platforms often value clean structure and easy navigation that improves browsing efficiency especially when they visit Digital Trend Corner Hub – The trend section is well structured making browsing feel smooth and intuitive while helping users discover content without confusion or delay.
KevinKnips –
stromectol 0.5 mg: Ivermectin First – buy liquid ivermectin
Henryjuh –
Many shoppers appreciate premium pick zones that offer a nice variety of picks and fast loading product pages for a smoother and more enjoyable experience Premium Pick Zone Organized Flow Hub – The website structure supports fast navigation and easy access to all product categories
DavidNup –
Digital users value stations that simplify premium trend exploration with modern layouts and fast navigation tools for efficient shopping experiences Smart Royal Trend Display Flow Station Portal – providing structured product listings, intuitive browsing flow, and clean interface design that improves usability and customer experience overall
RichardDef –
Visitors to online marketplaces often note that interesting product variety plays a key role in keeping browsing sessions engaging and enjoyable, as seen on petal copper shop link – items were appealing and made the experience feel worthwhile, encouraging another visit to explore the catalog more thoroughly in the future.
Brianpem –
Many digital shoppers appreciate the idea of marketplaces that feel like serene valleys filled with artisan goods, offering a browsing experience that emphasizes calm discovery and visual harmony hollow echo marketplace link – It suggests a peaceful e-commerce environment where rustic-inspired products are arranged thoughtfully to create a relaxing and immersive shopping journey.
Williamlap –
People exploring trendy household product platforms frequently enjoy websites that highlight both innovation and simplicity in how items are presented and described Trendy Home Goods – it showcases stylish and functional products in a way that helps users quickly understand how each item enhances modern living spaces effectively
Shawnzep –
People exploring luxury products online often prefer platforms that organize high quality items in a visually appealing and simple layout Elite Luxury Goods Hub making browsing efficient – It is commonly noted for its stylish presentation and easy to navigate structure
VincentPet –
While checking various sites during my free time, I encountered check this page and noticed the content seemed fresh and presented in a very readable format.
CharlesDub –
While checking out different online stores, I came upon take a look and it gave a calm impression – The browsing experience felt smooth and easy, with products nicely arranged in a clean and simple layout.
Westondiado –
People checking new online stores often mention how important first impressions are when browsing modern websites for shopping and discovery purposes urban flash corner overview layout and navigation both feel clean and intuitive overall, making browsing experience pleasant and easy to return to again later
Travismuh –
During exploration of curated commerce galleries and online vendor showcase pages I encountered a structured reference leading to Moon Cove creative gallery hub which appeared within a grouped index and after checking it briefly I noticed the interface was clean and organized – overall it felt engaging and worth returning to in the future for updates
CraigSesty –
Users who frequently shop online prefer platforms that keep navigation intuitive and product categories easy to understand for better browsing efficiency Simple Goods Zone – It ensures that stylish items are arranged in a logical way allowing users to explore different sections without confusion or delay
NathanObliz –
During a casual browsing session, I discovered check out this page – The site looks reliable, and the product details are presented in a clear and informative way, which makes browsing feel more straightforward.
RandomNamehiexy –
ironwavecollective.shop – Collective platform looks solid, easy access and well structured pages
Jameshof –
While browsing for general shopping platforms, GoldenBay online product hub delivers a simple yet effective interface, helping users browse through items smoothly while maintaining an overall pleasant and well structured shopping experience.
Jamesrip –
Нужна стальная лента? лента бандажная нержавеющая широкий ассортимент, разные толщины и марки стали. Выгодные цены, быстрая отгрузка и поставки для производства и строительства
Brucesof –
During a comparative review of online shopping platforms emphasizing cart performance, I discovered a module titled speedy checkout cart portal – The interface provides quick response times and seamless transitions, making it easy for users to move through product selection and cart actions without any noticeable lag.
RichardDef –
Many visitors to digital shops appreciate when the variety of items creates a sense of discovery that makes browsing more enjoyable, especially on copper petal showcase hub – the experience felt engaging because products seemed interesting and made the platform feel worth exploring again later.
Michaelgroup –
Many shoppers enjoy platforms that focus on practical goods with clean design and efficient navigation, making online shopping more comfortable and quick Savvy Smart Practical Goods Station Portal – designed for streamlined browsing, structured interface design, and improved product discovery that enhances overall shopping satisfaction
SidneyTalge –
While exploring online content, I ended up visiting check store now and it gave off a relaxed impression – The navigation feels smooth and the overall experience is quite enjoyable for casual browsing sessions.
AnthonyChear –
Shoppers today rely on digital marketplaces that can combine speed, convenience, and variety to enhance their overall purchasing experience Ultra Fast Deals Portal – This portal specializes in extremely quick access to promotional offers and deals designed for users who prioritize speed and efficiency in online shopping
AnthonywaW –
Many users appreciate shopping platforms that prioritize speed and clarity while ensuring smooth transitions between product pages and checkout sections Quick Order Bridge – It connects browsing and purchasing stages seamlessly, allowing customers to complete orders quickly without encountering delays or confusing interface elements
Stephenkethy –
Many online users enjoy platforms that make buying simple through modern interfaces and fast browsing tools for a more efficient shopping experience Modern Cart Ease Point supporting smooth browsing – It is often noted for its clean layout and quick access to products across categories
Aurelioplado –
Online visitors often enjoy marketplaces that balance visual simplicity with product variety, especially when browsing natural or handmade collections in a calm environment echo meadow shopping portal – It reflects a fresh, nature-themed digital store that emphasizes ease of use, open design, and a relaxing browsing experience for users seeking wellness-focused goods.
Merlealuff –
As I navigated through different online sources, I encountered go to this link and found it to be a solid site overall, with clearly arranged information that made everything easy to follow and understand quickly.
Jerryfielp –
During a relaxed browsing session, I found see shop page and it immediately felt easy to navigate – The layout is clean and the design is simple, making everything easy to explore in a calm and enjoyable way.
KevinKnips –
stromectol 3 mg tablets price: buy stromectol pills – ivermectin tablets
Westondiado –
Online users frequently appreciate when websites feel updated and visually consistent because it improves trust and encourages continued exploration of available content urban flash corner fresh view the interface appears clean and well arranged which creates a positive browsing experience that feels both modern and easy to use
TeodoroTUT –
Users who frequently browse online stores tend to prefer platforms that organize picks into categories while maintaining fast loading speeds and simple navigation Daily Picks Corner – It provides regularly updated curated items in a structured layout that supports quick browsing and easy exploration
DanielVibia –
I was going through various shopping websites when I discovered explore this page now – The browsing experience feels easy and pleasant, with simple navigation and fast page loading that makes everything run smoothly.
RichardDef –
Digital shoppers often highlight that engaging product selections make browsing more enjoyable and increase the likelihood of returning to a site, as seen on petal copper goods hub – the experience felt worthwhile since items looked appealing and made the platform feel like a place worth revisiting.
AnthonyDiz –
Many users appreciate platforms that focus on smart cart management, ensuring a clean and efficient shopping flow that reduces confusion during checkout and improves overall usability Smart Arena Cart Control Center – designed for smooth cart handling, structured browsing, and efficient checkout flow that enhances shopping convenience and user satisfaction significantly
Jackieboype –
During research into online retail environments, I found a well structured marketplace particularly when accessing Cove premium goods archive which offers clear categorization and easy navigation – The browsing experience feels polished and efficient supporting users in quickly locating items of interest
Jamesamect –
Online consumers frequently look for platforms that offer smooth cart systems enabling easy addition, removal, and management of items during shopping CartEase Builder Hub helping users stay organized – The website is known for its practical layout and efficient checkout process that reduces friction during online purchases
Anthonynor –
While analyzing e-commerce solutions designed for budget-conscious users, I found affordable cart explorer that presents discounted items in a structured layout – Value market hub focuses on affordable items and easy navigation, making it easier for users to browse efficiently and compare products without unnecessary complexity or clutter in the shopping interface.
Chriskib –
During a routine browsing session, I checked out check it out and found the overall structure to be clear and easy to follow, making the experience feel comfortable and efficient.
JasonDit –
Many digital users enjoy platforms that function as premium trend marts offering useful items and simple user experience for convenient and efficient online shopping across multiple categories Premium Trend Flow Mart Access – The website is known for its structured design and easy navigation system that helps users browse trending products without confusion
Merlegeori –
While exploring artisan marketplace platforms and small vendor directories I came across FloraBrook shop exploration portal which offered neatly arranged listings and easy-to-read product sections – overall I found useful insights while casually navigating through different areas of the site
Charlesasync –
Many users enjoy browsing e-commerce sites that feel inspired by flowers and natural beauty, offering a refreshing experience when exploring artisan gifts and decorative collections echo petal craft market – The concept suggests a floral-themed bazaar where products are arranged with delicate aesthetics and vibrant charm to create a soothing browsing journey.
DarrellDowly –
As I browsed through several websites earlier, I came across open pine shop and it stood out with clarity – The collection here seems fresh and thoughtfully curated for shoppers, creating a simple and enjoyable browsing experience overall.
Davidtag –
Online visitors often favor platforms that combine modern aesthetics with practical navigation when exploring trending products and ideas Aesthetic Trend Zone – The zone blends visual appeal with usability, allowing users to browse stylish products comfortably
Arthurothex –
Shoppers typically value websites that present products clearly while maintaining a stylish and modern interface you can explore stylish product gallery which organizes fashion items in a visually structured manner that makes browsing enjoyable and efficient – The platform offers a seamless experience with well designed pages and intuitive navigation features.
GlennTroub –
During my search for online stores with interesting offers, I stumbled upon explore this bargain site – The range of products stood out to me, and it seems worth checking out for anyone looking for good value deals.
Kennethwib –
As I explored more online content, I came across see products and it immediately felt neat and thoughtfully arranged – The curated selection gives the site a unique vibe, making browsing feel both pleasant and engaging from start to finish.
RichardDef –
Many people exploring digital stores tend to value platforms where products feel thoughtfully arranged and visually appealing for casual browsing, especially on copper petal goods site – the browsing experience felt enjoyable because the selection appeared engaging and gave a reason to return and explore more items later on.
DavidFoela –
In the course of reviewing digital commerce platforms with emphasis on cart reliability and system responsiveness, I found that clean design and consistent performance greatly improve usability, especially in product heavy stores, which was apparent when analyzing fast reliable cart – The experience feels steady and well structured, allowing users to manage their cart easily while maintaining smooth and dependable browsing behavior.
Robertcic –
Online shoppers often prefer curated marketplaces where smart choices are organized into clear categories, making everyday browsing easier and more efficient across a wide range of practical products for daily needs Smart Choice Variety Bazaar Hub – offering structured navigation, clean layout design, and well organized product selections that help users discover useful items quickly and comfortably
WilliamKen –
sildenafil online buy Viagra over the counter Cheap Sildenafil 100mg
Enriquebemen –
While analyzing e-commerce tools focused on improving catalog access, I found a streamlined shopping interface easy selection guide that allows users to explore multiple categories without confusion and improves browsing clarity – Quick online market supports fast product visibility and offers structured listings that help users save time while searching for relevant online deals and shopping opportunities.
AlbertBrign –
In the course of reviewing online informational platforms I discovered a resource that seems relevant for structured browsing and content exploration Quartz Orchard landing resource which provides categorized sections and navigation support that help users find and explore content in a straightforward manner – It feels organized and approachable for general browsing.
Josephtib –
Online shoppers frequently choose websites that showcase trending items in a structured and visually appealing way for better browsing efficiency Smart Arena Trend Hub making shopping easier – The platform is known for its modern design and user friendly navigation system
Ralphpeact –
Online users seeking modern retail solutions can visit Modern Basket Market which organizes products into a clean and user friendly structure – this helps simplify browsing and allows shoppers to enjoy a more efficient experience while exploring a wide variety of goods available across different categories.
RobertOxize –
People who enjoy fashion and lifestyle shopping often prefer platforms that highlight trends while keeping navigation straightforward and easy to understand Fashion Trend Corner Spot – The spot focuses on presenting trendy items clearly, enabling users to browse comfortably and discover new ideas quickly
RobertBully –
Digital shoppers frequently prefer websites that evoke forest imagery and natural simplicity, especially when browsing artisan products and sustainable lifestyle goods echopine nature goods hub – This suggests a pinewood-inspired collective space where products are designed and displayed with eco-conscious values and a calm, nature-focused presentation style.
Bernardhon –
While checking out different online stores, I came upon take a look and it gave a calm impression – The browsing experience was quite pleasant, with appealing items that were easy to view and explore without any hassle.
LeighRic –
Many online shoppers today look for reliable platforms that combine ease of browsing with fast delivery options and secure payments while exploring Golden Crest Shop official portal various categories including fashion electronics and home essentials making the experience more enjoyable and efficient for everyday users – This kind of layout typically improves customer satisfaction because visitors can move between pages without confusion and complete purchases with fewer interruptions or delays
EdwardThili –
Many shoppers appreciate premium trend zones providing stylish trending products with clear and easy layouts for faster and easier navigation Premium Trend Clean Zone Flow Hub – The website offers minimal design and efficient browsing tools for smooth experience
HarryCiple –
I had been exploring multiple shopping websites when I came across see what’s here – It appears to be a decent shop with trendy items, and the pricing looks fair enough to attract casual online shoppers.
RandomNamehiexy –
While checking out different online stores I found urban selection hub which had a clean layout and allowed effortless browsing across categories making the experience pleasant – overall it was a good platform with some interesting and slightly unusual items available.
RichardDef –
Digital shoppers often highlight that engaging product selections make browsing more enjoyable and increase the likelihood of returning to a site, as seen on petal copper goods hub – the experience felt worthwhile since items looked appealing and made the platform feel like a place worth revisiting.
Harryimith –
Many digital shoppers value platforms that reduce complexity while increasing deal visibility, a concept reflected in Smart Deal House Express – delivering structured promotional listings, simplified navigation layers, and practical discount discovery tools that enhance overall shopping efficiency today online.
Leonardwhady –
I spent a bit of time browsing different pages and came across see this shop which had a neat and simple layout – I found a few interesting items that made it feel like a place worth recommending to others.
JimmyOvaky –
During some casual online browsing, I discovered view this site and found the information useful, so I saved it for future reference and easy access in the future.
Kennynat –
As I navigated through different online sources, I encountered go to this link and found it to be a pretty decent platform, where I enjoyed scrolling through well-arranged sections that felt clear and user-friendly.
EdwinSoype –
Online buyers frequently prefer centralized websites that provide access to trending items and popular ideas in an organized browsing environment Trend Market Center Hub making shopping smoother – It is appreciated for its structured design and easy access to product categories
Rodrigoked –
Users who prioritize efficiency in online shopping tend to prefer platforms that reduce clutter and provide streamlined access to product listings Modern Cart Hub – The website enhances user experience by organizing products in a logical structure, making browsing both quick and straightforward for all visitors
Manuellup –
Shoppers seeking inspiration and variety often prefer platforms that gather stylish trends and updated products into one cohesive browsing experience Ultimate Trend Hub – This final hub provides a comprehensive selection of modern items presented in an intuitive and engaging layout
RichardDef –
Many online users appreciate stores where the product variety feels appealing enough to make them consider returning later for another look, especially on copper petal browse store – browsing was enjoyable because items seemed interesting and left a positive impression that encouraged future visits.
GeorgeDef –
While searching for new shopping options, I encountered browse this platform – The user interface feels clean and smooth, allowing quick product discovery without confusion or complicated navigation steps.
Floydgex –
Online users often value marketplaces that combine coastal inspiration with minimalist presentation, offering a peaceful browsing experience across curated product categories and lifestyle items frostbay serene shop view – This reflects a winter-themed collective brand where goods are displayed in a soft, cool aesthetic that enhances clarity and user comfort during browsing.
WilliamKen –
Viagra online price Cheap generic Viagra Cheap Sildenafil 100mg
Jamesher –
During my online browsing time, I stumbled upon browse spruce items and it felt easy to use – The goods variety is nice and everything looks well presented and organized in a smooth and simple layout.
Cecilmug –
While analyzing ecommerce systems designed for improved browsing structure and category flow, I observed that choice hubs simplify navigation and improve product discovery, especially when users explore multiple sections, which was clear when testing easy browse variety center – The interface provides a wide selection of products and allows seamless switching between categories for a more intuitive shopping experience.
ThomasHit –
People searching for an efficient online shopping experience often value platforms that reduce complexity while still offering a wide range of accessible products online catalog hub – The browsing flow feels intuitive and smooth, helping users move through pages effortlessly while discovering items that match their needs and preferences.
RobertNep –
Many digital buyers prefer platforms like prime value corners that provide good value deals with practical and affordable choices for smoother and more efficient online shopping experiences Prime Value Flow Corner Access – The website is known for its clean layout and responsive browsing system that allows users to explore products with ease
BrendoncaX –
Many shoppers prefer online stores that deliver consistent performance and easy navigation across all product categories, Goldendrift online store entry allowing them to explore different sections without encountering slow loading pages or confusing layouts. This consistency is often seen as a key factor in building long term user trust
Travisgrize –
Many digital shoppers prefer platforms that guide them toward useful items efficiently, and Smart Corner Easy Discovery Hub – offers organized product selections, fast navigation tools, and a clean interface designed to enhance browsing clarity and simplify purchasing decisions online.
Davidsef –
During exploration of niche marketplace platforms and curated vendor systems I encountered Fernstone listing board which compiles multiple storefront entries, and after browsing briefly I found the structure clear and easy to navigate – overall it felt straightforward and minimal
Davidflold –
Many users prefer online stores that function as a station for new trending products updated regularly to improve shopping convenience Trend Finder Station Hub making discovery simple – The website is often appreciated for its structured layout and frequent content updates
Jamestiets –
E-commerce users frequently seek websites that showcase clothing deals while keeping the overall interface lightweight and easy to navigate on mobile devices Trend Cart Access this platform highlights curated fashion offers and ensures a smooth checkout process that supports quick decision making for busy online shoppers
TerenceErani –
The evolution of online shopping has led to more dynamic platforms like Dynamic Goods Outlet where users can access a broad selection of everyday essentials – These modern systems are built to support fast interaction, reliable product discovery, and simplified interfaces that help improve the overall customer experience while reducing the time needed to find suitable items.
RichardDef –
Many online visitors appreciate when product displays are interesting enough to maintain attention and encourage future visits to the platform, especially on copper petal digital hub – the experience was pleasant since items seemed appealing and made the site feel worth revisiting for more exploration.
Davidtrife –
During my search for shopping platforms, I stumbled upon check this out now – The site appears quite interesting, and the product images are clear and appealing, making it easier to explore items visually.
HenryHaw –
Shoppers who prioritize efficiency in online shopping tend to choose platforms that organize items clearly and allow fast transitions between categories Organized Speed Corner – The platform combines structure with speed to deliver a better browsing experience
DennisBax –
While casually browsing online shops, I discovered check items here and it felt clean and structured – I really liked the overall feel, and browsing was quick and easy today, making everything easy and enjoyable to browse.
RicardoKep –
Many shoppers prefer online platforms that feel grounded in nature and winter imagery, making browsing more engaging when exploring rustic crafts and seasonal decorative items frost crest alpine goods view – It reflects a strong mountain-themed brand identity where curated products are displayed with a cool, structured, and visually appealing layout.
Edwardjaf –
I was casually going through a few online stores when I discovered shop link now and it stood out with its layout – The collection feels current and stylish, and the navigation was quick and smooth, making it enjoyable to explore.
RobertSes –
Many users prefer digital stores that keep things organized and allow them to quickly locate what they need urban pick zone web store – clear structure and simple navigation contribute to a better shopping experience and help reduce time spent searching for products overall online journey
JeraldEmene –
Online consumers frequently rely on quality buy worlds that provide a wide range of quality products making shopping simple and reliable for satisfaction Quality Buy World Market Flow Hub – The website is structured for easy product discovery and browsing
Robertdef –
Online shoppers often explore curated platforms that highlight modern product styles in an organized way, and this experience is reflected in Smart Trend Discovery Arena Hub – a structured marketplace designed to present updated items, smooth browsing flow, and clearly arranged categories for easier decision making.
WilliamKen –
Generic Cialis price Cialis 20mg price Generic Cialis price
Robertcob –
Shoppers today often prefer platforms that offer bright neon inspired shopping experiences with clearly organized deals and easy navigation for better convenience Glow Buy Neon Hub enhancing usability – It is frequently appreciated for its energetic design style and user friendly interface that supports smooth browsing
Lonniebog –
As I explored different online sites, I reached browse crown page and found it to be a nice site overall, offering useful content that seemed worth revisiting later when needed again.
MartinBus –
During a casual browsing moment, I discovered view this site and found it to be a clean and reliable website, giving a positive impression during my quick exploration today.
RichardDef –
Digital shoppers often highlight that engaging product selections make browsing more enjoyable and increase the likelihood of returning to a site, as seen on petal copper goods hub – the experience felt worthwhile since items looked appealing and made the platform feel like a place worth revisiting.
Derekvibly –
Modern buyers often appreciate tools like fast checkout browsing page – The cart choice store system is built to support rapid decision making, ensuring customers spend less time searching and more time selecting products that match their exact needs and preferences
Thomastenry –
Shoppers today expect fast, reliable, and well structured online stores that help them quickly move from browsing to selecting products efficiently, GoldenDune exploration hub – The platform offers a smooth experience where users can explore categories and items without unnecessary delays or complicated navigation steps interfering with their flow
DouglasMiz –
I was casually searching for deals online when I noticed take a peek here – My first impression is quite good, and the categories are arranged neatly, making browsing feel intuitive and smooth.
Clinttoott –
Online shoppers often value websites that reduce complexity and present products in a logical structure for faster navigation and better decision making Clean Speed Goods Zone – This version offers a clutter free environment where items are easy to find and browse efficiently
Waltercix –
While analyzing online marketplaces offering tech deals, I noticed a section named deal corner digital hub – The platform highlights affordable gadgets and digital products in a structured format, making it easy for users to find attractive deals and compare prices without difficulty during browsing.
Davidclota –
I had some free time and decided to explore a few artisan sites when I discovered discover harbor crafts and it looked very creative – Crafts here appear unique and interesting, and it’s definitely worth spending time exploring every section carefully.
Kevintix –
People browsing style focused websites often prefer layouts that highlight new fashion arrivals and simplify the browsing journey significantly style selection portal – the experience feels structured and easy to follow, helping users stay focused on clothing items while exploring various fashion categories
JeremyHef –
Online users often appreciate e-commerce platforms that feel innovative and visually distinctive, especially when exploring curated collections influenced by contrasting environments like icy frost and warm desert sands frostdune lifestyle portal – The idea reflects a bold marketplace identity where modern goods are arranged in a creative structure inspired by dual natural extremes, enhancing the sense of exploration during browsing.
Thomasreupt –
Shoppers looking for reliable trend updates often choose structured platforms like Smart Trend Store Showcase Hub – featuring clean interface design, well organized product listings, and smooth navigation tools that make browsing modern items easier and more enjoyable for everyday users online today.
RichardDef –
Many users browsing e-commerce platforms appreciate when the product selection feels fresh and inviting, making them want to explore further over time, especially on copper petal market view – browsing felt engaging because items seemed appealing and worth revisiting for a closer look at different categories and possible finds.
Robbielen –
Online consumers frequently enjoy platforms that showcase neon themed products in a fun corner designed for easy browsing and quick deal discovery Neon Style Fun Hub Corner making shopping smoother – The website is often noted for its lively presentation style and organized product sections that enhance usability
EmmettUnilt –
During a short search session online, I found open stone site and noticed smooth navigation with clear content presentation, which made the browsing experience pleasant and straightforward overall.
Juliantit –
Online consumers frequently prefer quality cart arenas because they offer smooth cart experience with well organized categories and checkout flow that simplifies purchasing decisions Quality Cart Arena Express Flow Hub – The interface ensures fast loading pages and easy navigation across all product sections
Vincentunurb –
Came across something interesting while scrolling earlier and thought it might be relevant to share here with everyone reading this thread discover this shop – The overall feel is quite unique, and it seems like effort was put into selecting items that stand out individually.
AaronFut –
During my search for online shopping platforms, I stumbled upon check this out now – The entire site looks well organized, making shopping online easier and more enjoyable as everything is easy to browse and understand.
GlennLix –
E-commerce environments today must support fast navigation and clear layouts so users can shop comfortably without facing technical or visual barriers Speedy Cart Portal – this platform improves accessibility and performance, allowing shoppers to browse deals and complete purchases with reduced waiting time and improved system responsiveness
Edwardcok –
I had some spare time and decided to explore a few sites when I discovered discover handmade shop and it looked quite inviting – The crafts feel authentic and nicely presented, making the browsing experience truly pleasant and engaging.
ThomasdAg –
While casually searching online, I came across something that felt simple and worth mentioning in this discussion check this site – It’s a nice shop overall, and the products look interesting and worth checking out if you browse further.
Stevenrak –
Shoppers who enjoy curated experiences often choose platforms that display selected items neatly while maintaining quick navigation features across the interface Handpicked Goods Center – This version emphasizes simplicity and speed, allowing users to browse featured items with ease
Williamlorce –
Busy individuals often rely on online stores that help them save time while ordering regular household supplies, and a relevant example is SmartDaily Market which emphasizes convenience while the service overview explains how it supports fast browsing and easy access to essential products for users managing everyday shopping tasks efficiently
WilliamKen –
how long does it take for semaglutide to work for weight loss rybelsus medication side effects buy drugs online
EddieensuH –
I was browsing randomly when I found a site that felt clean and artistic with a gentle structure and easy to follow design silver petal online hub – Beautiful collection here worth exploring for daily home inspiration today, offering calming ideas for home decoration.
Williamken –
While casually browsing online shops, I discovered check items here and it felt clean and structured – The design feels modern and comfortable to navigate, giving a smooth and pleasant browsing experience from start to finish.
RogerNeaks –
People browsing for unique decorative items online may come across niche creative hubs that include the Fern Handmade Corner section embedded in artisan marketplaces – it delivers a cozy and inviting selection of handcrafted pieces designed to feel authentic and personally meaningful to shoppers
RichardDef –
Many visitors exploring online marketplaces often mention that browsing feels pleasantly engaging when product selections are varied and visually appealing, especially on platforms like copper petal hub – the overall experience felt enjoyable since items looked intriguing and encouraged further exploration during the session with a sense of curiosity about what else might be available.
mostbet_nwel –
mostbet nu se deschide Moldova [url=http://mostbet13829.help]http://mostbet13829.help[/url]
Patrickunjub –
Many users enjoy platforms that make fashion browsing simple and visually clear, and Stylish Corner Trend Showcase Hub – provides clean interface layout, organized product sections, and intuitive navigation that enhances usability and improves shopping satisfaction significantly for everyday online users.
ShannonSeato –
Users exploring online stores often prefer imaginative branding that feels like discovering a hidden fantasy retreat, especially when browsing curated lifestyle and premium product selections frost eden goods showcase – It suggests a secluded winter enclave concept where cozy and carefully curated goods are displayed in a calm, magical environment that enhances browsing immersion.
DavidAdume –
While exploring online stores I found something that felt minimal and calm with a modern interface and easy navigation structure across sections twilight oak browse hub – Store has calm aesthetic with easy browsing and clean layout, helping users move through pages without confusion.
Roscoebaple –
Users browsing modern clothing stores generally prefer platforms that keep design simple and product discovery efficient modern fashion arena site – the experience feels smooth and structured, allowing users to quickly shift between categories and find outfits that match their style preferences
BrianSap –
While reviewing different websites during a short search, I stopped at learn more here and found the content pretty interesting, with everything arranged clearly so it was easy to go through and understand.
Dallasceato –
While browsing through various online shopping platforms looking for fresh items, I came across check this stylish hub – Products here look quite stylish and appealing, making it a nice place to discover new things online in a relaxed and enjoyable way.
Robertbiz –
Online shoppers who prefer structured checkout systems often use quality cart stations that provide efficient shopping station features with easy cart management and quick purchases designed for smoother buying experiences and faster decision making Quality Cart Station Flow Hub Explorer – The platform is appreciated for its clean layout, organized categories, and seamless navigation system that helps users manage carts and complete purchases without delays or confusion
Robertdeece –
While exploring tools for enhancing e-commerce performance and usability, I encountered flexible shop zone manager which supports store owners in organizing digital shops – it emphasizes improved control panels, smoother workflow handling, and scalable features that help businesses manage their online operations more effectively and with less complexity overall.
EdwardHob –
I was checking out different collections online when I found a shop that had a surprisingly fresh and inviting feel to it radiant collective picks and it immediately gave a sense of order and clarity that made browsing easy, – The experience feels thoughtfully crafted, with smooth navigation and a clean aesthetic that helps users explore without feeling overwhelmed or lost.
Vincentunurb –
Sometimes while casually searching online you run into something unexpectedly nice, which is exactly what happened to me earlier today check out this site – I like how everything feels intentional and a bit different from the usual mass-produced selections you normally see.
AlvinLam –
Shoppers seeking convenience and speed usually prefer platforms that combine quick product selection with efficient checkout systems for smoother shopping Ultimate Picks Market – This final version highlights a complete fast shopping solution with easy selection and smooth checkout flow
RichardDef –
Online visitors often mention that interesting product displays can make a site more memorable and encourage repeat browsing sessions, as seen on petalmarket copper collection – the browsing experience was enjoyable since items looked appealing and created a sense that the platform would be worth checking again later.
Justinplown –
While checking out handmade goods for fun, I discovered visit this page and it felt very structured – The items appear creative and the browsing experience was smooth overall, making exploration feel easy and enjoyable.
Sammybup –
While checking out online shops for fun, I discovered visit this link and it gave a structured and tidy impression – The layout is clean and navigation is easy, making browsing feel comfortable and enjoyable overall.
Raymondlap –
I was casually browsing online when I found a site that felt clean and easy to use with a smooth layout and clear product organization silver petal essentials – The emporium feels well organized with many appealing items available now, helping create a stress free browsing experience.
WilliamKen –
cialis for sale cheapest cialis Buy Tadalafil 10mg
Victorfiz –
Many shoppers value online platforms that emphasize seasonal artistry, especially when browsing curated handmade goods that blend garden freshness with frosty winter tones frostgarden floral craft portal – It suggests a gentle hybrid marketplace where decorative and artisanal items are displayed in a calming, nature-inspired digital environment.
Waltergoank –
While checking out various online stores, I came across see this shop – The product selection looks good, and it appears the inventory is regularly updated with fresh items that keep browsing engaging.
Charlieirrak –
Online users browsing trend based fashion websites often prefer simple navigation and clearly structured product listings for better user experience flow today Trend hub navigation link – interface layout is clean and organized, allowing users to find products quickly and move between sections effortlessly without any confusion or delay at all
Williamglach –
Online users who enjoy browsing mixed product categories often prefer platforms that organize items clearly while maintaining a consistent and easy shopping experience Market of Fern Finds – It provides a wide assortment of goods with an intuitive layout that supports stress free browsing and quick access to different product types
DavidAdume –
While exploring online I stumbled upon a store that felt calm and tidy with a structured interface and smooth browsing system twilight oak view hub – Store has calm aesthetic with easy browsing and clean layout, ensuring a comfortable user journey.
ElmerElulp –
While browsing late at night I found a store that felt smooth and minimal in design making everything easy to check out radiant essentials hub – The browsing experience was easy and the items seem quite useful for everyday use and general convenience purposes overall.
GregoryEvami –
Many users enjoy e-commerce platforms like quality trend centers that provide trend focused browsing with updated products and clean browsing design for everyday convenience Quality Trend Center Quick Access Hub – The system supports fast navigation and organized product discovery
Williamker –
Shoppers benefit from systems that organize deals in a structured way, allowing them to compare offers without feeling overwhelmed by too many options Savings Radar Hub this model focuses on guiding users toward the most relevant discounts through improved filtering and smart categorization techniques
Jameszet –
I wasn’t planning to spend much time browsing, but this one caught my attention because of how clean and organized it looked have a look at this page – The overall feel is neat and structured, making it comfortable and enjoyable to explore without confusion.
RichardDef –
Visitors to online marketplaces often note that interesting product variety plays a key role in keeping browsing sessions engaging and enjoyable, as seen on petal copper shop link – items were appealing and made the experience feel worthwhile, encouraging another visit to explore the catalog more thoroughly in the future.
Robertlew –
While browsing through various websites, I stumbled upon browse cloudberry goods and it felt clean and structured – The selection of products is nice and browsing here was simple and enjoyable, making everything easy to go through.
Pedronop –
During a random online search, I encountered explore more here – The website appears modern, and I had a good experience scrolling through different product sections today as it felt easy and enjoyable.
WillieRoope –
Digital users often appreciate e-commerce platforms that feel inspired by woodland groves, especially when browsing curated rustic crafts and handmade décor products frost grove rustic showcase hub – It represents a cold forest marketplace identity where wooden and artisan goods are arranged in a natural, visually calming layout.
Jacobgat –
While exploring various pages for comparison, I visited explore this page and saw that the arrangement of content feels balanced, offering a simple path for readers to follow without overwhelming them with too much information at once.
TimothyFoump –
I found a website while exploring online that felt modern and simple with a clean interface and well structured categories silver petal item hub – The store layout is simple and makes browsing very smooth experience, making navigation quick and intuitive.
Davidhed –
The website is frequently described as efficient because it allows users to access different product categories without experiencing slowdowns or lag urban speed store making it easier for shoppers to enjoy a seamless browsing experience where everything loads quickly and navigation feels natural and well optimized for convenience.
MarvinTof –
I found a website while browsing that felt minimal and organized which made it easy to focus on content without distractions radiant field portal – Clean layout and simple navigation make this site pleasant today and ensure a smooth and easy browsing experience overall.
RonnieAdume –
лучшие серии сериалов смотреть сверхъестественное
WilliamKen –
semaglutide results before and after rybelsus how to take online pharmacy no prescription needed
BrandonJoive –
Online shoppers who follow modern product updates often explore quality trend stations that act as reliable trend stations showcasing modern items and frequent product updates designed for smoother browsing and better decision making Quality Trend Station Flow Hub Explorer – The platform is appreciated for its clean layout, structured navigation, and fast loading interface that helps users quickly discover updated products without confusion or delays
RichardDef –
Visitors browsing e-commerce sites frequently enjoy discovering new and interesting products that keep their attention during the session, particularly on copperpetal product portal – the browsing experience felt engaging since items appeared worth checking again and encouraged curiosity about what else might be available on the platform.
Sidneypap –
During a relaxed browsing session, I found check items out and it immediately stood out for its peaceful design – The store feels calm and the products appear carefully curated, making browsing enjoyable and easy.
TerryInomo –
While casually checking out multiple shopping pages, I discovered explore this shop – The site appears tidy and browsing through it feels smooth and uncomplicated.
KevinCon –
During my usual browsing session, I found something that felt a bit different and interesting enough to share with others here take a look here – There are quite a few appealing items, and it seems like a place I’d revisit in the future.
AndresEnlib –
During my usual browsing session, I encountered check goods page and it immediately felt simple – Everything appears well structured and easy to browse through quickly, making it easy to explore without confusion or clutter.
Donaldthype –
I was casually searching for deals online when I noticed take a peek here – My experience so far is nice, as items are displayed clearly and descriptions help make product details easy to understand.
MichaelNeafe –
Many digital shoppers enjoy platforms that evoke coastal winter environments, especially when browsing curated lifestyle products inspired by icy harbors, calm seas, and seasonal decorative themes across organized product listings frost harbor craft market view – It suggests a calm and refined marketplace identity where curated goods are presented in a winter coastal aesthetic influenced by icy waters and tranquil harbor scenery.
HiramMet –
During my internet browsing I stumbled upon a shop that felt visually and conceptually different from typical online stores radiant grove shop hub – The selection is interesting and definitely stands apart from usual online stores, which makes it more engaging to look through slowly.
RichardDef –
Users who spend time on e-commerce platforms frequently appreciate when items are presented in a way that sparks interest and encourages return visits, as seen on petal copper marketplace – browsing felt satisfying because the product range appeared appealing and worth revisiting later for a closer look at different categories and offerings.
HaroldFluig –
People who browse online clothing stores regularly tend to appreciate sites that simplify product discovery through well structured categories trend station quick shop and this store appears to include attractive fashion options that may be useful for users looking for trendy outfit inspiration
Davidnog –
While browsing online I came across a store that felt modern and fresh with a clean layout that made exploring different categories smooth and easy silver sprout store hub – Nice selection of products here with a fresh and modern look, giving a pleasant and simple browsing experience overall.
MarcusBup –
In the middle of exploring unique online stores, I came across open this craft store – It gives a relaxed vibe, with a neat and simple layout that makes navigation feel natural and stress-free.
Henrydex –
Many digital shoppers appreciate quality trend zones that offer a nice zone for exploring trending products with simple navigation systems that help streamline decision making Quality Trend Zone Bright Hub Flow – The platform supports fast navigation and clean design structure
ArthurPouse –
While exploring online today, I found something that had a quiet and calming presence, so I decided to share it here browse this serene collection – The products look carefully crafted, and the experience feels smooth and peaceful.
mostbet_ceet –
мостбет зеркало для узбекистана [url=www.mostbet09654.help]www.mostbet09654.help[/url]
Williamidomo –
During a random browsing session across multiple platforms, I found click value hub – After a quick look, the site seems clean and easy enough to use, with a straightforward layout.
Michaelbeavy –
I was exploring different marketplaces when I found have a look here – The shop appears legit, with a clean interface and an impressive selection of products that makes browsing straightforward and pleasant.
JesseDeeno –
While going through different online shops, I encountered check lane essentials and it felt simple and neat – The essentials appear practical and nicely displayed across the site, making everything easy to explore without distraction.
Eliasronse –
Modern shoppers often look for online stores that provide structured navigation and reduce friction during product exploration and browsing activities VividCart Style Hub – The platform ensures smooth and intuitive browsing with clean design elements that make it easy for users to find products quickly while enjoying a visually engaging and user friendly interface
Leslieusalk –
As I browsed through several websites earlier, I came across see collection now and it gave a very tidy impression – I enjoyed browsing because everything is organized and visually appealing in a way that feels effortless.
RichardDef –
Online shoppers often highlight how a good variety of products can make browsing more engaging and enjoyable over time, particularly on copperpetal shopping portal – the experience was pleasant since items seemed interesting and left a positive impression that made the site feel worth checking again in future browsing sessions.
JesseTreno –
During a casual scrolling session across several websites, I paused at check this site and it appeared to be reasonably put together, leaving me thinking that it could be interesting to return later and explore it in more detail.
Donaldkeeri –
Users exploring digital marketplaces frequently appreciate seasonal branding that merges contrasting natural themes, especially when browsing curated rustic crafts and lifestyle goods frost harvest creative goods hub – This reflects a hybrid seasonal identity where handmade products are arranged in a soft, visually engaging structure inspired by harvest and frost elements.
Robertmen –
I came across this website during casual browsing and it felt easy to understand with a neat and simple interface radiant maple product view – I found some unique items while exploring this site earlier today, and it made the browsing experience feel smooth and worthwhile.
WilliamKen –
lowest dose of semaglutide rybelsus 7 mg cost best rx pharmacy online
Walterexada –
I was browsing through various online stores when I noticed check this goods page – The structure is well arranged, which makes browsing feel smooth and highly convenient.
Jameswaync –
While scrolling through various online shops I stumbled upon a store that felt elegant and earthy with stone themed design accents throughout stone light goods hub – Stone inspired designs give this shop a unique aesthetic appeal, helping create a refined and natural shopping experience.
Rogerphorp –
Many shoppers appreciate rapid buy markets offering fast shopping markets with easy access to everyday useful products for faster browsing and selection Rapid Buy Market Clean Flow Hub – The interface provides minimal design and efficient browsing tools
Jaspersef –
People who shop online for clothing often value websites that combine simplicity with a good range of updated fashion options trend zone station access and the platform seems to deliver a collection of trendy products that could appeal to users searching for fresh wardrobe additions
Richardblevy –
I wasn’t searching for anything in particular, but I did come across something that felt worth sharing after a bit of browsing take a look here – The selection is decent, and the overall structure makes navigation feel simple and convenient.
EdwardUrire –
While exploring different websites for ideas, I came across visit this urban buy site – The layout is simple and clean, making browsing through pages smooth and natural without distraction.
Anthonyuteni –
During my browsing session for new stores, I discovered explore this page now – I like how organized everything is, making items quick and easy to find with a simple layout.
AlfredSnabs –
Modern web visitors frequently choose platforms that deliver both performance efficiency and clean visual presentation for better interaction quality TrendCenter Browse System – It provides a smooth interface with fast page loading and logically arranged content sections that enhance usability and ensure users can explore different areas of the site without confusion or interruptions
RichardDef –
Shoppers exploring digital stores frequently enjoy platforms that offer a sense of discovery while browsing through different product categories and options, particularly on copper petal selection site – items felt interesting and made the experience worthwhile, encouraging another visit to see what new products might appear in the future.
DavidAPONA –
During my online browsing time, I stumbled upon browse meadow items and it felt very gentle – The calm layout made browsing feel relaxed and quite smooth, giving a smooth and simple browsing flow.
Jamescer –
Many shoppers appreciate platforms that feel like curated emporiums, especially when browsing winter-themed goods and cozy artisan product collections frostlane seasonal goods portal – The concept represents a warm boutique marketplace identity where products are displayed in a visually calm and inviting structure inspired by seasonal aesthetics.
mostbet_rvsi –
mostbet Urganch [url=https://www.mostbet59371.help]https://www.mostbet59371.help[/url]
Robertminty –
While browsing online earlier I came across a site that immediately felt calm and easy to explore which made me stay longer than expected radiant pine collective hub – Everything appears well organized overall, and the browsing experience feels simple, smooth, and free from confusion while moving through different sections.
KevinPealm –
I had been exploring different shopping sites when I noticed open this shop page – Everything loads quickly, and the content feels fresh, making the overall experience smooth and simple.
Devinimino –
While going through a variety of online stores, I encountered explore goods now and it felt clean and balanced – The modern layout ensures smooth browsing, making the entire experience comfortable and easy to navigate.
RonaldRoows –
Online consumers frequently rely on rapid cart centers that offer quick cart systems designed for smooth and efficient checkout processes improving satisfaction and usability Rapid Cart Center Market Flow Hub – The website is structured for easy product discovery and checkout flow
JosephGauff –
I had been browsing multiple shopping sites when I came across see this collection – It’s a decent store, and the browsing experience feels smooth with categories that are easy to navigate and understand.
Danielbix –
People browsing for affordable shopping options often appreciate platforms that present products in a clean format where pricing and value are easy to understand quickly price friendly shopfront and this website seems to offer a reasonable mix of budget items that could appeal to users who want simple and cost effective online purchasing.
ElbertCheet –
I came across this shop during browsing and it felt neat and practical with a clean design and well organized product categories sun haven essentials hub – Essentials here feel practical, useful, and nicely presented for shoppers, making the experience smooth and simple.
Stephentep –
In between browsing different platforms, I noticed visit urban buy station now – The structure feels clean and organized, and I could find everything easily without needing extra effort.
Lelandjet –
While going through different websites today, I stumbled upon something that felt solid enough to share in this discussion visit this online store – The overall presentation seems dependable, and the structure looks well organized and carefully arranged.
RichardDef –
Digital shoppers often highlight that engaging product selections make browsing more enjoyable and increase the likelihood of returning to a site, as seen on petal copper goods hub – the experience felt worthwhile since items looked appealing and made the platform feel like a place worth revisiting.
Gabrielteply –
Digital users often look for platforms that combine easy navigation with a minimal design approach that enhances focus and reduces distraction while browsing VividBrowse Station Center – The website ensures a smooth experience with intuitive layout design and clearly arranged content sections that allow users to find information quickly and interact with features without confusion or unnecessary effort
CesarSeace –
As I browsed through several websites earlier, I came across open petal shop and it stood out quietly – The aesthetic is soft and pleasant, and the items look carefully chosen, making the experience feel calm and easy.
Davidaneks –
During a quick search session across several pages, I found visit this link and liked the straightforward presentation, which made browsing feel smooth and uncomplicated.
WilliamKen –
Cialis 20mg price Generic Cialis price Cialis 20mg price in USA
Anthonysleby –
I came across this store while browsing and it felt surprisingly fast, with pages opening almost instantly every time radiant shore store view – The experience is smooth overall, and pages load quite fast here, which makes navigation feel simple and efficient.
DanielAdomb –
Users exploring eco-conscious online marketplaces often appreciate peaceful winter meadow branding that blends natural landscapes with frost imagery while browsing curated collections of sustainable crafts, lifestyle goods, and handmade products across organized digital categories frost meadow collective hub – The concept reflects a serene meadow-inspired winter identity where eco-friendly goods and artisan creations are presented in a calm, nature-focused environment that emphasizes sustainability, simplicity, and visual harmony.
BenitoSoine –
In the middle of comparing various online shops, I came across open this flower market – It has a pleasant atmosphere, and browsing different sections feels straightforward and well organized.
WilliamGon –
Users seeking efficient online shopping often prefer clean layouts and easy access Stylish Shopping Portal – A well structured browsing system ensures that visitors can find products quickly while enjoying smooth transitions between sections and maintaining a comfortable shopping experience overall
Normancal –
While testing different deal aggregation websites, I discovered organized deals hub which compiles various offers into neat sections – this shopnetmarket.shop service enhances browsing speed, reduces confusion, and allows shoppers to focus on relevant discounts while maintaining a smooth and straightforward user experience throughout their online shopping journey.
RichardDef –
Digital shoppers often highlight that engaging product selections make browsing more enjoyable and increase the likelihood of returning to a site, as seen on petal copper goods hub – the experience felt worthwhile since items looked appealing and made the platform feel like a place worth revisiting.
MichaelDot –
While casually exploring online shops, I discovered see this urban cart page – The experience is pretty decent, and the design looks modern while being easy to navigate throughout.
Howarddaf –
Online shoppers frequently value rapid cart hubs that function as central hubs for fast cart handling and convenient online shopping enabling quicker decision making Rapid Cart Hub Vision Flow Portal – The interface supports fast access and smooth checkout flow
HailerSabahr –
The collaboration and discussion started with Kavinsky’s team. When they spotted our old LED watches, they approached us with an idea to design a new watch that matches Kavinsky’s character. The red link button directly refers to Kavinsky, explains Antoine Aurelie, Yema PR manager.
ChrisKidge –
Online shoppers often value platforms that keep things simple while still offering a good range of budget friendly products Value shop discovery link – the experience feels well organized allowing users to compare items easily and make faster decisions during browsing sessions.
Richardsow –
I was just casually exploring the internet when I found something that felt simple, structured, and easy to navigate, so I thought I’d mention it visit this structured shop – It’s a nice shop overall, and everything being clearly categorized makes browsing smooth and straightforward.
StevenJEN –
During my usual browsing session I came across a site that felt bright and simple with a structured layout and easy navigation flow sun meadow market – Store feels bright, welcoming, and easy to browse through categories, giving a smooth and stress free experience.
DustinDrith –
While exploring various e-commerce platforms I evaluated navigation structure and clarity and found BestTrendStation product showcase – Great browsing flow, content is clear and visually quite appealing, making it easy for users to browse comfortably while maintaining a simple and well organized interface
Charlesunump –
I spent some time checking out various online shops and eventually found browse this petal market which looked neat and structured – The marketplace appears friendly and easy to navigate through different sections, making everything simple and pleasant to explore.
Nicolehiexy –
bluefocus.click – Blue focus provides clear direction and strong digital strategy guidance
MurrayHax –
During a relaxed browsing session, I found see shop page and it immediately felt well structured – The selection here is pretty decent, and the items look quality focused with a clean and visually appealing online display.
Williamneunk –
In between checking multiple online platforms, I encountered browse this peak hub – Everything is user friendly, and navigation feels smooth, making it easy to explore without confusion.
Josephskani –
I found a website while exploring online that felt visually appealing with a clean and softly glowing design style shadow corner goods hub – The shop has a cool aesthetic overall, and the product choices are interesting, making it worth exploring further without rush.
Jasonhiexy –
Digital consumers frequently appreciate e-commerce experiences that highlight artistic beauty, especially when browsing curated aesthetic goods, floral-inspired décor, and elegant lifestyle products frostpetal elegance goods portal – The concept reflects a delicate emporium where winter frost and floral aesthetics merge into a calm, visually refined shopping environment.
RandomNamehiexy –
Online shoppers benefit greatly from well designed platforms that support intuitive navigation and minimize the time required to locate specific products or deals where Stylish Commerce Hub – this system enhances usability by maintaining clean layouts and ensuring users can browse with confidence and ease throughout the entire experience
Jesuskip –
Modern online shopping tools often aim to reduce effort for users by organizing promotional content effectively, and this example fits that description deal browsing assistant – it is designed to help users quickly scan available discounts and offers in a way that feels intuitive and easy to navigate.
RichardDef –
Online shoppers often enjoy platforms where browsing feels dynamic and the product selection encourages curiosity and repeated exploration, as seen on petalmarket copper store – items were appealing and made the browsing experience feel enjoyable enough to return for another look in the future.
Lesterlix –
While scrolling through multiple online stores for comparison, I noticed explore urban zone cart – I liked how fast everything loaded, making the browsing experience noticeably more enjoyable and fluid overall.
JosephCrike –
стоматология рядом со мной номер телефона стоматологии
StephenUsels –
People often choose rapid cart solutions because they offer helpful solutions for cart management and streamlined buying experience overall, improving clarity and giving users better control over purchases Rapid Cart Solutions Smart Explorer Hub – The platform ensures intuitive navigation and well organized cart management features
Albertpsync –
During my analysis of e-commerce websites I observed navigation efficiency and interface design and found Best Choice Online product showcase – The platform is generally helpful overall, making it quick and convenient today to search for items, with a clean structure that supports easy and fast browsing across pages
JasonExext –
During my usual browsing session, I stumbled upon something that felt reliable and well put together, so I thought I’d share it here take a look here – It appears to be a trustworthy site, and the content feels authentic with a layout that seems carefully planned.
DonaldSof –
Users exploring online product listings often prefer platforms where visuals are sharp and consistent, allowing them to quickly compare different items without confusion or difficulty during browsing cart image browsing portal and the experience feels visually smooth and well organized, making it easier for shoppers to focus on items and enjoy a comfortable browsing session throughout.
CharlesNuh –
During a light browsing session across multiple platforms, I checked out go to this link and noticed right away that the site contained helpful information arranged in a way that felt structured and accessible.
ChuckWeict –
During casual browsing I came across a site that felt fresh and minimal with a soft design and easy navigation system sun petal discover hub – Market has good variety and items seem fairly well priced, helping users explore without complexity.
Brandonniz –
As I explored multiple online platforms, I came across view items now and it gave a soft impression – Simple and neat design made browsing feel quick and comfortable, making scrolling through items easy and stress free overall.
CharlesVow –
купить дизайнерскую люстру потолочную дизайнерские люстры
ThomasRen –
I had been jumping between different websites when I stumbled upon browse this flower store – The design is clean and organized, which makes it very easy to locate what you need without unnecessary effort.
WilliamKen –
Cheap Viagra 100mg order viagra Generic Viagra for sale
Thomasaluct –
While exploring online I found a store that felt visually refined and simple with a soft modern design language silk dune discovery hub – I enjoyed browsing here, as the items are stylish and reasonably presented, making it easy to stay engaged while exploring.
CarlosNaw –
Many digital consumers prefer soft and minimal retail platforms, especially when browsing curated floral-inspired décor, aesthetic gifts, and lifestyle product collections frostpetal winter retail hub – This reflects a gentle marketplace identity where products are presented in a calm, floral-winter inspired structure designed for relaxed browsing.
Charleshut –
Digital shoppers prefer online stores that emphasize clarity, structure, and fast access to product categories CartMarket Style Nexus enhances browsing efficiency while maintaining clean layout design and enabling users to navigate seamlessly across all sections overall experience better usability flow.
Wayneenuch –
In my review of online retail tools focused on simplicity, I came across minimal cart system that organizes shopping categories neatly – Simple shopping experience with clear layout and easy product access ensures users can quickly browse products and make decisions without unnecessary complexity or excessive steps during the shopping process.
GeorgeGlync –
During a random search session, I noticed explore urban flash hub – The site feels light and responsive, making it a nice and easy place to explore without friction.
RandomNamehiexy –
While exploring different online shops, I came across see petal items and it immediately felt light and refreshing – The theme looks soft, clean, and very welcoming visually, creating a browsing experience that feels relaxing and simple.
TimothyCal –
Creative professionals working on digital portfolios often need platforms that highlight design quality while ensuring fast and smooth page performance SkyCanvas Studio – The platform delivers visually appealing layouts and seamless navigation, allowing users to showcase creative work in a polished environment that reflects professionalism and modern digital design standards effectively
Jeffreyecofs –
Many digital users prefer rapid goods centers because they offer fast access to goods with well organized categories and listings making online shopping more convenient, structured, and easier to manage across different product sections Rapid Goods Center Smart Navigation Hub – The website provides intuitive controls and responsive design that enhance usability and improve browsing speed
JamesRaw –
Sometimes you find something online that just feels smooth and well designed, and this was one of those cases for me today take a look at this site – It has a clean design, and the simple navigation makes the overall experience enjoyable and effortless to explore.
JasonHok –
Shoppers who enjoy browsing products online often appreciate platforms that are optimized for smooth navigation and quick transitions between different listings and category sections smooth cart experience page and the layout feels responsive and easy to follow, allowing users to scroll through items comfortably while focusing on product selection without unnecessary distractions.
Phillipjopay –
While casually scrolling through online shops, I noticed visit pine page – The experience feels structured and simple, making it easy to follow while browsing different sections.
Bryantwow –
During a casual online search across different marketplaces, I discovered explore cloud ridge goods and it stood out with a tidy layout – The products appear well organized and easy to find on this site, giving a simple and pleasant browsing experience.
DanialDah –
I was casually browsing online when I found a store that felt minimal and functional with a simple layout and well structured product categories sun petal essentials – Simple store design makes shopping here quick and enjoyable experience, helping users move through pages without effort.
JamesUnsom –
During my usual browsing I found a store that felt like a calm marketplace environment with a straightforward layout design silver bay collection hub – The marketplace feel is nice overall, and the variety of products available here is decent enough to keep browsing interesting.
RubenEmowS –
Digital consumers benefit from platforms that make browsing faster through simplified category access and well arranged product listings throughout the site SmartCart Browse Zone – this approach improves user satisfaction by ensuring clarity in navigation and reducing time spent searching for specific products online overall.
Davidfen –
Many shoppers enjoy online stores that emphasize forest-inspired aesthetics, especially when browsing curated eco-friendly goods and rustic lifestyle product collections frostpine craft goods portal – It suggests a strong natural marketplace where handcrafted items are displayed in a structured environment inspired by evergreen forest traditions.
PatrickCix –
Modern e-commerce users expect seamless experiences that allow them to complete purchases without confusion or delay Fast Buy Interface the system is optimized for ease of use – offering quick navigation paths and a clean layout that supports efficient shopping from beginning to end
Thomasjep –
In between browsing different platforms, I noticed visit flash hub now – The structure is clean overall, and the content is easy to follow along without difficulty.
MatthewMIZ –
Online shoppers frequently use rapid goods corner platforms providing convenient corner for quick shopping and simple product discovery today, ensuring smooth browsing and efficient access to a wide range of products BrowseSmart Rapid Corner Flow Hub – Enhances user experience with clean design and quick navigation tools
DavidBog –
I stumbled upon something today that felt easy to explore and worth sharing because of its pleasant design visit this goods shop – I enjoyed checking it out, and it seems like a reliable shop with a neat and accessible structure.
JamesWax –
I had been exploring different sites when I found open collective ridge – The layout feels modern and easy to use, with a responsive structure that keeps browsing smooth.
Williamnut –
As I explored multiple sections and features, I found that view more info integrates into a tidy structure – discovered it today, and the platform looks informative, engaging, and well organized overall.
WilliamKen –
Viagra Tablet price Viagra online price Viagra tablet online
TimothyTeape –
Shoppers who enjoy browsing online stores often prefer websites that make navigation simple through clear category separation and consistent structure across all product pages and sections vivid cart zone access point and the organization of categories feels intuitive, allowing users to move smoothly through the platform while maintaining focus on finding relevant products quickly.
Hymanheish –
Digital shoppers looking for curated agricultural collections often seek platforms that balance product diversity with clean and accessible design Golden Crop Collection Shop – It offers a curated selection of harvest inspired products displayed through a user friendly interface designed to enhance browsing comfort and clarity
KeithTriat –
While browsing through several online shops earlier today, I came across cloud spire goods hub and it immediately felt modern and clear – Nice clean interface made browsing here smooth and straightforward overall, with everything easy to find and view.
DennisBic –
I was casually browsing online when I came across a shop that felt clean and neatly arranged with a simple browsing experience silver crest essentials – The products look reliable and the descriptions are clear and helpful overall, which makes the site feel trustworthy and easy to use.
Patrickval –
As I explored multiple online platforms, I came across view items now and it gave a clean impression – The products seem interesting and a bit different, and browsing here was actually quite fun and relaxing overall.
FrankWhile –
Best price fashion hubs are widely used by consumers who prioritize affordability and style while shopping for clothing and accessories online Best Price Fashion Hub This hub emphasizes competitive pricing on fashion items while maintaining a stylish catalog helping users find the best deals without compromising on modern trends
JamesaDund –
While exploring online I stumbled upon a store that felt clean and modern with a structured interface and smooth browsing system sun spire view hub – Collective offers interesting products and overall pleasant browsing experience today, ensuring a comfortable browsing experience.
RodneyPoott –
Online users often appreciate e-commerce platforms that feel inspired by quiet ocean shores in winter, making browsing more engaging when exploring curated coastal décor and lifestyle product collections frost shore aesthetic hub – The idea reflects a minimalist seaside marketplace where goods are displayed in a visually calm structure influenced by cold ocean tones and clean design aesthetics.
Harryslole –
In the process of exploring ecommerce marketplaces, I came across a platform that delivered a straightforward and efficient browsing experience with minimal clutter and clear structure BuyZone market entry page integrated naturally within the content area – The marketplace offers a wide variety of items and ensures users can browse comfortably without distractions or unnecessary complexity in navigation.
Rogerclink –
In between browsing different platforms, I noticed visit flash market now – The layout feels good and clean, and everything is easy to see clearly from start to finish.
mostbet_yxMt –
mostbet drugi depozyt bonus [url=http://mostbet2002.help/]http://mostbet2002.help/[/url]
melbet_usSl –
melbet пополнить с мбанк [url=http://melbet45163.help/]http://melbet45163.help/[/url]
JesusDEERA –
People interacting with online platforms often appreciate when design is minimal, modern, and optimized to make navigation feel natural and effortless UltraWave UX Portal – UltraWave offers a clean and modern interface where browsing is smooth and easy, ensuring users can explore content without distraction or complexity.
MichaelNow –
From my perspective after exploring several pages, check it out sits within a well-organized interface – the browsing feels smooth, and the structure makes navigation straightforward and intuitive.
Derricksoume –
During a casual browsing session where I was exploring different shopping platforms, I came across visit this shore shop – The first impression feels positive, and the content is simple, well structured, and clearly presented throughout the pages.
RolandTek –
While reviewing the interface and moving through sections, I came across go to this site which fits into a neat structure – checked this out quickly, and it looks like a neat and useful site overall.
ThomasAdege –
I was going through different websites earlier and found one that had an interesting collection worth mentioning here see this shop – The collection is interesting, and I may come back again to explore more items later on when I can spend more time.
Kevinisodo –
Users browsing fashion or general product stores frequently appreciate discovering appealing items that encourage them to revisit the platform later for more browsing sessions trend center item hub and the site provides enough variety and interesting picks to keep users engaged and willing to return for additional exploration over time.
Timothynit –
While scrolling through various websites I found a store that felt minimal and clean with a clear and structured interface silver dune goods hub – This site feels modern and easy to navigate for new users, offering a smooth browsing experience from the very start.
RichardGep –
While casually browsing and testing navigation, I noticed that follow this link contributes to a smooth experience – clean website overall, and it feels modern and easy to browse around today.
Ronaldinink –
People searching for elegant and budget friendly online shopping destinations increasingly value platforms that prioritize savings alongside visually appealing layouts and smooth user experience Elegant Savings Corner It provides a refined browsing space where users can explore discounted products presented in a stylish way making online purchasing both enjoyable and efficient for everyday needs
Rolandjepsy –
People who enjoy streamlined online buying usually search for websites that reduce effort and save time when selecting basic products for home use and routine shopping everyday essentials store – Many users find this kind of platform helpful because it presents essential items in a clear structure that supports faster decision making and easier navigation overall
ZacharyFub –
Many people exploring digital creativity tools enjoy interactive environments that encourage learning, idea sharing, and structured inspiration discovery frostspire knowledge idea hub – The idea suggests a collaborative learning space where creativity and education merge into a seamless interactive experience.
Robertamoup –
Users browsing modern websites generally prefer interfaces that are simple, responsive, and designed to guide them naturally through content without confusion SummitMedia Flow Interface – SummitMedia provides a well-organized and clean interface where navigation feels smooth and intuitive, allowing users to enjoy a comfortable browsing experience overall.
RobertLax –
While comparing different online store platforms I recently discovered Urban Pick Corner website link – Browsing through the pages felt natural and well structured, and I did not encounter any difficulty locating information, as everything appeared logically arranged and easy to interpret from start to finish
Charleshen –
While casually searching the internet I discovered a site that felt clean and organized with a modern interface and clearly defined categories sun woven goods store – Market feels creative with well curated items and smooth navigation, helping users find items quickly and without effort.
JerryFab –
International shoppers often explore global marketplaces that provide diverse product ranges and cross category selections and they frequently browse the Global Horizon Goods which offers an internationally inspired product selection with a clean layout and smooth navigation that supports easy access to items from various categories and enhances the overall browsing experience.
Jamesobemn –
People evaluating online systems often focus on usability, clarity, and how well the interface supports concentration and efficient browsing FocusUltra Clean Portal – The UltraFocus platform delivers a clear and structured layout where everything is simple, helping users stay focused and browse efficiently.
Terryordem –
After spending some time exploring different sections and observing the structure, I noticed that check this platform fits naturally into the experience – the site feels modern, and the overall layout gives a clean and visually appealing browsing impression.
HermanOveme –
In the middle of checking different shopping platforms, I came across open this trail store – I enjoyed visiting it, as the site feels smooth and all information is easy to read and understand.
KennethEngab –
During a relaxed browsing session, I found see shop page and it immediately felt simple and organized – The layout is well structured and easy to explore, creating a great browsing experience that feels easy and comfortable.
WilliamKen –
Tadalafil Tablet Cialis 20mg price in USA Cialis 20mg price
Scottemife –
During my usual browsing session I came across a site that felt simple and efficient with a clean interface and clearly arranged product categories urban bay market hub – Goods selection looks practical and well suited for everyday needs, offering a smooth and practical shopping experience.
DustinMor –
I wasn’t expecting to find anything notable, but I came across something that felt fresh and visually pleasing while browsing online visit this goods store – The site feels fresh, and I like the way products are displayed in a simple and modern structure.
BobbywaW –
I came across this website while browsing and it felt very organized with clear structure that made moving through sections feel natural silver fern store hub – I like how everything is categorized, which makes browsing really simple and helps keep everything easy to find quickly.
Kevinisodo –
Online shoppers often enjoy discovering appealing products that stand out from regular listings and make them interested in coming back later to see what else is available vivid shopping discovery link and the platform creates a browsing environment that feels engaging enough to encourage repeat visits for additional exploration and product checking.
Robertnut –
People searching for reliable savings platforms often appreciate websites that combine modern design principles with practical deal listings that are easy to browse and understand Savings Style Center – This variation highlights a more curated approach to online discounts where users can find structured promotional items presented in a clean interface designed for better shopping flow and improved product discovery
melbet_ewst –
melbet ставки на спорт [url=http://melbet49375.help]melbet ставки на спорт[/url]
MonroeAgile –
Digital shopping environments are increasingly optimized to deliver smooth transitions from browsing to final purchase Smooth Purchase Portal – This portal is designed for uninterrupted flow, ensuring customers experience fast, reliable, and user-friendly checkout processes from start to finish always consistently
ShaneJog –
Digital consumers frequently appreciate e-commerce platforms that blend industrial modernism with warm branding, especially when browsing curated essential tools and lifestyle products glowforge creative essentials portal – The concept reflects a marketplace where energy-inspired aesthetics merge with functional product curation in a clean, structured layout.
ArthurGaw –
People browsing online platforms often look for professional layouts, simple structure, and fast readability that supports easy understanding of content LaunchPro Access Hub – The ProLaunch website appears professional with neatly structured content, making it easy for users to read quickly and navigate without confusion.
Milfordvok –
While comparing several online retail interfaces, I observed consistency in layout helps user comfort, and UrbanPickZone web portal – The browsing experience feels smooth and well structured, allowing quick access to sections without confusion or unnecessary steps.
DouglasWab –
After reviewing a few pages and spending only a short time on the platform, I found that open this site fits into a user-friendly structure – the content appears simple, useful, and accessible to most users.
Anthonylor –
While browsing for new online stores, I discovered browse ember site – It looks like a solid platform, and browsing around feels straightforward and easy to follow.
Joshuahiexy –
I was exploring various websites when I found one that felt modern and warm with a clean layout and structured product display swift maple goods collection – Corner shop has cozy feel with surprisingly diverse product range, helping create a smooth and enjoyable browsing journey.
Rodneyvam –
Users exploring minimalist online stores often appreciate layouts that emphasize clarity and reduce unnecessary visual complexity Soft Meadow Marketplace allowing them to focus more on products that suit their needs while browsing comfortably and efficiently across a clean and simple interface experience flow
Arturosep –
While looking for reliable sources of tech knowledge, I found daily tech updates hub – a site that provides consistent insights into technology trends and helps users stay connected with modern innovations.
Josephvon –
While reviewing the interface and scanning content flow, I noticed that learn more here integrates into a clean layout – this page feels smooth, and browsing around was actually pretty enjoyable overall.
RandomNamehiexy –
In discussions about goal-oriented browsing platforms, some users point out that grow strategy site appears in collections focused on simple layout structures and helpful organization of informational material. – The design is often considered straightforward and accessible.
RalphIdosy –
While scrolling through different pages I came across a shop that felt clean and balanced with a smooth and structured layout silver field selection – The clean design and good layout make this store enjoyable today, offering a very easy and pleasant browsing experience overall.
Ernestbob –
Users searching for stylish items online frequently value platforms that make navigation simple while showcasing a wide range of categorized products clearly Fashion Goods Explorer – It is described as an exploratory space where users can discover fashion focused products in a structured environment designed for smooth browsing and improved shopping satisfaction
Stephenbep –
I wasn’t searching for anything specific, but I ended up finding something that felt worth mentioning because of its clean structure explore this ridge store – It’s good for browsing, and the layout is smooth, making it easy to follow everything without any hassle.
Haroldchodo –
Shoppers often prefer digital stores that provide stable performance and clear navigation paths during product searches and purchases Seamless Cart Space ensuring users can browse comfortably while experiencing fast and reliable system responses throughout their session – The platform prioritizes simplicity and consistency for improved user engagement
Russellnut –
People interacting with online platforms often appreciate when design is responsive, dynamic, and optimized for fast navigation that enhances usability SharpWave UX Portal – SharpWave offers a dynamic interface where navigation works fast and very smoothly, making it easy for users to explore content without lag or complexity.
BrockMum –
People browsing modern websites usually expect intuitive layouts and organized information flow that supports fast comprehension of content overall experience BrandVision info center – the information center approach of BrandVision ensures users can easily identify relevant topics and navigate without unnecessary distraction or confusion.
VincentMusty –
While casually browsing online I discovered a storefront that feels clean and well arranged with a layout that makes exploring categories feel easy and natural goods archive urbancrest offering a simple and structured interface – The browsing experience is smooth, practical, and easy to navigate
RobertLog –
While analyzing several e-commerce platforms for comparison I discovered Urban Style Bazaar digital storefront – The layout was organized in a way that made browsing feel natural, and I could move between categories quickly while everything remained clean, structured, and easy to understand without unnecessary complexity or distractions
CraigCox –
I spent some time looking through various sites and came across view copper goods collection which felt well structured – The variety is good and everything looks arranged in a clear way, creating a comfortable and easy browsing experience.
MichaelCep –
While looking through idea and creativity platforms, I found world insight hub – a site I like visiting because it always has something fresh and interesting that makes browsing a rewarding experience.
Terrymus –
As I examined the structure and how the information is displayed, I noticed that this page here contributes to a straightforward experience – everything appears clean, and understanding the content is easy and natural.
MichaelEpimi –
During a casual online search across different websites, I discovered explore ridge shop and it stood out with its clear design – The layout and presentation made it easy to quickly locate what I needed, creating a smooth and efficient browsing experience overall.
Henryfus –
In the middle of comparing different platforms, I came across check this collective page – Everything loads nicely, and the structure feels organized and pleasant, making navigation straightforward.
RobertTraix –
Digital enthusiasts exploring modern platforms appreciate systems that deliver fast responses and maintain clarity across all interactive elements FlowSync Interface since efficiency improves overall satisfaction – This platform provides structured navigation with responsive design elements that ensure users can access information quickly without encountering unnecessary complexity or delays during use
WilliamKen –
what does rybelsus look like rybelsus alternative international pharmacy
HenryFlalo –
As I explored different self-development platforms online, I encountered growth support hub – which provides structured and practical ideas for improving skills and achieving steady progress over time.
Deweyswish –
While casually browsing different websites I came across something that felt soft and organized with a balanced layout and smooth visual presentation that made browsing pleasant twilight cove browse collection – Collective site gives calm aesthetic and relaxing browsing experience overall, helping users explore comfortably.
Jamesboamp –
During my usual browsing session I found a site that felt creatively structured with a layout that clearly tried to break standard patterns silver grove market hub – The concept behind this store is interesting and stands out from others, giving it a unique browsing experience overall.
Luciusdot –
People reviewing digital branding websites usually focus on how effectively the platform communicates identity through design, clarity, and structured presentation of content across pages MatrixBrand Interface Node – The BrandMatrix platform offers strong branding with a modern interface design, ensuring users experience a clean, polished, and visually appealing environment throughout their browsing journey.
Keithnex –
People who regularly shop online appreciate websites that maintain consistent speed and clear category separation for improved browsing efficiency while also ensuring product pages load without delays even during peak traffic hours Elegant Goods Navigator – This navigator style platform emphasizes elegance in design while maintaining fast performance and smooth transitions between product pages for a better user experience overall
Terryrer –
Shoppers interested in floral inspired goods often value marketplaces that offer fresh designs and well organized digital presentation of products Fresh Bloom Marketplace presenting a wide selection of nature inspired items arranged in an easy to browse format – the site provides a clean interface, appealing visuals, and a structured layout that supports effortless discovery of seasonal collections.
Thomascex –
In my exploration of online business tools, I came across digital shop toolkit which provides streamlined features for store management – it improves workflow organization, supports scalable architecture, and helps developers and business owners build efficient e-commerce platforms that remain easy to maintain while offering strong performance and usability benefits.
Josephjag –
I was going through different websites earlier and found one that felt easy to navigate and worth mentioning here see this shore site – Everything is organized well, making it quick and convenient to find what you’re looking for.
Franknew –
While testing a few online shopping interfaces for usability, I noticed that the layout was quite organized and user friendly, and Urban Trend Arena official page overall everything seems nicely arranged, didn’t take long to get around, making the browsing experience feel smooth, straightforward and surprisingly easy to adapt to within a short time frame
Waynetah –
During my usual browsing session, I encountered check market page and it immediately felt simple and clear – Browsing here was smooth, and the items seem interesting and worth checking again later.
DanielNug –
After reviewing several parts of the site and observing the design closely, I found that open this site blends into a user-friendly layout – everything feels smooth, and accessing information is straightforward and convenient.
HollisTrelf –
In the middle of checking different shopping platforms, I came across open this petal site – The design is clean and minimal, and it improves the browsing experience by keeping everything straightforward and easy.
Jamesfluro –
While exploring various online stores I discovered a site that feels polished and minimal with a layout that supports smooth navigation and attractive product display urban harbor collection hub offering organized structure – The collective ensures visually consistent and appealing presentation
RichardDer –
Freelancers working in competitive industries often seek platforms that allow them to improve productivity, manage tasks efficiently, and achieve consistent project delivery outcomes Fast Track Growth System helping them maintain focus, streamline workflows, and ensure timely completion of assignments while improving overall operational efficiency
DavidSwava –
While reviewing layout and testing navigation, I saw that open this link integrates into a clear system – the site looks quite organized, and I found it easy to explore content here overall.
ThomasIdets –
When reviewing online directories of technology focused content and learning resources, users occasionally highlight platforms designed for simplicity including tech beyond guide point which is often mentioned as a clean and organized digital space. Navigation feels straightforward and user friendly across sections.
RobertNOb –
People evaluating websites often focus on perceived security, design clarity, and how easily they can move through structured content without confusion VaultBright Interface Hub – BrightVault ensures a secure and visually clean interface where users can navigate easily and enjoy a polished, comfortable browsing experience overall.
Bennienof –
While looking for a steady source of industry news and insights, I discovered innovation pulse guide – which offers useful updates and keeps me informed about the latest trends shaping different fields.
TimothyGom –
While browsing online earlier I found a store that felt calm and well structured with a smooth interface that made everything easy to access without confusion silver harbor store hub – The smooth browsing experience stands out, and the products seem thoughtfully selected here, giving a balanced and pleasant feel overall.
Stephentak –
Shoppers who prefer modern looking platforms often look for websites that load quickly and organize items in clear sections Modern Item Corner the corner highlights modern design principles and fast navigation helping users enjoy a seamless browsing experience across categories
Phillipkiz –
Shoppers who actively look for price reductions and seasonal promotions appreciate platforms that streamline access to relevant offers across various categories Price Drop Network – The system tracks and displays reduced pricing opportunities in real time, ensuring users can take advantage of savings quickly and efficiently without missing important deals.
Jasonmek –
People who want to simplify their approach to happiness often seek easy-to-follow advice that fits into real life, and they may explore simple-life-practices – This type of content focuses on removing unnecessary complexity while encouraging habits that naturally improve mood, focus, and emotional well-being over time.
TimothyWar –
As I moved through a few online pages earlier, I discovered visit aurora shop and it gave off a modern vibe – I enjoyed visiting this site since the items appear trendy and interesting, making the overall browsing experience enjoyable and easy.
Donaldpinge –
While casually browsing different websites I came across something that felt elegant and organized with a structured layout and soft visual tone twilight crest browse collection – Store feels polished and easy to navigate across all sections, helping users explore with ease.
pinup_rskt –
pin-up kazino slots [url=https://www.pinup2010.help]https://www.pinup2010.help[/url]
Jamessit –
People browsing modern web platforms often appreciate when interfaces are simple, fast, and designed to reduce complexity during interaction with content ConnectUltra Clean View – The UltraConnect website offers a user friendly and modern experience where fast loading pages and clear structure make browsing efficient and enjoyable.
Issacblils –
While exploring different online marketplace designs I came across a platform that felt surprisingly easy to use Urban Trend Center portal page – The browsing experience is smooth and stable, with clear navigation that helps users move around efficiently without getting distracted or stuck
Lonniemub –
After spending a few minutes exploring multiple sections, I found that open this site fits within a well-structured interface – the design feels user friendly, and the browsing experience remains simple and intuitive throughout.
AndrewSig –
I like sharing interesting finds occasionally, and this one stood out because of its thoughtful and unique product style browse this shop – The store is nice, and everything seems carefully designed with a creative and unique touch.
BryanSeish –
During a random browsing session across multiple platforms, I found click windspire collective – The site appears reliable, and everything is smooth and easy to navigate without confusion or clutter.
Kevinhiexy –
Many digital marketplaces now focus on rustic themed collections that highlight handcrafted quality and nature inspired aesthetics for modern consumers Pine & Craft Bazaar showcasing a wide assortment of artisanal goods that reflect forest inspired creativity and traditional workmanship – this site offers a balanced combination of visual appeal and practical navigation for everyday shoppers.
PeterVem –
Users exploring stable online platforms often value systems that maintain consistent performance and reliable structure during everyday browsing across different sections and content areas WebSource Stability Hub – The platform delivers a solid and dependable browsing experience with structured layouts and consistent responsiveness that ensures users can navigate smoothly while enjoying reliable performance across all pages without interruptions or instability during use
Geraldthert –
Digital users often appreciate websites that maintain a premium look while ensuring content is organized in a way that supports fast understanding ZoneElite Navigation Hub – The EliteZone platform offers a premium vibe with structured layout design, making browsing easy, clear, and visually consistent for all users.
WilliamKen –
Tadalafil price Generic Cialis price Buy Tadalafil 20mg
Kennethtob –
https://viagra.onl/# Generic Viagra online
Jessenadit –
While exploring online stores I found a site that felt fast and efficient with a modern design and seamless page loading system silver horizon collection view – Everything loads quickly and interface feels very user friendly today, creating a smooth and enjoyable browsing experience overall.
Walterdut –
Users who prefer streamlined shopping often seek platforms that unify product discovery and checkout into a single easy to navigate interface Style Checkout Hub – The hub integrates organized listings with a fast checkout flow helping users complete purchases efficiently without unnecessary navigation steps
Marvinses –
While exploring ecommerce pages I discovered a platform that feels minimal and structured with a clean interface that highlights products effectively under a creative theme lighthouse urban goods hub designed for usability – The store’s unique theme supports neat and organized product presentation
Andrewpievy –
While evaluating online shopping systems focused on structured browsing, I discovered shop foliage market that groups products into simplified categories – Shop tree market feels organized with useful categories for shoppers and helps users navigate efficiently by presenting items in a clear layout that reduces browsing effort and improves shopping convenience overall.
Roberthiexy –
During my search for streamlined digital experiences, I discovered smooth design guide – which presents helpful information in a neat and organized format, ensuring a comfortable browsing experience for all users.
Jamesrex –
https://viagra.onl/# over the counter sildenafil
RichardZon –
During my browsing evaluation of different shopping websites I focused on usability and flow and Trend Hub user portal – The site feels dependable enough, with a clean layout and responsive pages that make navigation straightforward and easy to understand while exploring different sections
Davidmop –
From my perspective after a short browsing session, check it out sits within a well-structured design – the first impression is positive, and the interface feels modern, clean, and approachable.
WilliamLor –
While casually exploring online marketplaces, I paused when I saw discover more here – The platform seems thoughtfully organized, with a layout that helps users find what they need quickly without any unnecessary complications.
Briankem –
I stumbled upon something today that felt peaceful and well designed, which made it stand out enough to share here visit this oak store – The vibe feels very calm, and the products appear curated in a thoughtful and aesthetically smooth way.
Rodolfoval –
While reviewing various online branding systems I observed consistency and usability strength and found Build Your Brand project hub – Great branding platform, tools are useful and easy to understand, ensuring a smooth experience where users can easily navigate and apply branding features effectively
GeorgeDed –
In many explorations of productivity oriented websites and clean interface designs, users occasionally point out idea orbit core in collections that emphasize structured browsing, clear layout, and minimal distraction for everyday informational use. – It is considered simple, elegant, and well organized.
Davidpeede –
Users comparing digital experiences frequently focus on usability, speed, and how effectively platforms guide them through information < AlphaForce Impact Page – The site maintains a clean and impactful layout where content hierarchy is well defined, helping visitors understand information flow without confusion.
Steveshura –
After spending time navigating through pages, I observed that access this link aligns with a clear presentation – interesting layout overall, and everything seems simple and easy to navigate around.
Shawncar –
During my usual browsing routine, I encountered check craft page and it immediately felt neat and structured – The crafts selection feels creative and thoughtfully organized, creating a relaxed and easy browsing experience overall.
KevinRon –
As I browsed through different online learning platforms, I encountered answers ideas space – a resource that shares helpful insights and encourages users to explore various ideas while also providing quick and easy-to-understand answers to common queries.
Marvinset –
Users interested in calming coastal aesthetics often browse online marketplaces that emphasize serenity and handmade goods for mindful lifestyle shoppers everywhere online Users interested in calming coastal aesthetics often browse online marketplaces that emphasize serenity and handmade goods for mindful lifestyle shoppers everywhere online Coastal Serenity Market offering peaceful themed collections for home decoration – A serene shopping platform that highlights coastal calm and artisan quality
Robertavash –
Generic Cialis price Buy Tadalafil 5mg Cialis without a doctor prescription
Jamesmal –
While casually searching the internet I discovered a site that felt simple and modern with a structured layout and easy usability silver lane goods store – Found this shop quite easy to use and navigate around, helping the browsing experience feel smooth and intuitive.
CraigSesty –
Users who frequently shop online prefer platforms that keep navigation intuitive and product categories easy to understand for better browsing efficiency Simple Goods Zone – It ensures that stylish items are arranged in a logical way allowing users to explore different sections without confusion or delay
Williamlap –
When browsing home product websites, many users are drawn to collections that evoke comfort while still maintaining a clean and modern aesthetic presentation style Cozy Home Collection – it focuses on warm, inviting household items arranged in a visually simple layout that enhances browsing comfort and product understanding
ToneyTor –
During my comparison of online retail interfaces I studied layout design and interaction flow and UTS online browsing center – The browsing experience felt smooth and easy to understand, with a structured design that allowed quick navigation and comfortable exploration of different sections.
Ronaldemavy –
People interacting with web platforms often value intuitive navigation systems and well-structured layouts that make browsing efficient and reduce cognitive load UrbanNexus Flow Portal – UrbanNexus offers a visually appealing interface where simplicity meets functionality, allowing users to explore content easily and enjoy a smooth and engaging browsing experience.
Ronaldnuary –
After reviewing multiple sections and paying attention to the layout, I found that open this site fits within a well-organized structure – the interface feels clean, making it easy to find things without delay.
Johnhiexy –
As I continued looking for organized educational resources, I discovered structured insight page – a platform that offers well-arranged information to help users understand topics step by step with ease.
Shanenulty –
Analytical discussions of online boutique ecosystems frequently include inline references that connect theory with practical examples of storefront design, particularly when observers notice soothing visual online shopping space UPC – These shopping spaces are designed to evoke a sense of calm through visual softness and structured content placement, which supports longer browsing sessions without causing user fatigue.
Horaceemets –
During a random browsing session, I ended up finding enter this shop – The interface feels clean and simple, creating a relaxed and enjoyable experience that makes browsing feel effortless overall.
Enriquepoism –
Creative professionals across industries often seek digital ecosystems that foster innovation and collaboration and a strong example is Idea Explorers Space which provides tools for idea discovery and refinement – A versatile creative platform that helps users explore new possibilities and transform imagination into actionable outcomes
KeithfUg –
Users interacting with digital websites typically prefer innovative systems with simple, effective design that enhances usability and reduces confusion ZenithLabs Navigation Node – ZenithLabs offers an innovative interface where the layout is simple yet effective, making it easy for users to navigate and understand content.
Stevenhiexy –
oakridgeemporium.shop – This store caught my attention, design is simple yet appealing.
AbdulKashy –
While exploring online I stumbled upon a store that felt smooth and well designed with a modern interface and clear product grouping silver oak view hub – Overall good experience browsing through items and checking different categories, making browsing feel simple and accessible.
TeodoroTUT –
Many users exploring digital marketplaces look for spaces where curated products are presented clearly and navigation feels smooth across different categories and sections Curated Style Picks – The experience emphasizes organized collections of stylish goods paired with a fast browsing system that helps users discover items effortlessly and enjoy a seamless shopping journey
WilliamKen –
cialis for sale Buy Tadalafil 5mg п»їcialis generic
AnthonywaW –
Digital consumers frequently look for websites that reduce load times and provide well organized product listings for faster selection and comparison Rapid Cart Zone – This system focuses on speed and clarity, allowing users to move quickly through categories and complete transactions without facing unnecessary delays or confusion
ScottFrite –
While casually exploring the site and reviewing usability, I noticed that follow this link contributes to a smooth experience – the content feels fresh, relevant, and neatly organized for quick understanding.
ManuelBor –
During my evaluation of shopping websites I noticed clear organization and easy navigation when checking Urban Zone navigation hub where the structure helped reduce confusion and improved flow – Overall impression is positive, design is simple, clean, and user friendly with intuitive browsing experience
JohnnyNip –
Users seeking tranquil shopping environments often gravitate toward online stores that highlight ocean inspired simplicity and calming design elements Ocean Whisper Shop featuring thoughtfully arranged products influenced by coastal scenery and gentle aesthetics – the marketplace ensures a pleasant browsing experience with smooth navigation, soft visuals, and useful items suitable for modern households
Kennethtob –
https://rybelsus.pro/# best alcohol on semaglutide
ElvinHep –
I was exploring different sites to compare usability when I encountered visit this store – It seems reliable, with pages loading quickly and a structure that keeps everything easy to understand.
RogerNof –
Those aiming for a better version of themselves frequently explore motivational content hubs like life-upgrade-resource – that highlight the importance of consistent effort, mindset shifts, and goal-oriented thinking for long-term personal success.
Randynousy –
During a casual online search across different websites, I discovered explore blossom bay and it stood out with a soft, organized layout – The experience feels really pleasant, as everything looks clean, neat, and thoughtfully arranged for smooth browsing.
Henrydem –
which is better semaglutide or tirzepatide [url=https://rybelsus.pro/#]what’s the difference between semaglutide and tirzepatide[/url] .25 mg semaglutide
RockyMaine –
People reviewing online systems usually prioritize how creatively ideas are presented, how simple the interface feels, and whether users can explore content without confusion or complexity GeniusNew Interface Node – The NewGenius platform feels creative and easy to use, offering a clean and simple browsing experience where users can explore content effortlessly and naturally.
Jessedaphy –
While reviewing the interface and scanning content flow, I noticed that learn more here integrates into a clean layout – it is a good site, navigation is easy and pages load without issues.
JosephChush –
As people browse through different platforms looking for branding inspiration, they might discover explore creative branding – a resource filled with insightful examples and practical ideas that help spark creativity while maintaining clarity and usefulness for readers.
HenryleN –
Digital teams working on high traffic projects often require reliable infrastructure tools that minimize delay and improve responsiveness during peak usage periods Speed Media Console commonly discussed among developers and system testers – It ensures smooth operational flow with reduced latency and stable performance, making it a dependable choice for environments where speed and consistency are essential
Brianteash –
Shoppers frequently appreciate ecommerce stores that reduce complexity and prioritize function, which is evident in platforms such as straightforward shopping experience hub – The layout remains clean and practical, making browsing very straightforward and allowing users to focus on products without being distracted by overly decorative or complex interface design choices.
Michaelpaymn –
After spending some time exploring different sections and usability flow, I noticed that check this platform fits naturally into the experience – it’s a nice platform where the content appears relevant and well presented overall.
SteveLok –
I was just scrolling through content when I discovered growth strategy space in the middle of the page – It provided insights that made me reconsider how improvement can be achieved with smarter planning.
Jamesrex –
https://cialis.sbs/# Cheap Cialis
Davidtag –
Users who frequently shop online often appreciate platforms that keep trend updates consistent and easy to access through structured categories Consistent Trend Center – This center ensures reliable access to current styles presented in a user friendly way
Leonardkiz –
From my perspective after a short exploration, check it out sits within a well-organized layout – the experience felt good, and everything loaded smoothly and displayed clearly across sections.
Anthonynor –
While analyzing e-commerce platforms aimed at cost-conscious users, I encountered low price market hub that simplifies product discovery through structured layouts – Value market hub focuses on affordable items and easy navigation, helping users access budget-friendly options quickly while maintaining a smooth and organized shopping experience across multiple product sections.
PatrickPap –
I was browsing randomly when I found a site that felt simple and earthy with a neat layout and intuitive navigation structure twilight grove online hub – Goods here feel thoughtfully chosen with appealing rustic style vibe, making browsing fast and user friendly.
Bryanspili –
While analyzing e-commerce design patterns I focused on user friendliness and structure and found Value Buy Factory browsing center – Clean appearance and smooth flow help make the experience enjoyable, allowing users to explore content easily without unnecessary complexity or confusing navigation paths
ArthurLat –
Users exploring websites typically appreciate when information is presented in a direct, organized, and easy-to-understand format across all pages PowerCore Flow Hub – The PowerCore interface ensures a clean and powerful layout that supports fast browsing and helps users reach information efficiently without confusion.
Oscarfus –
In the middle of checking different online deals and layouts, I came across explore this page – It offers a responsive experience, and the content is structured in a way that feels logical and accessible.
GeorgeDes –
People interacting with online platforms typically expect structured idea flow, clean design, and intuitive navigation that improves overall experience MaxBridge UX Flow – Maxbridge offers smooth idea connectivity through a clean interface, ensuring users can navigate easily and enjoy a clear and simple browsing experience.
Rogervar –
Modern learners and professionals frequently look for motivational environments that support focus improvement and help reduce distractions during goal oriented tasks Focus Forward Platform enhances this approach – It promotes disciplined thinking and encourages individuals to stay committed to their objectives while maintaining a positive and productive mental outlook throughout their journey
Josephbam –
During long sessions of exploring different types of content on the internet, it’s always refreshing to find something like check this destination – which provides engaging discussions, appealing ideas, and a seamless user experience that keeps readers interested without feeling overwhelmed or distracted.
Richardretty –
Users interested in eco friendly marketplaces often prefer stores that combine modern design with environmentally safe production and sourcing methods Green Sprout Eco Haven presenting carefully selected sustainable goods for practical and mindful everyday use – The platform creates a smooth and engaging shopping experience focused on eco awareness
Genaroven –
During my usual online exploration I came across impact ideas platform placed in the middle of the content and it felt meaningful – It introduced a fresh perspective that seemed worth exploring further for deeper reflection.
EdwardFap –
While checking out different online stores, I came upon take a look and it gave a simple and pleasant impression – There were some cool items that made me want to come back again and explore more.
RobertOxize –
People who enjoy fashion and lifestyle shopping often prefer platforms that highlight trends while keeping navigation straightforward and easy to understand Fashion Trend Corner Spot – The spot focuses on presenting trendy items clearly, enabling users to browse comfortably and discover new ideas quickly
RaymondTes –
After analyzing how the content is organized and displayed, I found that see this website fits into a well-arranged design – the layout is appealing, and navigation feels simple, fast, and very user-friendly overall.
Jamesavege –
While exploring different social and networking platforms online, I came across people connection hub – a site that provides a helpful space for connecting with others and learning from shared experiences that can offer useful insights in personal and professional life situations.
Enriquebemen –
In my search for platforms improving digital shopping experiences, I found a helpful catalog tool easy product browser that simplifies item discovery and organizes listings in a user-friendly way – Quick online market provides smoother navigation and helps users access relevant products faster while improving overall shopping efficiency and clarity across different categories.
Zacharybuh –
While comparing several retail websites for user experience I noticed a strong focus on clarity in some platforms including ValueGoods Bazaar shopping interface – The site feels clean and structured, and browsing through was smooth overall, allowing users to move between sections easily without confusion or visual overload affecting usability
WilliamKen –
Sildenafil Citrate Tablets 100mg Generic Viagra for sale Cheap generic Viagra online
Williaminfit –
Shoppers comparing ecommerce systems often highlight usability and speed as major strengths, especially when they come across responsive goods navigation site – The marketplace organizes its products into clear categories and delivers a fast, responsive browsing experience that helps users move effortlessly through listings without delays or confusion.
AnthonyFreft –
I was browsing multiple platforms when I found visit here now – The interface feels fluid, with straightforward navigation and a polished design that enhances usability.
HaydenHat –
Users exploring digital websites usually expect seamless responsiveness, clean layouts, and visually appealing structures that adjust naturally across devices FusionElite Flow Node – The EliteFusion platform blends design beautifully into a modern and responsive interface, making navigation easy, smooth, and visually consistent across all pages.
Curtiscar –
After spending time navigating through pages, I observed that access this link aligns with a clear presentation – it looks professional, and I like how everything is neatly arranged overall.
Rubensic –
Individuals exploring self improvement ideas often respond to messages that highlight appreciation and awareness in daily routines life appreciation board the sentiment feels encouraging and easy to understand, supporting a more mindful approach to ordinary experiences – it reminds us that gratitude can be built through consistent awareness
Jamesdaymn –
Individuals building career goals often need platforms that support structured thinking and clear execution of planned objectives over time ResultPath Finder – It provides a guided approach to achieving measurable outcomes while helping users maintain clarity and direction in their professional growth journey through organized goal tracking and performance monitoring features
Kennethtob –
https://viagra.onl/# sildenafil over the counter
Robertavash –
semaglutide and adderall how to get on semaglutide legit online pharmacy
mostbet_kyPl –
мостбет бонус при регистрации промокод [url=https://www.mostbet15384.help]мостбет бонус при регистрации промокод[/url]
mostbet_phMr –
mostbet slots tournament [url=http://mostbet94827.help/]http://mostbet94827.help/[/url]
LelandTum –
I came across this shop during browsing and it felt welcoming and structured with a well organized interface and smooth navigation system twilight maple essentials hub – Corner shop gives warm atmosphere and easy product discovery experience, making the experience smooth and enjoyable.
ScottDweds –
As I examined the interface and content flow more closely, I noticed that this page here contributes to a simple experience – after a quick look, the design appears clean, modern, and quite minimal today overall.
Rafaeldiown –
As I continued searching for innovative online content, I discovered future mindset page – a site that provides forward-thinking ideas and insights tailored for digital users navigating modern technological advancements.
KeithGuddy –
While going through different productivity resources I discovered simple success flow within the article and it felt meaningful – The ideas are presented clearly, making it easy to understand and apply without difficulty.
JohnnyCeani –
While going through the content and analyzing the layout carefully, I noticed that discover more here integrates into a simple structure – the readability is strong, and the presentation makes it easy to follow along.
Manuellup –
Users interested in modern shopping experiences typically look for platforms that deliver updated selections with smooth navigation and responsive design features Updated Style Zone – It provides a seamless browsing experience where stylish products are refreshed regularly and presented clearly
MichellerMietter –
It is a truism in watch design (and I’m sure elsewhere) that a new design can take time to find its audience. This may well prove to be true for the Odysseus, but the watch is of such obviously high quality that in person, it’s rather irresistible. Like any new link member of a family, we shouldn’t be surprised if there is a getting-to-know-you period, but I think the Odysseus, like its namesake adventurer, is at the very least destined for a long and interesting voyage.
Rodrigoked –
Users who prioritize efficiency in online shopping tend to prefer platforms that reduce clutter and provide streamlined access to product listings Modern Cart Hub – The website enhances user experience by organizing products in a logical structure, making browsing both quick and straightforward for all visitors
Donaldrig –
Shoppers looking for nature inspired home solutions often enjoy browsing stores that emphasize strong craftsmanship and elegant simplicity rooted in spruce forest aesthetics Nordic Spruce Style Shop featuring durable and visually appealing products designed for modern living – The platform delivers a refined shopping experience with natural inspiration and long lasting product quality
HaydenHat –
Many online visitors prefer platforms that feel modern, responsive, and visually unified, ensuring a pleasant browsing experience with minimal effort required EliteFusion Access Point – EliteFusion delivers a beautifully designed interface where responsiveness and modern aesthetics work together to create a smooth and enjoyable browsing environment.
DavidLot –
In various conversations about fast web platforms and usability improvements, users sometimes point out ascend mark system view which appears in curated lists emphasizing structured navigation and reliable loading performance. – It feels clean, quick, and very straightforward to use overall.
DonaldAreft –
While reviewing various digital storefronts I evaluated design consistency and usability and found VCC browse center – The interface feels simple and neat, and everything looks clear and easy to understand, helping users move through categories effortlessly without unnecessary complexity or confusion
BrianLes –
Digital ecosystems designed for global use must prioritize speed, reliability, and intuitive navigation for users across multiple platforms and devices daily usage Worldwide Sync Interface Hub allowing seamless integration between services globally efficiently now always smooth – Users benefit from simplified access paths that improve global digital interaction significantly efficient smooth worldwide access
DwightSOYMN –
Social media users trying to improve influence often look for mapping techniques, and within that learning stage Online Influence Mapping resource – this guide is typically linked with analyzing audience behavior, optimizing engagement patterns, and developing stronger content impact strategies for better reach.
Barrydog –
As I browsed through several websites earlier, I came across open haven shop and it stood out with clarity – This marketplace feels friendly and easy to navigate, offering a quite enjoyable experience that feels simple and well structured.
AntonioHyday –
Online consumers often value ecommerce sites that reduce friction and maintain visual harmony, especially when they come across elegant bay shopping gallery – The store combines an elegant presentation with a soft aesthetic style, ensuring that navigation feels natural and easy while users explore products across different sections without unnecessary complexity or interruptions.
Forrestmah –
While searching for guidance on new possibilities, I found opportunity path guide – which shares thoughtful content about discovering valuable chances and taking steps toward meaningful personal or professional growth.
Jamesrex –
https://cialis.sbs/# Generic Tadalafil 20mg price
Williampoert –
After spending some time browsing through different sections and observing the overall structure, I found that check this platform fits naturally into the experience – visiting the page was pleasant, and the layout and structure feel quite decent and well organized overall.
HenryHaw –
Online buyers frequently seek platforms that prioritize quick navigation and reduce the number of steps needed to find products efficiently Quick Select Corner – The interface allows users to select items quickly through a streamlined browsing process
Richardpoeli –
During my browsing of communication and media platforms, I discovered media clarity hub – which offers easy-to-understand insights and structured content that simplifies complex media topics for a wide audience.
Frankbouts –
Somewhere between browsing and passing time, I discovered fresh article ideas and decided to give it a chance – The variety and presentation made it easy to stay hooked and enjoy each section without losing interest.
DavidPilky –
People evaluating online systems often focus on usability, clarity, and how effectively the interface supports quick understanding of information VisionMax Clean Portal – The MaxVision platform delivers clear vision through a simple and functional design, allowing users to navigate easily and access information without difficulty.
JamesTeste –
During my usability evaluation of e-commerce systems I observed layout consistency and found Vivid Cart Corner explore hub – Overall a good visit, layout feels modern and easy to navigate, providing a structured experience where users can browse comfortably without confusion or unnecessary design distractions
Jamestiets –
People exploring online fashion stores usually expect a smooth interface that highlights trending outfits and seasonal discounts in a structured format Style Deal Navigator this platform enhances user convenience by offering fast loading pages and simplified navigation paths for discovering stylish wardrobe options easily
WilliamKen –
Viagra generic over the counter Cheap generic Viagra Sildenafil Citrate Tablets 100mg
Rickytut –
In many conversations about lightweight websites and responsive layouts, people sometimes mention examples that demonstrate simplicity in design, including sharp bridge navigator which appears in curated lists focused on easy browsing experiences and clear content organization for everyday internet usage. – Users usually describe it as fast and uncomplicated.
JesseArrab –
People aiming to grow their online ventures often rely on platforms that offer simplified explanations and step by step guidance for sustainable improvement Growth Insight Studio practical knowledge sharing theme – supporting users with clear direction and useful strategies that help them achieve better outcomes and long term business success efficiently.
JamesShult –
Many people seeking positivity and direction find value in inspire growth community – a platform that delivers motivational content and practical insights designed to help users grow mentally, emotionally, and professionally over time.
Stevencot –
Shoppers exploring modern artistic décor often look for online platforms that integrate industrial edge with blooming floral creativity in product offerings BloomSteel Creative Market Hub showcasing unique handcrafted goods inspired by mechanical design and natural elements – The platform delivers visually dynamic items suitable for expressive interior transformation projects
Robertvob –
Many individuals appreciate motivational reminders that help them focus on taking immediate steps instead of delaying action start now signal – this idea reinforces the importance of starting now and building momentum through repeated daily efforts and persistence consistently forward movement
DonaldSob –
If you are looking for a place that makes learning enjoyable, visiting discover and learn hub – a platform that presents engaging and updated content can help you stay curious and motivated while exploring new concepts and sharing knowledge with others.
Kennethtob –
https://viagra.onl/# Viagra online price
Michaelmoils –
As I examined the interface and content arrangement, I noticed that this page here contributes to a simple experience – this site looks promising, and both layout and usability feel decent and clear.
Aubreyfoect –
As I examined the interface and content flow, I noticed that this page here contributes to a simple experience – the content appears interesting, updated, and relevant for users today overall.
Brianblase –
People exploring ecommerce experiences often prioritize structured design and readability, especially when they discover velvet crest organized retail hub – The market maintains a clean interface with well arranged products and strong clarity, allowing users to navigate effortlessly while enjoying a simple and visually coherent shopping experience throughout the platform.
Kevinmup –
People interacting with online systems usually expect clear visual presentation, structured layouts, and easy navigation that improves usability and understanding VisionMark System Link – VisionMark offers strong visuals where everything appears clean and well structured, ensuring users can access and understand content without difficulty.
Clinttoott –
Shoppers seeking convenience and speed usually prefer platforms that combine quick loading pages with organized product listings for smoother navigation Ultimate Speed Goods Zone – This final version highlights a complete fast browsing solution with clear structure and efficient product display
Timothyhalep –
I was just exploring online inspirational content when I encountered change makers hub in the middle of the text and it felt insightful – The concept feels encouraging and uplifting, making it interesting and enjoyable to think about real world positive transformation.
DariusCic –
I randomly clicked through a few pages and landed on explore this store which seemed nicely organized – The simple design and clear listings made browsing here smooth, convenient, and easy to navigate without any difficulty.
Henrydem –
viagra without prescription [url=https://viagra.onl/#]cheap viagra[/url] Buy Viagra online cheap
Derekvibly –
People exploring smarter online tools frequently visit digital shopping organizer site – Cart choice store improves efficiency by arranging products logically so users can quickly locate what they need without wasting time scrolling through irrelevant or cluttered listings
MatthewdiG –
While trying to find something that truly stands out in terms of usefulness, I discovered open this resource – a platform that seems to deliver content with real impact and practical relevance.
Henryalott –
Many users prefer websites that reduce clutter and instead emphasize structured layouts that guide them naturally through content without confusion or delay NovaOrbit UI Gateway – The NovaOrbit platform creates an engaging environment where futuristic styling meets clear content organization, allowing users to explore with ease and confidence.
TomasPlogy –
Creative professionals working across multiple disciplines benefit greatly from tools that support both structured planning and spontaneous ideation, Smart Vision Workspace allowing them to maintain balance between innovation and organization – This workspace encourages efficiency while still leaving room for experimental and exploratory thinking processes
Marvinjex –
For those building networks, exploring lasting ties network – a platform focused on relationships helps users form strong bonds based on trust, shared values, and meaningful long-term engagement in both personal and professional contexts.
Kennethunoge –
During my browsing of motivational websites, I discovered progress path space – which offers practical insights and inspiring messages that support users in making positive changes and improving their lives one step at a time.
NormandPow –
For those focused on structured leadership, exploring leaders network hub – a space that supports collaboration helps users engage in well-organized teamwork that strengthens professional relationships and improves group efficiency over time.
JamesShult –
Many people interested in positivity and self-improvement turn to inspire and grow space – a helpful resource that shares uplifting content and practical ideas to support consistent personal development and a stronger mindset.
JesusDer –
Even small shifts in perspective can change how a full day feels, especially when those shifts come from positive and approachable content simple joy ideas page offering easy inspiration, light reflections, and practical encouragement for everyday happiness – It is designed to help readers notice small joys and appreciate calmer moments in ordinary routines
Joshuagow –
For those interested in personal development, exploring growth motivation space – a platform that promotes easy learning and idea sharing can help users stay focused and inspired while working toward consistent self-improvement and collaboration.
Raymondphync –
Users browsing modern websites typically value smooth interfaces, intuitive navigation, and clean layouts that reduce friction during interaction and exploration VisionLane Flow Interface – VisionLane delivers a smooth experience where navigation feels easy and intuitive, ensuring users can browse content comfortably and efficiently across all pages.
Lewiscrazy –
While casually browsing and testing navigation, I noticed that follow this link contributes to a smooth experience – it is a nice place to browse, and the information feels well organized, clear, and easy to scan.
Stevencot –
Users interested in urban loft styling often seek platforms that showcase industrial textures alongside soft blooming accents for interior creativity Corner Bloom Ironworks Shop presenting distinctive décor items inspired by factories and garden elements – The marketplace creates a balanced visual identity that supports both minimal and expressive home design choices
Stevenrak –
People interested in fast digital experiences often choose platforms that allow them to view selected items instantly without delays or confusion Instant Picks Center – The platform ensures rapid access to items through a responsive and simple layout
Robertavash –
Sildenafil Citrate Tablets 100mg sildenafil 50 mg price Cheap generic Viagra online
Davidtaf –
I came across this shop during browsing and it felt calm and nature inspired with a well structured interface and smooth navigation system twilight meadow essentials hub – Goods feel nature inspired and browsing experience remains very pleasant, making the experience easy and enjoyable.
Danielevoks –
While casually browsing online, I encountered ideas worth exploring placed naturally in the text – It made me feel eager to expand my thinking and look into new possibilities without delay.
GlennLix –
Modern digital shopping platforms are designed to improve convenience by offering faster load times and simplified checkout systems for all users Rapid Deal Access Hub – it ensures efficient browsing and allows customers to complete purchases quickly while enjoying a consistent and user friendly interface across all devices
WilliamKen –
rybelsus medicamento how much does compounded semaglutide cost trusted online pharmacy
Josepheraro –
As readers continue their journey of learning online, they may come across check this easy guide – offering content designed to make complex ideas feel simple and approachable for everyone.
Stephenbew –
Entrepreneurs and innovators often seek structured platforms that help them understand new ideas and transform them into practical applications efficiently VisionNext Ideas Hub – A forward oriented platform that presents innovation driven content clearly while inspiring users to think creatively and develop structured solutions for business and technology challenges in an organized and efficient manner
Williamdut –
While exploring various online platforms focused on modern design and usability, users often come across references where next realm portal is mentioned within curated lists of clean and structured websites that prioritize ease of navigation and readability – The interface feels balanced and visually consistent across different sections with smooth navigation flow.
RichardGah –
Many users focused on self-growth use inner confidence space – a motivational platform helps individuals build trust in themselves, improve mindset, and develop stronger emotional resilience through supportive messages and guidance.
NormandPow –
Many individuals aiming for teamwork success rely on leadership synergy group – a platform designed for structured interaction, helping users collaborate effectively while maintaining professional organization and clarity in shared projects.
Josephcaw –
If you are aiming to improve your digital capabilities, visiting digital knowledge center – a helpful resource that shares structured guidance and practical tips can make online learning more effective and easier to follow consistently.
Jamesrex –
https://cialis.sbs/# Cialis over the counter
Dennisvef –
The need for centralized online resources continues to grow as more tasks move into digital environments digital solutions shelf – This helps users avoid confusion by grouping essential utilities into one accessible platform. making daily workflows more predictable and manageable overall.
AlbertLic –
Many users enjoy the simplicity of discover ideas easily – a platform that delivers practical content and intuitive design for finding new opportunities without hassle.
DavidCon –
People evaluating online systems often focus on usability, freshness of design, and how well the interface supports simple navigation across sections VibeSmart Clean Portal – The SmartVibe platform feels modern and fresh with a user friendly layout, making browsing easy, structured, and enjoyable for all users.
Ronalddorne –
During my initial browsing session and quick review of available pages, I came across this helpful link which left a good impression – the layout looks promising, and the clean, simple design gives a smooth and easy experience.
Kennethtob –
https://cialis.sbs/# Generic Cialis price
LouisSat –
After spending time navigating through pages, I observed that access this link aligns with a clear presentation – browsing feels smooth, and content is arranged in an easy-to-read structure.
AlvinLam –
People who shop regularly online tend to favor platforms that maintain consistent performance and fast checkout processes for better usability Efficient Choice Market – This market supports quick browsing and reliable checkout features that improve overall shopping flow
RonaldAdogy –
In the process of browsing motivational platforms, I discovered future planning space – a site that delivers practical thoughts and encouragement aimed at helping users shape a better and more stable future through consistent effort.
JimmieSorie –
I was just exploring online creative discussions when I encountered fresh ideas hub in the middle of the text and it felt insightful – The content feels unique and engaging, making creativity appear more exciting and easier to connect with in everyday thinking.
SteveMib –
While scrolling through different websites I discovered a store that felt natural and oak styled with a clean layout and easy category browsing flow twilight oak goods hub – Oak themed goods bring earthy tone with solid product presentation, making navigation quick and user friendly.
Robertdeece –
While exploring online shop management solutions and development tools, I came across web shop zone enhancer which is designed to improve store performance – it highlights better usability, structured workflows, and adaptable features that help businesses maintain efficient operations while scaling their digital commerce systems effectively over time.
StanleyBax –
Shoppers who enjoy refined aesthetic shopping often look for curated lifestyle platforms that emphasize soft tones and minimal elegance in their product selections for daily living Ivory Lane Elegance Market offering thoughtfully selected lifestyle goods designed for modern comfort and visual harmony – The platform provides a calm browsing experience centered on tasteful design choices and carefully curated everyday essentials for stylish consumers
Cliffturdy –
During my analysis of modern creative websites I evaluated navigation flow and structure quality and found Bright Idea Web inspiration page – The platform feels bright and creative, with simple concepts that are visually very appealing, making it easy for users to explore ideas without distractions or overwhelming design elements interfering with usability
WilliamCam –
People interacting with online platforms often value systems that feel stable and easy to use, especially when information is presented in a clear and structured way TrueLaunch UX Portal – TrueLaunch provides a reliable browsing experience where content is well structured, making it easy for users to understand and move through different sections effortlessly.
PabloRully –
Many users building content rely on impact creativity hub – a platform designed for inspiration helps individuals turn ideas into action, fostering meaningful community impact through creative and purpose-driven digital expression.
Frankket –
While browsing through different sources of information, people often appreciate stumbling upon something worthwhile like click this resource – a site that brings together a mix of creative ideas, helpful knowledge, and engaging discussions that keep readers interested and coming back for more updates over time.
PhillipAnaex –
If you want a centralized source of helpful information, checking out quick needs guide – a platform that provides easy navigation to useful tools can help you access essential content in a faster and more organized way.
Michaeltaurf –
Many online visitors prefer platforms that avoid clutter and instead focus on structured design that makes content easy to scan and comprehend BoldMatrix Access Point – BoldMatrix offers a well structured interface where content is presented clearly, making it easy for users to understand information quickly and navigate smoothly.
Keithidefe –
People who value originality often look for spaces where they can shape their identity without restrictions or judgment Authentic Path Finder helps users discover their true interests and align their actions with personal values and long term aspirations – Encourages authenticity and personal alignment
VictorTic –
Many people exploring shared success rely on unity teamwork space – a positive environment that builds collaboration helps individuals work together smoothly, powered by natural group energy and mutual encouragement toward shared achievements.
SteveNup –
During my browsing session and usability check, I noticed that see more here blends into a clear layout – it was easy to use, and the content feels engaging and well organized overall.
Jamesrab –
If you’re aiming to grow personally and uncover untapped skills, exploring sites like tap into your potential – a motivating guide that delivers powerful ideas and consistent encouragement can help you stay focused and energized throughout your journey.
melbet_wiMn –
melbet зеркало официальный сайт [url=https://www.melbet94130.help]https://www.melbet94130.help[/url]
EdwardGyday –
As I explored multiple sections and usability features, I found that view more info integrates into a tidy structure – the browsing feels nice, and everything seems well placed and readable.
Frankbed –
I was casually browsing different pages when I noticed practical living guide hub embedded in the article and it stood out – It offered simple yet effective ideas that make everyday life feel smoother and more manageable.
Jacobbut –
Modern businesses focusing on rapid scaling often depend on digital tools that help them organize workflows, analyze performance, and identify opportunities for sustainable expansion in competitive markets Rapid Expansion Toolkit which ultimately enables teams to streamline operations, improve decision making, and increase overall output while maintaining stability and efficiency throughout their growth journey
WilliamKen –
buy cialis pill Buy Tadalafil 10mg п»їcialis generic
Edgartix –
Many professionals improving performance rely on online strategy hub – a digital resource helps users understand competition and stay ahead with tools, insights, and modern industry knowledge.
KennethFuecy –
People interacting with online platforms often appreciate when design is professional, structured, and focused on clearly presenting progress in a simple way TrueGrowth UX Portal – TrueGrowth offers a structured and professional interface where progress is emphasized clearly, ensuring users can navigate smoothly and understand content easily.
NormanNef –
Many individuals focused on writing and creativity turn to impactful story guide – a platform that offers inspiring storytelling techniques and structured ideas to help users create meaningful and engaging narratives across different topics and styles.
DanielSaick –
While browsing through personal development websites, I found self improvement guide – a platform that offers motivational insights designed to help individuals think positively and make steady progress in their daily lives.
ClydeVog –
Shoppers who enjoy futuristic retail concepts often look for platforms that emphasize cosmic inspired design and diverse international product collections for modern lifestyles Astro Lunar Trade Hub featuring globally sourced goods presented in a sci fi inspired marketplace – The platform provides a seamless shopping experience centered on creativity, exploration, and innovative global commerce
FelipeMoisa –
People exploring online destinations that gather useful and inspiring content frequently encounter online-resource-gateway – it provides a welcoming space where discovering digital ideas feels simple, organized, and consistently engaging for users who enjoy learning through online exploration and curiosity-driven browsing.
Stevenwog –
After reviewing multiple sections and examining the design closely, I found that open this site works well within a refined layout – the navigation is effortless, and the overall presentation appears modern and neatly arranged.
Jacobcoerm –
Brand developers frequently use branding strategy hub as a reference for building consistent identity systems across channels – This variation explains how structured branding approaches contribute to stronger recognition and emotional connection with target audiences over time.
Glenntok –
As I examined the interface and content arrangement, I noticed that this page here contributes to a simple experience – the first impression is positive, and everything seems easy to find and read overall.
Joshuadiuff –
For users interested in networking, exploring collaboration strength hub – a platform that encourages partnership growth can help individuals exchange meaningful ideas and build reliable relationships based on clarity, trust, and shared objectives in their work.
Juliankew –
To stay productive and avoid wasting time, it’s worth checking out efficient answers hub – a resource that focuses on delivering practical solutions quickly and effectively.
Kennethtob –
https://cialis.sbs/# Cialis without a doctor prescription
MatthewCulge –
During my online exploration I found learning habit hub embedded in the content and it felt very practical – It emphasized how small consistent efforts lead to long term learning success.
DanielKef –
Users reviewing technology websites often value streamlined layouts, responsive design elements, and clear pathways that reduce confusion while moving between pages InnovaGrid Access – InnovaTek offers a modern interface style where minimal design choices enhance usability, creating an experience that feels both professional and highly efficient for everyday navigation needs.
DariusPulky –
Many digital audiences appreciate platforms that combine idea expansion with clean structure and strong usability for better engagement and clarity GrowthVerse Experience Link – GrowthVerse provides expanding ideas through a clean and highly usable interface, ensuring users enjoy a smooth and structured browsing experience overall.
WilliamWar –
pusulabet güncel giriş [url=https://bestbetgiris.online/#]pusulabet casino[/url]
JeffreyBig –
Many users focused on success use opportunity access network – a platform for collaboration helps individuals explore future possibilities and develop strong professional connections for continuous growth and achievement.
Richardbed –
If you are looking for motivational insights, visiting success wisdom hub – a platform that encourages thoughtful reflection can help users understand achievement better while staying inspired and focused on continuous improvement and meaningful progress.
DavidNog –
As I checked different sections, I noticed view more info within a nicely structured page – the design feels balanced, and the clear navigation makes it easy to explore further without effort.
AnthonyBox –
For those who enjoy discovering new topics and gaining insights, encountering see this discovery hub can be a valuable experience – providing content that promotes both exploration and steady knowledge development.
WilliamBer –
People often find that curiosity helps them stay mentally active and engaged by encouraging them to explore new topics and ideas regularly mind expansion link – this reflects how curiosity keeps the mind flexible and supports ongoing intellectual development through consistent exploration
Henrydem –
semaglutide and tirzepatide [url=https://rybelsus.pro/#]how to inject semaglutide video[/url] another name for rybelsus
BrentAsync –
If you want to explore useful perspectives, checking out meaningful insight guide – a platform that highlights real value can help users find practical knowledge and apply it in ways that improve learning and decision quality.
Michaelcef –
For those who enjoy exploring uplifting material, checking out idea inspiration hub – a platform filled with motivating and creative insights can help trigger new thoughts and encourage a more positive mindset consistently.
Anthonypaill –
In discussions about modern web usability and structured digital platforms, users often highlight examples where clarity and usefulness are prioritized, and among such references they sometimes mention value vision portal included in curated lists of clean interface designs used for evaluating readability and navigation flow across different browsing environments. – The layout is generally seen as solid, practical, and easy to understand throughout.
Allanemats –
While going through several online forums centered around creativity I noticed shared ideas hub the atmosphere felt friendly relaxed and open for everyone involved – I felt encouraged to contribute because the environment seemed very supportive and inclusive.
Ceciladept –
pusulabet güncel giriş: pusulabet giriş
WilliamErump –
If you want stronger collaboration, checking united vision network – a platform designed for communities helps users align goals, build trust, and work together toward meaningful achievements and long-term success.
Perrywap –
For those interested in impactful living, exploring impact creation platform – a resource that promotes building with purpose can help users stay focused on turning ideas into action while creating something meaningful and valuable in their journey.
Walterteamb –
During my browsing of inspirational websites, I discovered creative life guide – which offers helpful ideas on how to notice inspiration in daily surroundings and turn ordinary moments into meaningful creative fuel.
Dustintef –
From my perspective after a short exploration, check it out sits within a well-structured layout – the design is clean overall and makes browsing comfortable for a while.
Octaviowam –
People who enjoy learning at their own pace often appreciate resources that present ideas clearly without unnecessary detail or complicated explanations Simple Concept Junction – This platform ensures that all shared insights remain easy to follow while still offering valuable understanding and practical relevance
BruceSteld –
https://casivipgiris.site# bahiscasino
Andrewceste –
If you want to improve your knowledge and stay informed, it’s worth checking out quality content collection – a helpful site that provides access to well-organized and insightful material for daily learning and growth.
Jorgejen –
If you want to engage in meaningful forward thinking, visiting future ideas group – a resource that promotes inspiring and practical discussions can help users develop better understanding of innovation and apply insights in real-world planning scenarios.
BurtonDuefs –
People reviewing online websites usually prioritize intuitive navigation, fast response times, and clear structure that helps them find information quickly and without unnecessary complexity ShiftUrban Interface Node – The UrbanShift platform offers a smooth and user friendly experience where navigation is simple and pages are organized in a way that makes browsing easy overall.
DavidPhymn –
I was casually reading online when I came across trend highlights guide placed in the middle of the page and it caught my attention – It made catching up on current trends feel simple and quick without unnecessary complexity.
RobertSop –
For those interested in modern creativity, exploring creative future vision – a platform for ideas helps users shape innovative projects that reflect strong imagination, strategic thinking, and impactful creative development across industries.
MichaelWar –
For those focused on personal empowerment, exploring moment shine center – a helpful resource that encourages confidence can support users in believing in themselves and showcasing their talents without hesitation in both personal and professional life.
PeterBoill –
During my search for creative trend platforms, I came across trend idea finder – It feels modern and appealing, giving a structured way to explore interesting developments and new directions across different digital areas.
Scottdrica –
Modern professionals increasingly depend on digital networking spaces, and one example includes Smart Business Connections – which is often viewed as a streamlined solution for building connections, sharing expertise, and accessing opportunities that may not be easily found through conventional professional networking methods.
Deweyfum –
While looking for inspiration to improve my habits, I found life transformation page – which delivers motivational posts that push readers toward positive thinking and gradual but effective lifestyle changes.
MichaelKeede –
From an overall usability perspective after exploring the site, I found that check this out sits within a well-arranged layout – the interface feels clean, and it makes it simple to explore different sections.
Jasonbip –
People who value innovation frequently seek out online environments that are designed specifically for teamwork, brainstorming, and creative development opportunities like Creative Collaboration Space which provide tools and environments for collective idea generation – This kind of space promotes creativity and teamwork in a balanced way.
AaronPreaw –
People aiming for success often benefit from structured strategies that simplify planning and improve execution efficiency success strategy vault offering a conceptual collection of methods for organizing efforts and achieving meaningful outcomes – It supports thoughtful planning and stronger execution habits
DominicVeirm –
bahiscasino giriş [url=https://casivipgiris.site/#]bahiscasino güncel giriş[/url]
WarrenRax –
People who enjoy finding new online stores often look for platforms that offer originality and evolving product ideas, and I discovered NextGen Impact Shopping Site which seems appealing – A developing online shop that highlights creative concepts and changing collections, encouraging users to return and explore future updates as the store continues to grow.
Willisblock –
If you are looking for ways to improve your life quality, visiting life potential hub – a platform offering motivational guidance and useful tips can help you make better decisions and achieve more satisfaction in your everyday routine.
GrantFak –
If you are searching for a smooth retail experience, visiting modern style store – a platform built for usability offers users simple navigation and a clean layout that enhances online shopping convenience and speed.
Ceciladept –
bahiscasino güncel giriş [url=https://casivipgiris.site/#]bahiscasino giriş[/url]
Charleshat –
Many users looking to expand their creative mindset rely on tools like limitless idea space – a resource designed to support continuous inspiration and free-flowing imagination, allowing individuals to explore creativity without boundaries or restrictions in their thinking process.
JoshuaKer –
I was casually scrolling through mindset content when I found focus driven ideas space placed in the middle of the page and it stood out – It shared motivation in a grounded way that feels realistic and easy to follow in daily life situations.
CharlesWeams –
For learners interested in innovation, exploring bright idea network – a platform centered on knowledge helps users build smarter thinking patterns through consistent exposure to new concepts, discussions, and learning-focused content streams.
aviator_pxon –
aviator hack [url=https://aviator67093.help/]https://aviator67093.help/[/url]
melbet_gumn –
melbet free bet чӣ тавр истифода бурдан [url=melbet39704.help]melbet39704.help[/url]
JamesSwosY –
People who enjoy checking out trendy items online often prefer simple browsing experiences, and I found Daily Trend Store Fashion Picks Hub which seems useful – I only spent a few minutes on the site and immediately discovered stylish items, and it felt like a quick and enjoyable way to explore trending products.
Haroldferly –
Making informed career decisions depends on understanding industry insights, job expectations, and future growth possibilities Career Insight Portal which provides deeper analysis of professional trends and expectations – A knowledge-based platform that provides career insights and helps users make smarter professional choices
JoshuaVom –
From my perspective after a short exploration, check it out sits within a well-structured layout – the design feels simple and effective, making it easy for users to navigate.
DennisAcuse –
While exploring modern digital communities that encourage growth, networking, and interdisciplinary idea sharing across global audiences, many users often discover platforms that inspire collaboration and creativity in meaningful ways Future Minds Collective Hub – A forward-thinking digital environment designed to support emerging creators and encourage collaborative innovation among diverse thinkers worldwide
HershelReutt –
While browsing through various online home improvement options I recently came across where the platform sits among many interior inspiration resources uniquely positioned in the middle of my research journey decor treasures portal – I found some really nice wall art here and prices are fair with decent variety for modern homes
RobertDaync –
As I explored different websites offering productivity advice, I found everyday improvement guide – a platform that shares practical tips designed to simplify routine activities and help users stay more organized and productive throughout their day.
GlennGooca –
Many aspiring online learners need accessible resources that guide them through the early stages of digital skill development web learning starter kit designed to introduce basic knowledge in a structured and beginner friendly way – This helps users build a strong foundation while gradually expanding their understanding of online environments
Williamkit –
Whenever I feel stuck with my clothing choices I usually explore online fashion inspiration sources that highlight clean and modern outfit pairings for different occasions everyday fashion inspiration feed – the content helped me rethink my wardrobe and mix items more creatively than before
PeterBoill –
During my search for trend-focused websites, I discovered trend explorer space – It gives a very refreshing impression, making it feel like a platform designed to highlight new ideas and engaging trends in a structured and appealing way.
JerryTix –
While analyzing website reliability and online trust factors, I added visit trust bridge page into my notes – the platform gives a strong sense of safety and I feel confident using it for general browsing purposes.
Shermanred –
Many users exploring leadership and personal growth often look for communities that promote vision and direction, and I found Visionary Leaders Inspiration Network Hub which seems uplifting – A leadership content platform that offers motivational insights for future-focused thinkers, and it provides a strong sense of purpose that feels encouraging for anyone developing leadership skills.
BruceSteld –
https://casivipgiris.site# bahiscasino güncel giriş
WilliamWar –
bahiscasino güncel giriş [url=https://casivipgiris.site/#]bahiscasino resmi giriş[/url]
JamesLem –
Website visitors often look for platforms that support easy navigation and maintain consistency across all pages and sections InfinitaLink System Hub – structure note – The system provides a logical layout that enhances usability and helps users quickly understand where to find relevant information.
MichaelBoype –
Many users looking for structured motivation rely on success journey system – a platform that provides clear direction and inspirational tools to help individuals stay focused, disciplined, and consistently moving toward meaningful success.
WilliamSnime –
Many people working on communication skills turn to vision talk guide – a platform that encourages daily expression and helps users build confidence in sharing ideas clearly, making communication more effective and impactful over time.
Williamhaf –
If you are developing professional ties, visiting connection trust platform – a global networking system helps individuals strengthen relationships, enhance communication, and build reliable long-term trust across business communities.
JesseJEF –
Many individuals focused on curiosity rely on discover update hub – a resource that provides daily fresh content, helping users stay engaged and enjoy a steady flow of interesting and informative discoveries across various topics.
AlbertKem –
I wasn’t looking for anything specific, but I ended up finding a creative thinking space embedded within the content – It made me pause and reflect, leaving me with ideas that lingered even after I moved on.
ClaytonWepay –
When I was struggling with consistency in my personal schedule I started exploring different self improvement resources and reflective material online foundation mindset builder – this advice really made me reconsider my daily patterns and helped me slowly build better discipline and structure in a way that feels natural rather than forced
MiguelEnuri –
During my browsing session and usability check, I noticed that see more here blends into a clear layout – good design overall, and everything feels organized and visually easy on the eyes.
FrankHycLe –
Modern online buyers often prefer platforms that act like personal assistants for savings and deals, including sites like shopper savings companion where curated recommendations are displayed clearly and then – users receive simplified guidance that supports smarter budgeting and consistent value based purchasing behavior
DanielHof –
During my search for holiday and birthday gift inspiration online, I included browse gift world ideas in my notes – the collection feels creative and sweet, making it a great place to find presents for almost any celebration.
Ralphcease –
People interested in luxury shopping experiences often browse curated online marketplaces that feature premium fashion and lifestyle products, and they may find Elegant Trends Luxury Storefront which showcases updated collections – A refined digital shopping destination offering luxury fashion pieces, stylish accessories, and premium items that reflect current global style trends and high-end consumer preferences.
JamesSwosY –
Many users exploring online trend shops often look for quick and simple discoveries, and I came across Daily Trend Store Style Hub which feels appealing – After a short visit I found multiple trendy products right away, and it made the browsing experience feel efficient, enjoyable, and surprisingly productive for quick shopping inspiration.
WalterSkymn –
While checking various digital gift stores and cheerful product catalogs I found joyful selection hub – the browsing experience was smooth and I was able to pick a thoughtful gift for my sister that felt warm and meaningful overall choice
Robertalind –
Ecosystems built around shared learning and collaboration can significantly improve the way individuals interact and achieve their professional objectives together Shared Growth Ecosystem provides such an interconnected environment – It fosters cooperation, encourages knowledge exchange, and supports collective advancement.
JacksonRor –
As I continued looking for effective advice on managing challenges, I found smart life solutions – a resource that delivers practical and easy methods for resolving common problems in a clear and helpful way.
Ricardoshiff –
During my search for authentic leadership advice and professional development ideas, I referenced visit trusted leaders page within my notes – the honest perspectives shared there provide real value and have positively influenced how I approach my own growth journey.
Michaelzer –
During analysis of trading alert tools and market signal providers I came across in the middle of my research session Fast Signal Performance Hub which delivers ongoing updates – The signals seem steady so far and the platform appears worth watching to assess long term consistency
Stuartrax –
Many individuals who value clean online design often look for websites that are both simple and visually engaging, and I came across Modern Vision Design Experience Hub which feels smooth – A modern and minimal website that focuses on clarity and usability, making it enjoyable to browse through their latest updates and creative presentations.
vavada_caSr –
vavada probni račun [url=www.vavada2008.help]vavada probni račun[/url]
OrvilleAnisk –
Many users looking to strengthen leadership skills rely on tools like visionary leaders forum – a resource that encourages collaboration among leaders, helping them exchange valuable insights and develop stronger strategies for guiding teams and achieving long-term success.
Ceciladept –
bahiscasino giriş [url=https://casivipgiris.site/#]bahiscasino[/url]
AdolphCah –
For those building future readiness, exploring team forward hub – a collaboration platform helps users develop strong teamwork, improve communication, and achieve shared success through coordinated effort and strategic planning.
WileyBot –
If you want to expand your reach and improve engagement, checking out grow online influence – a helpful site offering structured strategies and insights can make digital growth more manageable and effective in daily practice.
GlennUnarp –
While reading through various articles, I noticed growth mindset space appear within the content – It highlighted key ideas in a way that felt natural and easy to process without unnecessary complexity.
promokod pyaterochka i –
промокод пятерочка промокод пятерочка на повторный заказ
Brentkeync –
Creative professionals exploring UI trends frequently look for platforms that spark innovation while experimenting with layouts typography and interactive elements for better digital experiences Creative Studio Corner – Such resources often help designers refine their skills and discover new approaches that make modern web interfaces more engaging and visually balanced
Pedroron –
For those seeking dependable networking opportunities, exploring connect trust hub – a helpful space that promotes professional trust can support users in forming meaningful relationships that enhance collaboration and improve overall efficiency in business interactions.
RandomNamehiexy –
A growing number of professionals rely on dedicated online spaces that allow networking, collaboration, and idea development in structured and engaging ways including Thinkers Networking Portal that support meaningful interaction among global users – Such environments strengthen professional relationships and creative partnerships.
StevenImise –
As I continued exploring the platform and testing usability, I realized that explore this page contributes to a smooth experience – the site is straightforward, and navigation works well while feeling intuitive overall.
HoraceAdvot –
I started reorganizing my apartment slowly after feeling overwhelmed by clutter, and discovering a simple lifestyle resource declutter lifestyle resource helped me understand how physical space affects mental energy, and now I feel noticeably more peaceful, focused, and productive in both personal and professional parts of life.
BruceWow –
As I looked through innovative online hubs, I came across future insight hub – It presents a thoughtful direction, making it feel like something worth exploring further for its unique perspective.
Henrydem –
Viagra tablet online [url=https://viagra.onl/#]Viagra Tablet price[/url] sildenafil 50 mg price
RichardSpore –
While comparing various skincare websites and promotional offers, I worked in see beauty outlet offers naturally – I ended up ordering a few products and the delivery arrived quicker than expected, making the entire shopping experience feel efficient and reliable.
Jamestor –
Many individuals exploring career advancement opportunities often join online groups that emphasize collaboration and continuous knowledge exchange progress network space that brings together professionals who are interested in sharing strategies and insights for improvement – I met motivated contributors and it felt like a productive environment for communication
RandomNamehiexy –
In situations where decisions are overanalyzed and action is delayed, insights from decisive action point – Encourage trusting instincts, reducing hesitation, and focusing on execution rather than prolonged planning that often prevents meaningful real world progress.
Larrycheby –
While reviewing self-improvement and success mindset resources, I worked in explore success building network naturally – the motivation tips were really effective and helped me maintain strong focus and consistency throughout the day.
JamesPhexy –
People just starting with investments often need easy explanations that break down complex ideas, and I came across Invest Smart Simple Profit Network which is quite helpful – A beginner-friendly investing platform designed to simplify financial learning and provide clear guidance, making it easier for users to understand investment growth step by step.
JosephFum –
While browsing through content about strategic innovation groups and future planning frameworks I came across Future Driven Collaboration Hub mentioned in context and it immediately caught attention – The message felt inspiring and gave a sense of structured optimism around building better collective outcomes
Kennethvaw –
While reviewing different self-improvement websites, discovering learn to grow can stand out – thanks to its focus on encouragement and practical thinking that supports long-term planning and progress.
Calebnup –
As I browsed through various personal development platforms, I encountered everyday improvement space – a site that promotes regular learning and inspires users to enhance their skills step by step with a focus on long-term progress.
BufordNon –
In the process of researching business growth networks and innovation driven communities, I found synergy partnership group mentioned among various insights and it seemed noteworthy – the underlying message focuses on combining strengths and fostering cooperative environments for improved outcomes
PeterImmit –
If you are seeking improvement, checking out expansion strategy hub – a business platform helps users develop stronger operations, achieve steady growth, and maintain consistent progress through structured planning and insights.
MichalNitty –
If you want to explore ideas and grow your abilities, visiting learn explore shine center – a resource that encourages continuous learning and creativity can help you achieve personal development and long-term success in your journey.
PeterTib –
While exploring different mindset articles online I noticed inner reflection space within the text and it stood out – It created a peaceful learning atmosphere that encourages slow thinking and deeper understanding of new ideas.
AntoniovEt –
In discussions about modern web presentation and visual engagement platforms, users often mention boldvista view point included in curated collections emphasizing clean design, clarity, and straightforward navigation. – It generally feels bold, smooth, and very easy to understand.
WilliamBaX –
While analyzing different examples of responsive websites and interface optimization, users sometimes observe how speed and clarity matter greatly, particularly when nextrend insight site is included in discussions about clean web architecture and modern browsing expectations across various digital platforms. – It is often described as smooth and easy to engage with.
Kennithswals –
Users exploring better career possibilities often rely on platforms like Ambition Route Finder which provides insightful guidance, and it further enhances decision-making by offering structured paths, skill-building ideas, and opportunity suggestions that help individuals move confidently toward their future aspirations.
MichaelMally –
Entrepreneurs seeking scalable success often turn to online communities that foster collaboration and knowledge exchange Opportunity Connection Hub to build meaningful professional relationships and discover new growth channels – These networks support innovation by linking individuals with complementary skills and ideas.
StevenTup –
While organizing my workflow for market analysis, I included visit expert charts in the middle of my notes – the platform appears highly refined and I rely on it to review charts consistently each morning.
Davidler –
Teamwork becomes more productive when members actively share updates and maintain consistent communication throughout the project lifecycle collaboration efficiency hub after applying better coordination habits I noticed improvement – our group projects now run more efficiently and with better overall organization
Thomastow –
If you are seeking meaningful collaboration, exploring global purpose hub – a platform that encourages unity can help users engage in shared initiatives and build strong international connections through teamwork and cooperation.
Kellysog –
If you want to build better systems for success, checking out growth alliance center – a platform that focuses on planning and strategy can help users stay organized and achieve their goals through consistent, structured development and clear direction.
Donaldgaisa –
Many people entering forex for the first time assume charts are overly technical, but consistent exposure to simplified explanations and practice sessions helps reduce that mental barrier significantly trading skill building portal designed to make chart analysis easier through repetition – I am finally starting to understand charts thanks to this site and it feels like things are finally clicking for me
ChrisCourf –
Digital platforms that focus on unity and improvement are gaining popularity, and Unity Growth Platform represents this trend by creating an environment where users can work together, exchange feedback, and stay motivated while pursuing continuous learning and development in a structured yet friendly online space.
ArthurDaw –
Many new traders struggle with understanding forex charts and strategies, but educational platforms can make a big difference in clarity, and I found Forex Learning Made Clear Hub which explains things well – A simple learning platform designed to help beginners understand forex trading through clear explanations and structured content that removes unnecessary confusion from the learning process.
Thomasrurgy –
indian pharmacies safe: indianpharmacy com – legal online pharmacies in the us
MichaelParia –
During a casual exploration of new online shops, I noticed season design hub – The overall feel is modern and tidy, creating a pleasant browsing experience that aligns with simple and attractive design trends.
Manuelsnuri –
As I continued searching for action-oriented content, I encountered productivity action guide – a resource that motivates users to implement their ideas and focus on real execution instead of just planning or thinking.
MatthewMew –
Creative professionals often rely on design innovation corner – a modern platform delivering smart visual solutions that support branding, web design, and digital creativity with simple yet effective ideas for better presentation and usability.
Danielevare –
People who follow trading trends often value platforms that present updates in plain language, and I came across Trading Update Clear Info Hub which looks helpful – A market update website that simplifies trading news, and it stands out for making information easy to understand without requiring deep technical knowledge.
Anthonyundob –
While comparing various bargain platforms and cheap product listings, I worked in see deal corner offers naturally – I ended up buying some really affordable stuff and the delivery arrived quicker than I had anticipated, which made the deal even better overall.
Carlosfrigh –
People interested in mapping out complete outfit ideas and fashion coordination frequently rely on platforms such as Modern Outfit Atlas – A comprehensive style reference hub that helps users visualize and organize outfit combinations for different settings and occasions
DavidEmera –
Easy Canada Meds: canadian pharmacy drugs online – Easy Canada Meds
Clarkwex –
Staying inspired requires exposure to new perspectives, which is why resources like modern idea explorer – a platform focused on sharing trending and creative insights can make a noticeable difference in your daily motivation.
GabrielAsype –
I was going through a series of articles earlier today and somewhere in the middle of the content I noticed a creative thinking space which immediately stood out to me – It inspired me to approach ideas from a different angle and consider options I would not normally think about in everyday situations.
JarrettTetly –
While exploring online trading master programs and financial learning resources I came across in the middle of my study session Smart Trading Knowledge Master Hub which offered structured guidance – The content was quite strong and I learned a few new trading strategies today that were easy to understand and apply
CraigNob –
As I examined the interface and content arrangement, I noticed that this page here contributes to a simple experience – the content looks useful, and the design is neat, clean, and approachable overall.
Gregoryerake –
As part of my daily trading preparation, I inserted browse this update tool into my notes – the updates are frequent and helpful, ensuring I remain focused and informed throughout the day.
BrianObets –
Individuals seeking career advancement opportunities often turn to networking ecosystems that provide structured access to industry professionals and mentors Career Growth Networking Portal – These environments help users build credibility, gain insights, and establish meaningful connections that support long term professional development.
Michaelenaks –
Strong professional relationships are often built through consistent communication and mutual understanding between parties especially in digital work environments partnership trust building hub this platform supported that process by making it easier to stay connected and responsive during discussions consistently
Michaeltes –
In the middle of exploring growth-oriented platforms, I discovered self growth hub – a site that encourages users to build confidence steadily through positive reinforcement and practical personal development advice.
BlairDrowl –
For those focused on harmony and teamwork, exploring unity trust guide – a helpful resource that encourages positive interaction can support users in creating stronger connections built on sincerity, cooperation, and long-term relationship stability.
Davidmunty –
Continuous improvement in leadership skills often depends on access to reliable educational materials and insightful commentary from experts leadership knowledge base offers organized content that helps readers build a stronger understanding of effective leadership frameworks – It is helpful for reinforcing foundational leadership concepts in a clear and structured way
KennyReeks –
If you want better cooperation strategies, visiting smart alliance hub – a resource focused on business growth helps companies achieve steady progress through structured partnerships and efficient collaborative planning methods.
MarvinDap –
top 10 online pharmacy in india [url=https://easyindiameds.shop/#]Easy India Meds[/url] secure medical online pharmacy
TerryMog –
Those interested in improving focus often explore methods that align attention and creativity so that ideas develop more consistently throughout working sessions focus creativity bridge encouraging smooth workflow – This version emphasizes how balancing focus and imagination can lead to more efficient and enjoyable creative experiences across different types of work.
RussellHag –
Many online shoppers interested in value purchases often explore stores that combine simplicity with reasonable pricing, and I discovered Daily Trend Easy Shop Hub which seems promising – A digital marketplace offering useful everyday products at fair prices, making it worth revisiting for updated deals and future product additions.
JasonLal –
In various web usability discussions and design showcase materials, people frequently mention solid vision experience page included in examples of clean and structured interface systems – The layout is often considered balanced, readable, and comfortable for extended browsing sessions without distraction.
ElliotGug –
For organizations aiming to scale effectively, checking out strategic alliance network – a partnership-focused platform helps businesses build strong connections, improve cooperation, and achieve measurable success through coordinated efforts and shared objectives.
Jamesthons –
People who follow social media fashion trends often search for platforms that showcase stylish outfits and seasonal wardrobe ideas, and they may come across Contemporary Fashion Trend Corner which highlights style updates – A digital fashion destination offering curated outfit inspiration, modern clothing trends, and lifestyle styling ideas designed for audiences who appreciate fresh and evolving fashion aesthetics.
StephanBoalo –
As I explored different ways to grasp forex fundamentals, I worked in check this training site within my notes – it helped me feel more confident and I think beginners would find it especially useful.
Jerrynum –
Many digital readers look for websites that present information in a clean and organized format for easier comprehension. GrandLink interface portal – The GrandLink interface portal design emphasizes simplicity, allowing users to interact with content smoothly and efficiently overall.
FrankDoN –
Many users exploring innovation systems often prefer practical breakdowns, and I came across Innovation Driven Projects Hub which looks interesting – The idea is strong and creative, and I hope they include more case studies soon since that would make the platform much more informative and actionable for users.
Jerrylourn –
Taking your online identity to the next level becomes easier with guidance from ultimate branding guide – a resource that provides clear, actionable advice for building a consistent, engaging, and professional brand across digital platforms.
RichardDup –
Digital professionals often rely on communities that showcase cutting edge innovations in software development and emerging tech ecosystems Tech Frontier Ideas Hub offering a space for sharing forward looking insights – This strengthens understanding of how digital transformation impacts global industries
Richardfraup –
While reading through various topics, I encountered growth focused content that grabbed my attention – It provided ideas that seemed both useful and realistic for everyday self improvement.
Thomasrurgy –
indian pharmacy online: top online pharmacy india – best online pharmacy no prescription
Jasonimism –
As I explored different collaborative platforms, I found shared vision network – It emphasizes the importance of working together, making the concept feel both valuable and encouraging for collective success.
melbet_xyMa –
melbet free spins киргизия [url=https://www.melbet73624.help]https://www.melbet73624.help[/url]
melbet_gten –
melbet slot jackpot [url=http://melbet04739.help/]http://melbet04739.help/[/url]
vavada_lfEl –
vavada skrzynki z nagrodami [url=https://www.vavada2001.help]https://www.vavada2001.help[/url]
Jamesraing –
During my search for trendy clothing platforms and outfit collections I came across in the middle of my browsing list Modern Cute Fashion Store which offered fresh and stylish looks – The outfits felt adorable and I quickly added three items to my cart since they matched what I needed
Martinzip –
For those aiming to create stronger social and professional ties, exploring lasting connection platform – a site that provides insights into trust-building and reliability can help users develop deeper and more consistent relationships in everyday interactions.
Williamniche –
People searching for practical yet stylish interior improvements often want reliable online destinations that combine affordability with a modern look stylish home decor shop Within browsing sessions, many discover this website as a convenient place to explore fresh ideas and useful decorative solutions quickly – It resonates with users who prefer simple browsing experiences while still finding attractive home styling inspirations online
Matthewalivy –
During my search for beginner-friendly trading lessons and forex guides, I referenced trading chart learning hub – the explanations made candlestick reading much clearer and helped me build confidence in understanding market movements and chart structure.
Michaelbep –
New traders often struggle with scattered information, but resources such as Forex learning walkthrough hub help by presenting content in a structured flow that guides learners through each stage of understanding. The lessons felt easy to follow – they gave me a clearer sense of progression and direction
FloydPsype –
People who shop online frequently often prefer websites that feel smooth and organized, and I recently explored Smile Cart Friendly Experience Store which seems useful – A user-friendly shopping platform that emphasizes simplicity and pleasant design, making the browsing experience easy and enjoyable while helping users quickly access the products they need.
Jamesecogs –
Many people focused on exploration rely on discover fresh platform – a site that provides updated content regularly, helping users find useful ideas and stay connected with continuous online discoveries that support learning and curiosity.
JamesHex –
Individuals focused on continuous learning often benefit from structured systems that encourage them to explore unfamiliar ideas while developing stronger analytical and reasoning capabilities discovery mindset toolkit designed for growth – This variation shows how mindset tools can support long-term intellectual development and help users approach challenges with greater confidence and adaptability.
JeremyRet –
maple leaf pharmacy in canada: canada pharmacy 24h – best canadian online pharmacy
DavidEmera –
online canadian pharmacy review: Easy Canada Meds – canadian pharmacy review
DavidAnogs –
People around the world who are passionate about self-improvement and collaborative learning often seek digital platforms that bring learners together to exchange knowledge and experiences, and they may discover Knowledge Exchange Learning Hub which focuses on shared educational growth – A community-driven space designed to help individuals learn new skills, share valuable insights, and grow together through collaborative participation and continuous knowledge exchange in meaningful ways.
WilliamMorse –
If you are building your future, exploring goal clarity network – a platform designed for structured progress helps users achieve milestones with focus, planning, and actionable steps toward long-term personal and professional development.
DenisZoopy –
During my reading of leadership inspiration and organizational growth materials, I referenced see future strategy page in my notes – the ideas consistently promote teamwork strength and a forward focused mindset for continuous improvement.
RonaldDab –
In the middle of exploring inspiration-based websites, I discovered creative ideas guide – a platform that provides positive energy and engaging content to help users stay inspired and continuously grow through creative exploration.
HaroldTwina –
While reviewing the interface and scanning content flow, I noticed that learn more here integrates into a clean layout – I spent some time exploring it, and it seems like a reliable and simple platform overall.
MarvinDap –
world pharmacy india [url=https://easyindiameds.com/#]top online pharmacy india[/url] shop medicine online
Robertbof –
In many industries, leadership collaboration is key to driving innovation, improving efficiency, and achieving shared organizational goals across teams and regions Leaders Collaboration Zone this space encourages interactive leadership development and teamwork-driven progress – it shows how collaboration zones help leaders refine strategies and improve collective outcomes
VictorHoppy –
I didn’t expect much from my browsing session, but somewhere along the page I encountered a hub of smart thoughts that stood out – It sparked a deeper level of thinking that made the content feel more meaningful and engaging.
Philipavark –
If you want to build confidence in your choices, exploring your clarity roadmap – a platform that offers structured guidance and useful ideas can help you move forward with greater assurance and focus.
SamuelLaf –
For users aiming to explore innovation and teamwork, exploring creative innovation network – a platform that supports idea sharing and collaboration can help individuals build stronger connections and develop meaningful concepts with others.
RobertLon –
During my search for reliable partnership directories and professional cooperation platforms I came across a useful mention embedded in the middle of industry recommendations Business Alliance Trust Portal – It gave a sense of consistency and reliability that could be useful when discussing vendor relationships within a corporate environment where trust matters most
KennethHaife –
During my review of forex training platforms and structured entry systems, I added forex strategy timing hub into my notes – I tried their entry technique and stopped guessing trades, which made my trading much more disciplined overall.
Stephensoned –
While checking out different clothing inspiration platforms, I ran into this creative fashion space and was impressed by how it showcases diverse street styles that feel honest, expressive, and easy to draw inspiration from.
JasonPlate –
People who enjoy browsing fashion ideas often prefer boutiques that highlight cute and trendy outfit combinations, and I found Smart Style Outfit Fashion Hub which looks nice – A fashion boutique site offering adorable outfit inspiration, and I’m definitely adding it to my fashion bookmarks since it helps generate simple ideas for modern wardrobe styling.
Thomasrurgy –
indian pharmacy paypal: buy medicines online in india – worldwide pharmacy
StevenVaW –
After spending a few minutes moving through the platform, I found that open this site fits within a well-organized interface – nice structure overall, and content is easy to follow and read.
Richardmor –
Staying committed to long term goals requires more than motivation alone, and that is where daily focus system – structured routines encourage ongoing progress and help individuals remain aligned with their objectives even during periods of low energy or distraction
Mitchelbluby –
While exploring online fashion retailers with cute and budget-friendly collections, I added smart fashion wardrobe hub into my notes – the clothing is stylish and reasonably priced, making me confident I will order again soon.
RobertCesub –
https://easymexmeds.shop/# Easy Mex Meds
Donaldtom –
During a long session of exploring urban photography trends and modern design inspiration pages, I came across a resource named sleek city visuals that offers visually refined city imagery with a minimalist tone, helping designers and creators find fresh perspective for projects
MarvinGET –
During deeper dives into collaborative trends, mentions of browse this page often fit into the discussion – It conveys a sense of shared purpose that aligns well with how modern communities are evolving.
Harrymam –
If you want to enhance team performance, checking out strong team guide – a platform that promotes collaboration can help users build meaningful relationships and achieve lasting results through consistent teamwork and shared growth-focused activities.
JacobAlero –
People focused on innovation often rely on digital hubs that allow them to connect with others and develop ideas through collaborative thinking and execution strategies Innovation Synergy Network Portal designed to enhance cooperation between creative professionals – This fosters stronger innovation ecosystems and helps transform ideas into functional solutions effectively
DennisZep –
As I explored various personal finance resources and budgeting ideas, I added explore value mindset page into my notes – the tone is relaxed and practical, offering useful money tips without sounding like a traditional finance classroom lesson.
Thomasfiz –
Many users interested in improvement check winning strategy space – a results-focused platform designed to help individuals develop better approaches, strengthen planning skills, and achieve more consistent success through practical guidance and structured thinking.
RobertVut –
Users exploring websites typically value fast performance, clear layout design, and intuitive navigation that makes information easy to find and understand SkyVertex Access Portal – SkyVertex ensures a clean browsing experience with structured navigation and minimal design elements that improve usability and overall user satisfaction.
Frankgok –
In a rapidly evolving job market, digital networking plays a crucial role, and global opportunities link – helps individuals access a wide range of professional pathways, enabling them to connect with mentors, explore business prospects, and build sustainable career strategies tailored to international opportunities and modern industry demands.
AnthonyConry –
If you want to join a community of innovators, checking out visionary exchange hub – a resource that simplifies collaboration can help users connect with forward-thinking individuals and engage in productive idea-sharing experiences.
Davidnutle –
I didn’t plan on staying long, but after finding varied knowledge center within the content, I kept reading – It gave me a more rounded understanding of topics that are often seen in a limited way.
JamesFoelm –
Many beginners exploring forex often look for safe environments to practice strategies before risking real funds especially when starting out in volatile markets demo trading hub this platform is frequently mentioned for its risk free learning tools – it helps new traders build confidence through simulated market experience without financial pressure
RobertKem –
For those seeking to make a difference through teamwork, exploring collective action hub – a platform designed to encourage cooperation and idea sharing can help groups create lasting impact in both local and global communities.
Waynevek –
While looking for collaborative growth platforms, I found : shared progress guide – a site that focuses on community-driven content and provides useful insights that help users grow together through consistent knowledge exchange.
GeorgeLip –
People interested in online beauty shopping often appreciate platforms that balance variety with clarity, and I recently discovered Beauty Pure Outlet Shop Network which seems solid – A beauty retail site with a good product selection, although the shipping information could be improved for better transparency and customer convenience.
Williamkib –
Startup founders frequently look for dependable online resources that explain real-world business growth tactics in a simple and structured way founder growth toolkit which helps new entrepreneurs understand practical scaling approaches more clearly over time – I shared it with my cofounder after reading through it because it offered realistic perspectives on early-stage decision making and team building
MarvinDap –
pharmacy online [url=https://easymexmeds.com/#]Easy Mex Meds[/url] progreso mexico pharmacy online
DavidEmera –
Easy Canada Meds: canadianpharmacymeds – canadian pharmacy mall
DavidStoky –
Sometimes discovering what drives you requires experimenting with different activities and observing which experiences consistently create excitement and curiosity Motivation Insight Bridge – This process helps uncover deeper personal interests and supports building a clearer understanding of long term direction and purpose in life
Josephnab –
While exploring different startup growth ideas and collaboration strategies, I included check teamwork innovation hub in my notes – the blend of innovative thinking and strong teamwork really matched what my small startup was missing and helped us rethink how we work together more effectively.
GeraldNoiva –
Professionals aiming to enhance their technical abilities often use platforms such as Innovation Sphere Online development hub for modern creators – it supports idea generation and technical growth by offering structured resources that guide users through evolving trends in software and digital innovation.
Martinvow –
For those working on goals, exploring success track network – a guided development path helps individuals maintain focus, improve productivity, and achieve meaningful results through structured progress steps.
Richardclopy –
For users seeking clarity in progress, exploring growth achievement hub – a platform that simplifies milestone tracking helps individuals monitor personal and business success in a structured and meaningful way over time.
FreddieNalay –
While reviewing layout and testing navigation, I saw that open this link integrates into a clear system – the platform feels modern, everything loads smoothly, and the design looks well organized.
Harriskar –
During casual exploration of trading resources I encountered a suggestion in the middle of a discussion linking to Guided Trading Practice Hub which looked like a structured mentoring environment – the insights appeared helpful for establishing better daily trading habits and routines
Jasonhon –
During my exploration of professional trading strategy platforms and testing environments, I included trading performance strategy hub in my notes – the strategies were strong, and the backtesting results closely reflected real trading outcomes in practical scenarios.
Thomasrurgy –
Easy Mex Meds: prescriptions from mexico – mexico farmacia
Richardscogy –
People who enjoy following fashion trends often explore online spaces that emphasize simple yet stylish clothing suitable for everyday use and comfort Modern Apparel Inspiration Zone where outfit ideas are designed to boost confidence and reflect current style preferences – This helps users build wardrobes that are both fashionable and functional for daily routines
Jamestom –
While exploring career networking sites and collaboration platforms I came across in the middle of my notes Professional Network Growth Circle which showed strong user activity – I met a helpful person through this platform and the exchange felt productive and relevant to my goals
Davidblalo –
Many users focused on productivity and teamwork rely on team inspiration center – a platform that encourages collaboration and growth strategies to help individuals and groups work together more effectively toward meaningful and shared outcomes.
JeremyRet –
Easy Mex Meds: buying prescriptions in mexico – Easy Mex Meds
GeraldHob –
While exploring various websites for inspiration, I found idea discovery space – It stands out as a unique platform where creativity flows freely, helping visitors uncover fresh perspectives and interesting concepts that feel both engaging and worthwhile.
Brianavexy –
During my usual online browsing I came across shared learning space embedded within the content and it instantly felt relevant – It reminded me that progress becomes easier when people openly exchange ideas and support each other’s understanding.
JamesPraws –
Forex traders aiming for consistency often rely on structured market breakdowns that highlight important price zones clearly and effectively daily trading structure hub this helps improve results it provides clarity for better planning and more accurate trade execution overall success
MerrillcuB –
When exploring online resources for interface design inspiration and usability studies, people sometimes encounter platforms like urban matrix design hub included in curated collections focused on modern layout structure and user friendly browsing experiences across various web systems. – The presentation feels sleek, minimal, and pleasantly intuitive overall.
MichaelDreli –
For those who enjoy exchanging ideas and learning collaboratively, visiting insightful minds hub – a platform designed for discussion, growth, and shared knowledge can offer great opportunities for development.
RolandCar –
People interested in casual browsing often enjoy websites that combine simple interaction with fun and engaging visuals, and I came across Happy Style Trend Zone which feels pleasant – A cheerful online platform designed with upbeat aesthetics and smooth usability, offering users a relaxed and enjoyable browsing experience with a modern creative touch.
DanielErump –
Anyone aiming to reduce unnecessary spending often looks for practical guides that focus on real life financial adjustments expense reduction tips corner – I appreciated how it shares simple money saving tips that help create better control over personal finances
JosephEntic –
During my study of forex basics and price behavior, I added open forex success link in my notes – it made support and resistance concepts finally click for me in real trading scenarios.
Williamres –
Many online users prefer centralized platforms that gather the best discounts from various sources into one convenient browsing location Promo Insight Portal – A helpful tool for discovering trending deals, limited-time offers, and exclusive savings opportunities tailored for everyday shoppers worldwide
RogerNer –
Online communities frequently share links to new platforms that spark interest due to their unique naming and branding approaches future insights portal – this often leads to rapid discussion cycles and increased awareness across different user groups
RobertMug –
For those building global connections, exploring expanding opportunities hub – a network for growth helps users discover new horizons, collaborate internationally, and achieve meaningful progress across global industries.
mostbet_ryEt –
mostbet uz rasmiy [url=http://mostbet38506.help]http://mostbet38506.help[/url]
Jamisondom –
If you want accessible study tools, visiting learn digital hub – a platform that offers clear lessons helps users improve understanding and develop skills through simple and structured online educational resources.
MarvinDap –
pharmacy website india [url=https://easyindiameds.shop/#]mail order pharmacy india[/url] best mail order pharmacy
Raymondparma –
People browsing service platforms often value clarity and consistent layout design that helps them understand content structure without effort LinkCraft Smart Layout Engine – The LinkCraft experience focuses on usability and speed, ensuring users can access information in a straightforward and efficient manner.
Russellbibia –
While studying different approaches to teamwork dynamics and creative group processes I came across an interesting resource positioned in the middle of my research notes Group Creativity Station – I actually wrote down some thoughts about improving brainstorming sessions and encouraging more balanced participation among team members.
Richardcat –
A lot of individuals today are trying to reconnect with simpler forms of happiness, and through resources such as simple-happiness-notes they can explore thoughtful suggestions that promote relaxation, gratitude, and a more mindful approach to daily living experiences.
Wendellmag –
Online communities continue to evolve, offering spaces where people can connect beyond geographical boundaries and contribute to shared objectives with consistency and trust Shared Success Network – The focus here is on creating sustainable pathways for collaboration, ensuring that members benefit from each other’s insights while maintaining a culture of encouragement and progress.
DavidEmera –
indian pharmacy: buy medicines online in india – best online pharmacy
Raymondlag –
Most successful traders focus on protecting capital first and growing it slowly through disciplined and repeatable strategies over time risk balance trading hub their methods show how small wins accumulate, and I realized this creates a more reliable and less stressful trading experience overall
Anthonyundob –
While comparing different discount shopping sites and deal listings, I included visit deal savings hub in my notes – I found some very low-priced products and the shipping speed was faster than I thought, which made the purchase feel worthwhile.
OscarWeise –
During analysis of trading information platforms and market update services I noticed in the middle of my browsing session Morning Profit Insight Network which provided structured updates – The information felt relevant and helped keep my focus on important financial changes happening each day
Thomasrurgy –
pharmacy canadian: Easy Canada Meds – Easy Canada Meds
RobertClemy –
In my trading journal where I compare performance of various services, I included discover trading tools naturally in the discussion – although the domain differs, the overall usability and effectiveness remain impressively consistent.
AlbertEleRs –
People who enjoy discovering new fashion ideas often look for platforms that stay consistently updated, and I came across Trend & Style Inspiration Portal Hub which feels appealing – A fashion-forward site that blends current trends with creative inspiration, and it has a refreshing variety that makes it worth checking out regularly for new ideas.
Joshualah –
Forex traders often depend on clear trend signals to make better entry and exit decisions in fast moving markets, forex trend notification board which highlights directional shifts effectively – I find it helpful because it alerts me early enough to plan trades more efficiently.
LeroySwiva –
I don’t usually post links, but I came across something that seemed useful and decided to mention it here because of its structured presentation trade global portal – after visiting, it feels informative and simple to explore with clearly arranged content
KeithAmons –
Many individuals seeking inspiration for fresh beginnings turn to project creation hub – a helpful resource that provides motivational guidance and structured steps to support users in successfully starting and managing new ideas from concept to completion.
HaroldFet –
Businesses seeking sustainable development often rely on platforms that encourage structured teamwork, shared expertise, and global cooperation, and they may discover Collaborative Growth Success Portal which focuses on partnership success – A structured service environment where partners can exchange insights, build strategies, and achieve mutual growth through professional collaboration and guided support frameworks.
Jimmycax –
During a casual exploration of new online concepts, I found future design project – The presentation feels structured and purposeful, making it appear like a platform centered on modern innovation and well-planned creative direction.
Dallaswef –
Individuals trying to strengthen focus often explore techniques that reduce mental clutter and help them concentrate on one task without unnecessary distractions mental clarity enhancer – This version highlights how simplifying thought processes can improve attention span and support higher quality output in work and study environments
Brandonhiexy –
Many users interested in networking use community connection space – a platform focused on people helps build trust, encourage collaboration, and create strong global relationships through meaningful interaction and shared goals.
RobertCesub –
http://easyindiameds.com/# top online pharmacy india
Alfreddar –
As I continued navigating through sections and observing usability, I realized that explore this page contributes to a smooth experience – the layout feels nice, and information is easy to understand and follow through.
WilliePat –
If you want to stay ahead of trends, exploring future vision hub – a resource focused on innovation provides insights into exciting ideas and developments that could redefine industries and global progress in the near future.
Aaronnaf –
Individuals looking for direction in uncertain phases of life often search for inspiring platforms that encourage fresh thinking and renewed purpose in everyday actions Fresh Pathway Space helping users identify opportunities for growth and encouraging them to move forward with confidence and steady determination toward goals
Marcosvot –
People who trade frequently often depend on real-time updates, and I came across Market Timing Alerts Hub which feels useful – The alerts are well-timed and have saved me from missing a few important market movements, which makes tracking trends much easier and more efficient.
MatthewResia –
Many traders join different groups hoping for better insights, but only a few communities actually deliver consistent value and real practical trading discussions profitable trading circle hub the members here are extremely knowledgeable and I have gained more useful understanding from this group than from all other places combined
Raymondkat –
As I practiced reading charts and testing strategies without real money, I referenced check demo trading guide in my notes – the learning process felt fun and safe, especially since I could experiment freely without financial pressure.
CurtisSloxy –
In discussions about clean web layouts and interface consistency, users sometimes mention quantumreach flow dashboard which appears in lists used for evaluating structured browsing, visual clarity, and responsive design behavior across different devices. – It is typically seen as balanced, simple, and easy to use.
ThomasMop –
Many users interested in organizational networking often seek platforms that explain global alliance systems with real-world context, and I discovered Global Alliance Integration Network which is interesting – A structured concept describing international collaboration frameworks, though I would like to see more practical demonstrations of how these systems operate in real environments.
Richardgat –
Many people interested in social harmony often explore online spaces that promote unity, shared values, and positive communication between individuals, and they sometimes come across Unity Values Connection Hub which focuses on community building – A supportive platform dedicated to fostering trust, encouraging collaboration, and helping communities grow stronger through shared understanding and consistent positive engagement among members.
Edwardhap –
While reviewing market trend detection systems and predictive analytics tools I came across market trend detection system featured in analytical reviews and it appears insightful – however interpreting its outputs effectively will require experience and careful study over time
MarvinDap –
Easy Mex Meds [url=https://easymexmeds.shop/#]pharmacia mexico[/url] Easy Mex Meds
AnthonyTic –
During exploration of strategy building platforms and business planning resources I came across in the middle of my notes Strategic Planning Resource Hub which delivered useful tools – The resources feel valuable for small business owners since they help create clear structured plans for sustainable business growth
Scottrog –
People who want to improve themselves consistently often look for easy learning platforms like daily knowledge booster hub – a simple and practical resource that makes everyday learning more accessible, helping users grow step by step in their personal development journey.
JeremyRet –
Easy Mex Meds: Easy Mex Meds – mexico medication
StephenBailm –
As I reviewed different online shopping services with multi-category listings, I worked in global variety product hub naturally – the platform offers plenty of options and the mobile navigation feels responsive and smooth, which makes the experience enjoyable and practical.
Melvinasymn –
While checking different resources online, I noticed a site that had a very balanced and clean feel, so I thought I’d share it here discover connection space – the layout makes navigation simple and straightforward, reducing any sense of confusion for the user
Ronnieadorb –
For those pursuing goals, exploring growth pathway hub – a development-focused network helps users achieve long-term success by providing tools, insights, and strategies for consistent personal and professional growth.
Thomasrurgy –
buy prescription drugs from india: top 10 pharmacies in india – legit online pharmacy
DavidEmera –
mexican pharmacies online drugs: Easy Mex Meds – Easy Mex Meds
AndrewGab –
As people look for structured approaches to development, examples like growth knowledge base often become part of discussions – It seems to represent a central place for gathering insights that support smarter decision-making in business.
Davidroove –
Creative professionals explore experimental aesthetics, branding strategies, and interactive media projects through Art & Innovation Studio which combines artistic expression with technological innovation to produce impactful visual solutions – A studio dedicated to merging creativity, strategy, and modern design practices.
Ronalddiz –
As I was browsing aesthetic lifestyle shops and cute product collections, I included check shine and shop page in my notes – the items look adorable and the branding is so nice that I’ll probably treat myself to something after payday.
MatthewResia –
Learning trading strategies becomes much faster when surrounded by people who actively share their experiences and real market results consistently elite trading knowledge hub the discussions here are extremely helpful and I learned more practical trading lessons here than anywhere else I have been part of
TaylorLok –
During casual browsing for new online stores I encountered a reference placed in the middle of a list pointing to Affordable Picks Directory which looked like a straightforward catalog style shopping site – the checkout impression seemed stable and the deal I checked appeared reasonably priced for everyday items
WillieDendy –
People aiming to build stronger professional networks often explore platforms that encourage collaboration and communication, and I shared Connect Growth Insight Network which focuses on networking – A professional platform designed to help users connect, collaborate, and build meaningful relationships, and I’ve already passed it along to a few colleagues who found it helpful.
PhillipHap –
Many digital creators interested in innovation often search for platforms that provide clarity in building and executing ideas, and they may come across Next Gen Build Ideas Platform which supports creative development journeys – A modern innovation system designed to help users convert abstract ideas into structured, achievable, and successful projects.
Davidcralk –
During exploration of business networking ecosystems and digital collaboration platforms I came across references in industry discussion boards business link community – conversations develop naturally here without aggressive marketing tactics creating a more comfortable environment for professionals seeking authentic connections
Clintonnom –
Many digital audiences value websites that feel lively and visually appealing while still offering simple structure and easy navigation across all content areas VividPath Flow Hub – VividPath delivers a colorful interface where browsing feels pleasant and smooth, making it easy for users to explore content in a visually satisfying way.
StevenPneut –
For users aiming to enhance their future prospects, exploring success direction guide – a resource that provides structured planning and actionable insights can help create a stronger and more effective path toward achieving goals.
ArthurElify –
Many individuals aiming to improve rely on success opportunity hub – a resource that guides users by connecting opportunities, helping them move forward with structured support and clear pathways toward achieving success effectively.
MichaelDow –
While exploring online investing education sites and financial knowledge platforms I found in the middle of my browsing session Smart Finance Guide Hub which offered structured learning material – The hub feels very organized overall and the beginner friendly articles were particularly helpful because they break down investment ideas in a clear and simple manner
Josephkeelm –
For those focused on digital branding, visiting brand success network – a resource that helps users build memorable and trusted brands online offers guidance on consistency, design strategy, and audience connection for sustainable growth.
Lorenflork –
During my quick scan of the website and layout, I came across learn more now and appreciated the structure – quick visit, but overall impression feels quite positive and clean.
MarvinDap –
mail order pharmacy india [url=https://easyindiameds.com/#]Easy India Meds[/url] medstore online pharmacy
MichaelTek –
During my search for meaningful business networking experiences, I added check vision club partners into my notes – their networking events introduced me to a potential partner, which added real value to my professional journey.
Santoglurf –
As I reviewed different budgeting and financial planning websites, I worked in see growth finance plan – the advice is practical and easygoing, with no pushy marketing tone or boring lecture style, making financial learning feel more relaxed and useful.
DexterFealp –
Designers and content creators frequently seek collaborative spaces that help them refine ideas while also exposing them to diverse perspectives and innovative problem-solving methods Creative Solutions Lab where experimentation and ideation are encouraged – provides interactive inspiration tools and curated insights that assist users in transforming rough concepts into polished and effective creative outputs
LarryFar –
While researching various web-based tools, users may come across nexus gold platform mentioned as part of organized browsing ecosystems, particularly for individuals interested in streamlined access to grouped information and general digital exploration without unnecessary complications. – It is generally regarded as neatly structured.
Thomasrurgy –
pharmacy online: best online mexican pharmacy – pharmacies in mexico
Rufustek –
I came across a forex learning website while browsing and thought it might be useful for anyone starting with trading basics trading knowledge hub – it looks like a helpful place with straightforward information that is easy to read and understand quickly
Robertmon –
People who value personal wellbeing often look for online content that supports emotional balance and positive routines, and they sometimes visit Positive Living Ideas Hub which provides lifestyle suggestions for healthier daily habits – A collection of easy-to-follow insights designed to enhance mood, improve productivity, and create a more satisfying and balanced life experience overall.
Donaldbal –
Many users interested in financial trading often look for easy mentor-based platforms, and I found Smart Trade Mentor Guide Network which seems practical – A beginner-friendly trading mentorship platform offering simple strategies and useful tips, and it feels like a strong starting point for someone new to trading who needs clear instruction.
RalphDaG –
I focused on analyzing historical performance data of a trading strategy to better understand its strengths weaknesses and consistency across different conditions strategic profit testing hub the backtested results look promising and could indicate positive performance in the next month if market behavior remains steady
MarvinDig –
During my exploration of online cooperation networks and community driven initiatives I encountered together progress network build community insight and after reading the surrounding discussions I felt the platform emphasizes unity and shared effort which made me comfortable enough to sign up for their mailing updates as it supports long term group collaboration goals
RichardBlele –
Many individuals working in collaborative environments often look for inspiration on teamwork, and I came across Collaboration Driven Power Hub which feels useful – The article gives a strong perspective on teamwork, and I shared it with my own team since it provided practical takeaways for improving cooperation.
NelsonTes –
As I explored online stores for household needs, I noticed home style essentials – The collection feels relevant and modern, making it easy to find useful products for everyday living and home improvement.
RobertAnine –
For those committed to making a lasting impact, exploring ultimate legacy guide – a platform offering practical advice on consistency, dedication, and purposeful action can make the process clearer and more achievable over time.
Joshuaedunc –
For individuals seeking motivation, visiting sites such as journey success club – a community-driven platform helps users stay inspired through shared goals and encourages consistent personal development with supportive guidance and collective progress mindset.
Russellnip –
As I reviewed financial literacy resources and investment strategy guides, I referenced explore smart investing insights in my notes – the advice is grounded and helps reinforce a calm, structured approach to financial decisions.
ScottMop –
While exploring clutter free lifestyle websites and minimal living blogs I came across in the middle of my browsing session Pure Simple Life Hub which highlighted simplicity focused living – The message felt very calming and promotes reducing unnecessary things which helps create a more peaceful and intentional lifestyle overall
RobertCesub –
https://easymexmeds.shop/# Easy Mex Meds
BrianNeago –
Shoppers today often look for platforms that encourage intentional spending habits and clearer decision-making when browsing online stores, and one example is Purposeful Shopping Hub which is often described as a place where users can explore products more thoughtfully, compare options calmly, and continue discovering items that better match their personal values, budget goals, and everyday lifestyle needs.
Stanleylar –
Many individuals seeking practical online deals explore platforms like Daily Value Explorer that focuses on affordability, and it continues to assist users by offering curated suggestions – making it easier to find essential goods that combine quality with budget-friendly pricing for everyday use.
Gregoryheedo –
Many users starting their trading journey often prefer platforms that are organized like professional academies, and I recently discovered Pro Trader Education Skills Portal which feels structured – A learning-focused trading academy that presents courses in a clear format, and honestly it looks promising at first glance for people exploring trading basics seriously.
JosephBes –
While spending some time online, I noticed something that seemed worth sharing because it had a neat and practical approach to goal tracking profit tracking hub – I found it interesting and the content feels quite straightforward and easy to follow at a glance
Hollisbig –
I recently decided to refresh my home decor and explore different stores offering stylish and affordable decorative items online home beauty decor store the two vases I purchased were packaged with exceptional care and arrived safely without any damage or issues at all
Robertshite –
Digital leaders often explore ecosystems that connect global thinkers in collaborative online environments global leadership vision space helping share ideas that influence modern innovation pathways and strategic growth – The worldwide scope is strong and I look forward to seeing its progress
WilfordTible –
Users evaluating online services often focus on how effectively the interface communicates structure and whether navigation feels logical and easy to follow UrbanScale Flow Interface – UrbanScale ensures a clean and structured layout where visual balance helps users explore content easily and enjoy a seamless browsing experience.
Thomasrurgy –
cheapest online pharmacy india: pharmacy website india – best rx pharmacy online
melbet_tvKi –
melbet autoexcludere [url=melbet63149.help]melbet63149.help[/url]
Denniszenly –
If you want a steady path toward improvement and earnings, exploring learn earn success platform – a guide that offers structured knowledge and practical online opportunities can support continuous personal and financial growth effectively.
Marvinclamb –
As I compared online clothing stores for visual accuracy and product quality, I worked in see outfit collection within my notes – the jacket I ordered looked just like the photos, which made the whole purchase feel very smooth and trustworthy.
DouglasFause –
From my perspective after a short exploration, check it out sits within a well-structured layout – the design feels fresh, and browsing here was simple and quite smooth overall.
EllisSnasp –
Many users learning trading for the first time often get discouraged by complicated material, and I found Learn Easy Trading Hub which seems helpful – The platform makes learning more enjoyable by presenting information in a simple and non-boring way, which really helps beginners stay interested and motivated.
RalphJar –
In various conversations about web performance and interface design, people sometimes highlight testing environments where tools and samples include primeimpact gateway as part of broader discussions on clarity, responsiveness, and simplified content delivery across online platforms used for general evaluation. – The overall experience is often seen as clean, direct, and visually consistent.
Walterzem –
For companies seeking dependable networks, exploring business trust network – a reliable platform enables professionals to build strong connections based on transparency and mutual benefit, encouraging sustainable growth through trusted partnerships.
LanceTet –
Creative collaboration spaces encourage users to think differently, challenge norms, and explore innovative approaches to everyday problems and professional tasks Idea Craft Collective – The collective nurtures hands on creativity, enabling members to design, test, and refine ideas through supportive peer interaction and shared learning experiences
Francislaurl –
While studying different global networking platforms and business communication forums I found in the middle of my research list Professional World Connect Hub which appeared to host frequent user interactions – I engaged with a couple of members and the community felt lively and well maintained
Oscarhok –
As I explored different online innovation resources, I found tech future hub – The platform feels aligned with progress and modern development, making it seem like a useful space for discovering emerging ideas.
RenaldoMeasp –
People who study business trends and economic patterns often look for platforms that simplify complex data into clear insights, and they may discover Trend Insight Research Hub which emphasizes analytical reporting – A structured digital platform providing market forecasts, trend evaluations, and consumer data insights designed to help users understand evolving global industries effectively.
JamesPhexy –
People exploring investment learning tools often appreciate simple platforms that explain concepts clearly, and I discovered Growth Profit Investing Simple Portal which looks practical – A straightforward investing site that provides easy financial education, helping beginners understand investment growth step by step without feeling overwhelmed by technical details.
EdwardAlemi –
Many individuals benefit from motivational platforms that highlight real journeys of growth perseverance and success across different life situations strength inspiration hub the stories shared gave me a strong motivational boost and encouraged me to stay focused on my goals immediately after reading them
Ronaldundut –
While exploring different online stores, I found something that stood out enough to mention because it had a clear and simple layout discover dream deals – the structure feels clean and intuitive, making it easy to browse through products without any unnecessary confusion
Calvinapeds –
In the process of finding better discussion spaces, I encountered this perspective-sharing site and noticed how effectively it combines different opinions, allowing for a more complete and thoughtful understanding of various topics.
DanielBib –
While browsing inspirational content hubs and positive mindset communities, I included check win daily vibes in my notes – the overall feel is motivating and pleasant, which naturally encourages me to revisit it every day.
CharlesTax –
Many designers and artists benefit from centralized inspiration platforms, including Creative Minds Outlet which supports creative exploration by offering structured resources, idea collections, and motivational insights that guide users toward successful project development – a supportive environment for artistic growth and experimentation.
RobertPioda –
For those who enjoy simple shopping decisions, exploring bright offer hub – a resource that organizes deals clearly can help users discover valuable savings and make confident choices based on straightforward and easy-to-understand information.
DennisSob –
In many communities, individuals rely on digital resources to shape better future planning habits future planning resource that encourage structured thinking and consistent self improvement practices – It serves as a helpful framework where users can organize goals, strengthen discipline, and develop actionable steps that make long term success more achievable and realistic.
Justintor –
during browsing through leadership discussion boards I saw a reference to collaborative growth among professionals in networks Leadership Synergy Network Hub I considered how group dynamics influence leadership skills – The concept seemed relevant and I think more real world case studies would improve clarity
Brycejuind –
Many users exploring business collaboration often appreciate straightforward explanations of partnership benefits, and I found Strong Business Alliance Partnership Hub which seems useful – A platform that focuses on how partnerships support growth, and it presents the information clearly so users can easily understand the importance of cooperation in business success.
Robertsaifs –
Many online buyers appreciate when they can find quality electronics at reduced prices without long waiting times for delivery discount earphone zone shop – I managed to secure a nice deal on earbuds and was impressed by how fast they arrived, making the purchase feel smooth and efficient
Robertshada –
Forex learning often becomes confusing when traders do not have a structured way to evaluate their progress, progress tracking guide which leads to stagnation – I appreciated the step by step clarity it provided for improving trading discipline and structure over long term practice gradually
WilliamHam –
Across various forums discussing societal improvement and collective responsibility, people often highlight the importance of staying informed and actively contributing to positive change initiatives community action banner – this perspective emphasizes that progress is not instantaneous but develops through consistent effort, collaboration, and shared understanding among participants
Donaldsor –
While checking various trading insight platforms, I noticed a section that blended smoothly into the page and offered clear guidance easy navigation insights making the browsing experience more intuitive – the information is presented in a very clean and straightforward way
JosiahZit –
While analyzing different platforms for home accessories, I mentioned browse quality decor within my thoughts – the offerings look high-end and the pricing matches well with the overall presentation.
Thomasrurgy –
pharmacy website india: reputable indian pharmacies – online pharmacy no prescription needed
JamesbeR –
During a search for something fun and modern, I encountered trend explorer shop – It’s a playful and engaging place filled with items that reflect popular styles and make browsing feel exciting and fresh.
DavidBug –
In various conversations about branding consistency and digital identity design, users frequently point out brandcrest structure page included in curated resources highlighting clarity, accessibility, and strong visual branding organization. – It typically feels stable, simple, and very user friendly overall.
Emiliobug –
After spending a few minutes moving through the platform, I found that open this site fits within a well-organized interface – the structure is clear, and everything looks well arranged, making the site easy to use.
Allenket –
While reviewing the interface and moving through sections, I came across go to this site which fits into a neat structure – the design is strong, and the website feels modern and very easy to use.
JamesMut –
Individuals seeking better opportunities often explore platforms that emphasize education and community development as key drivers for personal and collective success Bright Path Learning Hub offering structured programs for skill enhancement and growth – This ensures long term improvement through accessible education and supportive learning environments
Rolandfooff –
People seeking career advancement often explore platforms that focus on building strong connections and improving communication between professionals in different fields Network Trust Builder Space designed to enhance collaboration and relationship quality – This supports professional growth by encouraging consistent and reliable networking practices
Joshuaphege –
Many users interested in business alliances often appreciate platforms that offer structured educational content, and I came across Collaborative Growth Resource Portal which feels useful – A hub providing articles and insights on partnership development, and I plan to read more of its resources later tonight when I have more time.
Steveabugh –
If you want to build strong global networks, checking out global innovation hub – a platform focused on partnership can help users collaborate effectively and achieve growth-oriented results through shared expertise and coordinated teamwork.
Derrickasype –
Many productivity issues actually come from poorly structured mornings rather than lack of effort or motivation during the day itself success routine mindset hub once I fixed my morning habits I experienced a steady increase in productivity and mental clarity that felt very natural
Jameschure –
Understanding forex markets requires consistent practice with real examples rather than just reading theory, which often feels abstract without application market practice tutorial hub helping learners build confidence step by step through structured learning paths – I saw it as another valuable learning spot and the example-based approach improved my clarity significantly
RobertClemy –
While preparing a summary of useful trading platforms, I made sure to mention visit this resource in context – the domain may be different, but the tools remain just as effective and dependable for analyzing trends.
Williamhoord –
Many users looking for quick inspiration often prefer websites that provide simple and practical daily finds, and I recently explored Daily Essentials Handy Finds Hub which feels useful – A finds platform focused on everyday essentials, and I check it almost every morning since it gives short and helpful ideas that are easy to use in daily routines.
FrankieCoAwn –
While searching for online trading courses, I found a platform that looked quite helpful for new learners academy forex training guide – It gives a straightforward learning experience and seems easy to follow even for complete beginners
NormanMen –
During exploration of professional development tools and career coaching websites I came across in the middle of my study list Skill Growth Career Hub which delivered simple and practical advice – The career insights felt reliable and I often come back to this hub whenever I feel stuck or need direction in my work life
Jameshoita –
People interested in mindset transformation often explore digital platforms that promote encouragement, reflection, and shared experiences, and they sometimes discover Mind Growth Inspiration Network which supports collaborative idea exchange – A thoughtful community space designed to help users stay motivated, develop positive routines, and build a stronger foundation for lifelong learning and growth.
Robertger –
Fashion lovers in modern cities often look for clothing inspiration that blends street aesthetics with functional everyday wear suitable for diverse environments Urban Lookbook Style Zone – It showcases how fashion evolves through cultural influence and practical needs within fast paced metropolitan lifestyles around the world
WilliamApova –
Many small business owners benefit from platforms that provide consistent motivation, practical business advice, and encouragement to keep pushing forward despite obstacles, and they may find Entrepreneur Daily Motivation Hub which highlights growth mindset content – A dedicated space offering inspiring messages, strategic business insights, and helpful reminders that support entrepreneurs in building stronger foundations and achieving long-term success through consistent effort and determination.
Josephagosy –
During a casual search for networking and business strategy platforms, I came across business growth alliance – The concept feels strong and well-aligned with long-term planning, making it appear useful for structured development and collaboration.
Joshuamob –
During my exploration of cautious investing strategies and profit systems, I added check profit plan model into my notes – the setup looks strong, so I’m testing it with small amounts first to understand how it behaves over time.
EdwardCibia –
Many people who enjoy budget friendly fashion often search for small online stores that offer stylish pieces without high prices and good variety fashion sparkle hub friends kept asking where I found these cute accessories because they looked more expensive than they actually were
Jeffreyjoids –
I usually assess communities by how they handle transparency and whether they maintain open dialogue with their audience and participants integrity driven network page – it reflects a mindset centered on accountability and ethical interaction in all collaborations.
Thomasrurgy –
Easy Canada Meds: Easy Canada Meds – canadian pharmacy victoza
Josephcal –
While checking out various resources online, I came across something that seemed worth a quick mention since it had a nice flow to it simple savings link – the design is straightforward and practical, which makes it feel approachable and easy to explore for anyone
Davidboage –
Users exploring digital services often prefer websites that reduce clutter and provide a clean visual environment that supports quick understanding and easy movement between pages PureHorizon Flow Interface – PureHorizon stands out for its simple and refreshing layout, making it easy for users to browse content smoothly while maintaining a clear and distraction-free experience.
Winstonred –
As I navigated through different sections and usability flow, I noticed that visit here aligns with a structured interface – the experience is good overall, and both layout and content seem well balanced and user-friendly.
AlfredDak –
Many users who prefer positive online shopping experiences often enjoy bright and simple layouts, and I found Happy Trend Zone Product Hub which looks nice – The cheerful design helps make shopping feel more relaxed and less stressful, giving users a comfortable browsing experience where they can explore items at their own pace.
RobertCesub –
https://easyindiameds.com/# india pharmacy
Allanplunk –
Many individuals who support community-driven missions often look for platforms that provide inspiration and regular updates on ongoing efforts, and they sometimes come across Global Change Progress Network which promotes transparency – A purpose-focused initiative designed to share meaningful updates, encourage participation, and strengthen awareness around impactful projects that aim to improve society and global connections.
Eddiegab –
Online buyers who prefer structured information about discounts often visit sites such as price drop assistant for guidance – it provides organized insights into current market offers and helps users maximize savings through better awareness of ongoing promotional campaigns.
Alexhiexy –
Some traders prefer systems that clearly define entry and exit points because it reduces emotional decision making, and within forums a commonly referenced guide is breakout edge strategy noting that it helped identify two profitable movements during trending conditions in recent forex sessions globally
ThomasHox –
Freelancers and small business owners frequently need simplified ways to organize earnings and expenses in a consistent manner money strategy planner that provides step by step guidance for setting realistic financial goals and tracking progress effectively – I started using it this week and it already feels helpful for managing irregular income better
AndrewThabe –
While browsing through different online style platforms, I came across smart style collection hub – The overall presentation feels very polished and thoughtfully arranged, offering a stylish yet practical selection that makes browsing both enjoyable and visually appealing for everyday inspiration.
MelvinOpela –
During my search for beauty trend inspiration online, I found a page that stood out for its clean and elegant design approach beauty modern space – the overall look feels fresh and modern, and the content is engaging and enjoyable to explore casually
sweet-bonanza_gvpl –
sweet bonanza турнір слоти [url=http://sweet-bonanza27450.help/]http://sweet-bonanza27450.help/[/url]
Thomasrurgy –
canadian pharmacy meds review: Easy Canada Meds – canadian pharmacy review
RandyLinna –
Many online shoppers often worry about complicated payment systems and delayed updates, but my recent experience felt surprisingly simple and reassuring smooth checkout store the delivery matched product descriptions exactly and everything arrived on time without any confusion or hidden surprises making it a very stress free purchase overall
Rickymix –
Many individuals entering forex markets benefit from step based learning systems that gradually build understanding of price action and trends trader learning progression hub while applying concepts in real scenarios over time – This approach encourages steady improvement and helps create sustainable trading habits
Williamcuddy –
I was just browsing casually and noticed something that seemed worth sharing because it had a simple and approachable design everyday essentials shop – the overall feel is smooth and user-friendly, making it easy to explore items without confusion
Kevinmop –
During casual fashion browsing for hoodies and streetwear I noticed in the middle of my search results Trend Everyday Clothing Hub which offered clean and minimal designs – I bought a hoodie and shipping was much faster than expected which made the purchase experience very satisfying overall
Raymondget –
During my search for clear and practical trading education resources, I included market options clarity hub in my notes – the explanations made complex concepts easy to follow and helped me avoid several costly beginner trading mistakes.
WilliamQuify –
During a casual look at self-growth platforms, I came across motivation progress center – The idea feels balanced and inspiring, connecting motivation with personal improvement in a natural and uplifting way.
DarrellMaX –
Many people attempting lifestyle changes find that structured peer support significantly improves their ability to stay consistent over time consistency builders forum members often share that having a reliable group helps them recover quickly from setbacks and continue moving forward
Albertoamife –
I had been searching for professional online communities before discovering trusted partner vision – The website looked modern and well organized, and the updated structure made it easy for visitors to browse without confusion or overwhelming design elements online.
Robertdig –
Earlier today while browsing through different pages, I found something that seemed relevant enough to point out for others interested in simple platforms value shopping page – the layout is straightforward and allows users to follow the information without confusion or distraction
Thomasrurgy –
Online medicine home delivery: Easy India Meds – no prescription needed pharmacy
Michaelzer –
During review of trading signal providers and market analysis tools I noticed in the middle of my browsing session Reliable Trade Signal Flow which shares structured entry points – The signals so far look fairly consistent and the platform seems like another one worth observing for ongoing performance trends
DavidInobe –
After comparing several partnership platforms, I found daily partnership hub – The website felt great overall, and the content was engaging and neatly arranged, making it easy for visitors to navigate without confusion or clutter affecting usability online.
Jessicahiexy –
As I explored different e-commerce platforms focused on trendy yet budget-conscious products, I discovered affordable trend store guide – the selection feels fresh and stylish, making it my go-to option whenever I want fashion without breaking the bank.
Stephennor –
I spent some time exploring motivational platforms before discovering world change hub – The platform felt really inspiring overall, and the content appeared helpful, clear, and motivating, making it easy to stay engaged and understand everything without confusion or clutter online.
MichaelVex –
After checking multiple websites for practical home accessories and furniture recommendations, I landed on favorite household link – Everything felt organized in a natural way, and the smooth navigation made browsing much more pleasant without dealing with excessive distractions or cluttered page sections online.
Stephenfossy –
While browsing through recommendation lists I discovered a platform that feels well curated and pleasant for everyday exploration purposes Explore Daily Insights – The site offers smooth transitions between pages and the content presentation makes it easy for users to stay engaged
SamuelDor –
As I searched for motivational communities online, I noticed success development space – The platform feels inspiring and goal-focused, emphasizing steady progress and realistic pathways toward long-term achievement and personal success.
SamuelElido –
I don’t typically recommend lifestyle sites, but this one felt worth sharing because of how clean and modern everything appeared overall modern daily living – the browsing experience feels comfortable and the interface is simple and user friendly
Cliftonjes –
In my exploration of knowledge based platforms I discovered a website that inspires users to stay curious and keep learning in everyday life situations Learning Curiosity Hub – the content feels uplifting and insightful encouraging users to explore ideas, stay curious and build strong learning habits that support personal and intellectual growth over time online
JoshuaKeype –
In my browsing of retail websites I discovered a platform that offers easy shopping with structured design, smooth navigation and clear product listings for better usability Daily Shopping World Hub – the website feels efficient and organized, helping users explore products, find deals and complete purchases quickly and easily
StephenHurge –
After reviewing multiple trading education sites, I landed on smart trader hub – The platform felt helpful and well organized, and the layout was simple and easy to understand, making learning accessible without unnecessary distractions or complex design elements online.
JesusStoof –
Users who enjoy imagination driven content often prefer platforms that make idea generation simple and enjoyable, especially when they visit creative discovery hub – the website feels smooth and well organized, helping users explore limitless ideas while maintaining a clean and engaging browsing experience across all sections.
Douglaspeecy –
While exploring self improvement content related to relationships and social skills I noticed in the middle of my reading list Real Connection Advice Center which highlighted simple and applicable guidance – The approach felt honest and useful especially for people looking for grounded ways to improve their interactions
mostbet_ubEr –
mostbet logare rapida [url=http://mostbet87342.help/]mostbet logare rapida[/url]
Jamesswibe –
Many users looking for creative presents often prefer websites that make gifting simple and personal, and I recently explored Creative Gift World Unique Presents Hub which feels nice – A gift platform offering creative and standout items, and I already got something for my mom, which made the experience feel easy and heartfelt overall.
Eddienenty –
After reviewing several online learning platforms focused on trading, I discovered smart trading source – The content appeared helpful and well organized, and browsing felt easy because the pages were clean without clutter or overwhelming design elements online.
Kennethsaive –
Shoppers appreciate online platforms that make ordering simple and pleasant, where each step of the process feels intuitive and supports a smooth transition from browsing to final purchase confirmation smilingordershop – This highlights a comfortable shopping experience designed to make users feel relaxed and satisfied while completing transactions in an organized and enjoyable digital space online.
Mariapoems –
Shoppers looking for simplified clothing exploration often prefer systems that reduce clutter and highlight essential fashion options fashion browse point – focused browsing points allow users to quickly access relevant clothing categories while eliminating unnecessary distractions and improving overall efficiency during online shopping sessions
RobertCesub –
https://easycanadameds.com/# Easy Canada Meds
MartinRhisk –
During my search for global retail platforms I found a website that offers a clean interface and well organized product listings for users Market Ease Network – the platform feels dependable and user focused allowing smooth navigation across categories while providing a wide variety of products in a structured and accessible marketplace environment today
Arnoldmig –
While reviewing different collaboration networks and business discussion groups, I worked in growth connection group hub naturally – I encountered ambitious people, and the discussions were actually insightful and helped me see things from a more practical angle.
GeraldDix –
In my search for knowledge platforms I came across a website that encourages users to expand their horizon by learning and exploring new opportunities for personal growth Expand Future Horizon Hub – the platform feels structured and helpful, guiding users to develop skills, learn new concepts and discover opportunities through a clear and inspiring online experience
Thomasrurgy –
best online pharmacy india: Easy India Meds – buy drugs online
HerbertAsymn –
Shoppers looking for efficient digital marketplaces usually choose platforms that highlight clarity and structure, helping them browse products without confusion or delays Effortless Deal Hub as it improves speed and usability – The shopping experience is designed to be clean, intuitive, and focused on helping users find relevant items quickly across all categories
PatrickGen –
Stopped thinkingPeople exploring online fashion options usually prioritize platforms that are simple yet visually appealing Online fashion bazaar – this marketplace feels modern, lightweight, and designed for smooth everyday browsing – making it convenient to discover new clothing styles without unnecessary distractions quickly.
MyronFox –
While checking different forex and trading learning platforms online, I noticed a site that felt simple and well organized at first glance traders success hub – it seems like a useful resource with clear information that is easy to read and understand without unnecessary complexity
BrianPix –
While exploring online self improvement websites I discovered a platform that focuses on sharing simple and positive motivational content for daily inspiration Inspire Happy Living – the experience is helpful and easy to explore offering uplifting ideas that encourage users to stay positive and improve their mindset through gentle daily guidance online
MichealSheer –
When evaluating long-term relationships, insights from places like quick access link often stand out – Trust building continues to grow as a fundamental necessity in a constantly changing world.
BuddySoulk –
While comparing different online shopping platforms, I eventually opened exclusive value corner – The browsing experience felt smooth and modern, and products were clearly organized and visually appealing, making it easy to explore without clutter or confusion online.
JamesPough –
Individuals browsing for curated product selections often value websites that simplify navigation and enhance clarity, and modern shopping hub – offers a well-arranged collection where users can discover products easily while enjoying a smooth and visually balanced shopping experience overall.
DanielBap –
People who enjoy relaxed online shopping often look for platforms that feel easy and cheerful to browse, and while exploring they discover cheerful shopping hub space – the experience feels simple, friendly, and well structured, allowing users to browse products comfortably without stress or confusion while enjoying a smooth and pleasant interface overall.
GeorgeLig –
After comparing several shopping websites for local products and deals, I found daily market guide – The website looked clean and professionally designed, and browsing felt simple because everything was organized clearly without unnecessary clutter or distracting visual elements slowing things down online.
Jasoncoisp –
While exploring online trend analysis websites I came across a platform that delivers information in a modern structured format Trend Horizon Desk known as Trend Horizon Desk tool – users can easily browse trending insights and discover new updates with a clean interface that prioritizes simplicity and usability across all sections today right now
Isaacdef –
During my review of trading insight networks and financial analysis hubs I found in the middle of my notes Market Strategy Review Zone which offered organized breakdowns of trading trends – The analysis felt professional and consistent which helped strengthen trust in the interpretations shared this week
RandomNamehiexy –
shopandsmilealways – Great website today, products appear organized, easy and visually pleasant
Bennyciz –
In my exploration of online creativity tools I discovered a platform that motivates users to build something new and start meaningful projects easily Creative Idea Build Hub – the experience feels simple and inspiring helping users take initiative, explore ideas and turn creativity into real projects through structured online guidance today
RaymondGen –
Online users seeking personal inspiration frequently value platforms that emphasize growth and self-confidence, and life renewal hub – offers encouraging content designed to motivate individuals toward healthier habits, stronger focus, and more meaningful progress in their personal journeys.
Williamhoord –
Many users looking for practical daily recommendations often prefer websites that highlight simple and useful discoveries, and I found Daily Finds Essentials Guide Hub which seems useful – A daily essentials page offering convenient little finds, and I often browse it each morning since it provides quick inspiration for useful everyday products in a very easy way.
Philliptrope –
In many online browsing experiences centered around lifestyle inspiration and simple shopping ideas, users often discover curated platforms where convenience matters HappyLivingStoreHub – This online space is often described as a gentle lifestyle shop experience that feels easy to navigate while encouraging positive and relaxed browsing without overwhelming product choices or confusing layout elements for everyday users.
Edwardpoili –
While checking e-commerce websites I came across a platform that highlights unique products in a clean layout while providing a smooth and enjoyable shopping experience Unique Trend Discovery Hub – the platform feels simple and structured helping users explore products easily while enjoying a seamless and pleasant online shopping journey today
BrettTem –
While exploring different fashion pages online, I came across something that felt a bit different and decided to mention it here briefly fashion picks online – the design is simple yet appealing, making it easy to browse through without unnecessary complications
MichaelRounc –
As I reviewed different financial tracking platforms and market intelligence tools, I included global trading insight hub in my notes – the daily updates kept me ahead of price movements, and the chart performance is smooth and very fast-loading overall.
Donaldcouts –
People who enjoy intellectual exploration often search for platforms that encourage curiosity in a simple way, especially when they visit curious ideas discovery space – the website feels structured and friendly, helping users explore topics easily while maintaining a calm and enjoyable browsing experience throughout their journey overall.
AlbertElale –
After reviewing multiple trading education websites, I landed on smart trading system – The website felt informative and easy to use, and everything was updated and well organized, making navigation quick without confusion or clutter affecting usability online.
Jimmypremn –
While comparing different online boutiques, I eventually opened exclusive fashion hub – The platform looked modern and attractive, and products were shown clearly in a clean layout that made browsing simple without overwhelming design elements or confusion online.
Thomasrurgy –
Easy Mex Meds: Easy Mex Meds – Easy Mex Meds
Trevorbes –
While searching for practical online discount platforms I discovered a webpage that offers clearly categorized deal listings designed for fast and easy browsing Quick Deal Corner – the interface is straightforward and helps users efficiently navigate through available offers while maintaining a pleasant and uncluttered experience
Phillipbob –
While exploring idea sharing platforms I discovered a website that focuses on clear and simple concept exchange where users can easily explore and understand new ideas in a smooth and structured environment Idea Connection Hub Online – the platform feels highly intuitive and organized helping users share, browse and understand creative concepts in a clean and accessible way that encourages open thinking and collaboration
DanielAmumb –
As I explored various online style platforms, I discovered style inspiration zone – It feels welcoming and personal, offering content that makes browsing fashion-related ideas both fun and visually satisfying.
Donalddow –
Many homeowners searching for practical renovation inspiration come across Modern Space Ideas which provides helpful insights into room organization, lighting choices, and stylish furniture arrangements – The platform encourages a thoughtful approach to design, blending comfort with modern visual appeal for improved living experiences
Chasesog –
Digital consumers often value platforms that help them quickly identify trending products while maintaining a smooth and uninterrupted browsing experience Trend Vision Store designed to enhance product discovery through intelligent layout and responsive interface elements – Users benefit from faster navigation and improved clarity when exploring different product categories
SandySog –
Individuals interested in interior decoration trends often browse online platforms that help them visualize updated home aesthetics and compare different styles before making design decisions and they might find Elegant Space Finder while searching for inspiration – the platform is typically presented as offering clean navigation and structured content that makes exploring modern home ideas feel straightforward and visually appealing throughout the browsing experience.
Jamesscoog –
People researching new products online often appreciate stores with simple category structures and accessible layouts, and shopping inspiration spot – offers a streamlined browsing system that supports faster product discovery while keeping the overall experience clear, modern, and enjoyable for visitors.
WilliamQuali –
During casual browsing of marketplace examples and UI inspiration resources I came across in the middle of my notes Bright View Shopping Center which stood out for its minimal design approach – The experience felt smooth and made it easy to focus only on relevant shopping content
MauriceMoume –
During my search for shopping websites I came across a platform that provides a fast and reliable experience with a good selection of products and organized design Best Today Store Hub – the interface feels smooth and structured making it easy for users to browse and shop efficiently in a simple and well organized online environment today
Kendallmaift –
While studying online trading support systems and mentorship communities I found Adaptive Trading Mentor Point a flexible learning resource that adjusts explanations to different skill levels in trading – It felt intuitive and helpful for learners progressing at their own pace
Robertker –
People exploring self-improvement resources often value platforms that encourage confidence and continuous growth, and potential growth hub – provides motivational content designed to help users build stronger self-belief while supporting steady personal development and positive mindset changes over time overall.
Michaelutele –
During some random browsing of simple living and home lifestyle pages, I stumbled upon a site that felt very easy to understand and visually light minimal essentials hub – I appreciate the minimal layout and how effortless it is to move around the site without distractions
Zacharywhact –
People who like simple lifestyle improvement often search for platforms that focus on essential information, especially when they discover simple living essentials hub – the site feels clean and helpful, allowing users to focus on useful ideas while maintaining a structured and calm browsing experience overall across multiple topics.
Rodneyacess –
Earlier today I was checking different beauty product websites before opening modern beauty hub – The design looked beautiful overall, and browsing products felt smooth and enjoyable, making the experience simple and pleasant without unnecessary distractions or complex navigation online.
WilliamTob –
While researching places to find discounted products and useful online offers, I ended up trying best value picks – The website maintained a clean and simple appearance the entire time, making it easier to focus on browsing items without constantly navigating around distracting advertisements or unnecessarily crowded page layouts during my session.
Georgeupliz –
As I browsed various online communities focused on success and collaboration, I added success growth network hub into my notes – it really stands out as a space where people share ideas freely and everyone appears helpful and genuinely engaged in conversations.
WilliamSmept –
While exploring home design inspiration I came across a platform that showcases trending ideas for interiors with modern aesthetics and visually pleasing arrangements for all spaces Design Style Home Hub – the website feels helpful and elegant, offering users decor inspiration, stylish layouts and contemporary home transformation ideas
Bennymitle –
Users who spend time reading motivational blogs and wellness-focused content often encounter hidden recommendations for uplifting websites, and within those pathways they sometimes reach HappyLifeRipple – A gentle digital space centered on emotional wellbeing, gratitude practices, and cultivating a consistently positive mindset.
HowardAntef –
During my recent browsing of discount resources I discovered useful details at Budget Deals Portal which gathers a variety of promotional offers in a single organized page making comparison shopping much simpler for users – the presentation style appears clean and focused on usability for visitors
RandomNamehiexy –
Many fashion enthusiasts enjoy platforms that showcase modern clothing trends in an organized and visually appealing structure that makes browsing enjoyable and easy to understand at a glance modernfashionfeed – the experience focuses on delivering cleanly arranged style content that allows users to stay informed about new fashion directions while enjoying smooth and efficient navigation throughout the site
SimonWen –
Shoppers who prefer minimalistic interfaces tend to appreciate platforms that eliminate unnecessary distractions and present deals in a straightforward manner for faster decision making Savings Browse Portal so they can focus only on the most relevant offers available at any given time – The browsing experience is designed to feel clean, simple and easy to follow for all types of users
MatthewSef –
During my exploration of e-commerce platforms I discovered a website that emphasizes secure transactions and a trustworthy, professionally designed user experience Confidence Online Shop – the platform feels simple and reliable helping users browse products safely while enjoying a smooth and structured online shopping experience today
Rufusuphot –
While exploring online stores, I ended up visiting special gift picks – It’s a delightful place filled with imaginative choices that can easily turn a simple gift into something thoughtful and appreciated by anyone.
Agustinmeala –
Many users interested in economic patterns often look for platforms that explain market shifts clearly, and I found Global Market Insight Strategy Hub which seems useful – It delivers insightful financial data that helps users understand larger market movements, offering a clearer view of how global economic changes unfold.
Thomasrurgy –
india pharmacy: reputable indian pharmacies – online pharmacy no rx
TommyEmope –
I came across this while exploring a range of shopping sites and felt it might be helpful for others due to its clear and modern presentation modern trend hub – the interface feels intuitive and allows for quick browsing without unnecessary complications
Jordantuh –
People who enjoy journaling and personal reflection often look for platforms that present ideas in a peaceful and structured way, especially when they explore reflection journal space – the platform feels minimal and soothing, helping users organize thoughts and memories while enjoying a distraction free and calming browsing environment overall.
HoraceTus –
While searching for useful online resources and curated content, I eventually came across trusted value source – The website felt professionally maintained, and navigating through different sections was simple because everything was organized clearly without unnecessary clutter or intrusive advertising online.
Andrewclisk –
After reviewing multiple trading platforms, I found simple trading hub – The content felt useful and well arranged, and the structure appeared clean and professionally maintained, allowing users to browse smoothly without distractions or complexity online.
DavidVeilk –
Users who enjoy discovering elegant shopping experiences online often prefer platforms that showcase products in a structured and visually pleasing manner Designer Outlet Hub where clarity and simplicity guide navigation – this helps visitors focus on relevant items while maintaining an enjoyable and stress free browsing experience overall
JoshuaCoapy –
While exploring fashion retail sites I discovered a platform that offers stylish shopping with trendy products presented in a clean and visually appealing layout Style Trend Shop Hub – the website feels structured and elegant, guiding users to browse fashion items, explore collections and enjoy smooth shopping experience online
VirgilFeamy –
While checking educational platforms I discovered a website that promotes idea sharing and smooth interaction between learners from different backgrounds Edu Connect Hub – the platform feels well structured and easy to use allowing users to explore educational content share insights and enjoy a consistent and distraction free learning experience across all sections today
RobertSuing –
Many platforms aim to simplify how people interact with digital information by offering cleaner layouts and more intuitive discovery tools explore more world – A globally oriented exploration experience that connects users with diverse content streams allowing them to expand perspectives and discover meaningful resources across multiple knowledge domains online.
Calvincealp –
As I explored structured trading education websites and strategy training programs, I worked in master trading skill hub naturally – it was worth my time, and I gained knowledge about risk management that I previously didn’t understand at all.
DouglasAdush –
People searching for quick and simple online shopping often appreciate platforms designed for everyday use, and daily needs portal – offers a well-arranged layout that helps users browse essential items easily while maintaining a comfortable shopping experience overall.
Danielanalp –
People looking to uncover hidden discounts and lesser-known promotions often rely on specialized pages that compile various savings opportunities in one place, one such example is Savings Discovery Page – which is described as a helpful browsing resource designed to make discovering deals more straightforward and less time-consuming overall.
RandomNamehiexy –
While browsing lifestyle inspiration resources I found a platform that provides modern ideas and visually appealing content designed to improve everyday life easily Daily Lifestyle Glow – the website offers helpful inspiration that supports users in building better habits and enjoying a more creative balanced and modern approach to daily living online
JamesAbemo –
Individuals interested in modern fashion and lifestyle inspiration often appreciate websites that simplify content discovery, and fashion world gallery – supports comfortable browsing through visually organized sections that showcase stylish concepts in an appealing and easy-to-follow way overall.
RobertCesub –
https://easyindiameds.com/# indian pharmacy online
JosephSed –
People who enjoy action oriented inspiration often search for platforms that encourage travel mindset thinking, especially when they explore world exploration journey hub – the platform feels smooth and engaging, allowing users to discover ideas that motivate action while maintaining a calm and inspiring browsing experience overall across all sections.
Williamrip –
Modern shoppers appreciate digital stores that feel intuitive and reduce effort when searching for everyday goods, especially when time efficiency and clarity are priorities Smooth Purchase Portal – This experience is described as a friendly and accessible shopping environment where users can move through categories easily, find relevant items quickly, and complete transactions without unnecessary complications or confusing layouts
DonaldLip –
In the middle of comparing different online shops I came across Shiny Finds Storefront and it stood out because of its simple navigation and interesting assortment of everyday items that seemed practical for many users – the overall browsing experience felt smooth and surprisingly well organized for a lesser known platform.
CraigJed –
I came across a teamwork-focused website while browsing and thought it might be worth mentioning due to its clean and simple interface collaboration innovation space – the site looks interesting with a clean layout and easy usability that makes everything feel very straightforward
JasonGow –
While browsing various e-commerce platforms, I eventually noticed exclusive deals source – The website design felt clean and structured, and the browsing experience stayed simple because the categories were easy to understand without overwhelming advertisements or confusing layouts online.
Jesusnot –
While browsing discount deal websites I came across a platform that focuses on value outlet shopping with fast navigation and simple reliable access to products Pure Outlet Deals Hub – the experience feels smooth and structured, helping users discover affordable items, explore offers and enjoy easy shopping through a well organized online system
Wesleycok –
After comparing several gift shopping websites, I found modern gift corner – The collection appeared interesting today, and finding unique products felt effortless and convenient, making browsing simple and enjoyable without clutter or distractions affecting usability online.
MichaelPyday –
While browsing digital marketplaces focused on fashion trends I came across a platform that presents new items in a structured and attractive way Latest Style Hub – the shopping experience feels seamless and modern with clearly organized sections that help users quickly find trending products without unnecessary distractions or complexity today online
DavidLyday –
As I browsed through sites highlighting modern ideas, I noticed trend ideas center – The name draws attention and creates curiosity about the kind of trends that might be presented.
Thomasrurgy –
india pharmacy: Easy India Meds – medicine online
JeremyKah –
I had been searching for idea development platforms before discovering modern growth studio – It is an inspiring space where ideas are shared clearly and effectively, allowing users to grow without clutter or confusion online.
Grantlic –
While checking online inspiration platforms I came across a website that focuses on motivating users to keep growing forward with positivity and consistency Progress Mind Hub – the platform encourages users to stay motivated and think positively while providing simple guidance that supports continuous personal growth and improvement in everyday life online
Brianhat –
Website users typically appreciate platforms that reduce clutter and provide clear pathways for accessing information quickly and efficiently without unnecessary effort SphereUX Design Hub – NexaSphere reflects a modern web design philosophy where usability and visual structure are integrated smoothly, ensuring users enjoy a clean and responsive browsing experience throughout.
Richardref –
Users who follow fashion trends and outfit inspirations often look for platforms that balance visual appeal with structured content organization to improve browsing experience and creativity ModeStyle Journal making fashion discovery simple and enjoyable – The community atmosphere feels clean, organized, and visually engaging for style exploration.
Marioreice –
As I browsed through serious trading communities focused on real performance, I added successful market traders club into my notes – the content is honest and experience-driven, avoiding hype and focusing on what traders actually see in live markets.
DonaldFen –
Ambition without action remains only a dream but when combined with effort and persistence it becomes a powerful driver of success Ambition Booster Link Ambition without action remains only a dream but when combined with effort and persistence it becomes a powerful driver of success is shared as a reminder that execution turns ideas into reality – highlights the importance of taking consistent steps toward goals
RaymondCheft –
People exploring structured ideas for global improvement often look for platforms that combine inspiration with practicality, and they come across world improvement blueprint hub which provides organized concepts designed to help users understand how consistent positive actions can lead to meaningful change in communities and broader social systems over time.
Thomasstofs –
During a casual search for online income planning resources, I came across modern profit guide – The website felt clean and user friendly, and the information was easy to follow because everything was explained in a simple and practical way online.
RonaldSnage –
While exploring happiness lifestyle platforms I came across a website that encourages positive thinking and simple daily enjoyment ideas for users Everyday Positivity Joy Hub – the experience feels uplifting and smooth, guiding users to enjoy daily life, stay positive and develop a happier mindset through easy and meaningful content online
HowardNit –
While browsing through various trading-related resources online earlier today, I came across something that seemed worth mentioning here because it had a clear and practical presentation overall forex learning guide – the content feels useful and is explained in a straightforward manner that makes it easy to understand even for beginners without confusion
PatrickMob –
While searching for fast analytics and growth platforms, I eventually came across smart growth tracker – The website offered great content and insights, and pages loaded quickly without clutter, giving a clean and distraction free browsing experience that felt very responsive and well organized online.
JamesCrime –
In my exploration of online engagement platforms I discovered an interesting site at social discovery network – users appear active and responsive which makes interaction feel natural and the process of connecting discovering and growing within the community feels consistent and well balanced overall
mostbet_qnpi –
мостбет рабочее зеркало [url=https://mostbet64028.help/]https://mostbet64028.help/[/url]
Robertreuck –
Many online users prefer shopping environments that are visually structured and easy to navigate, especially when exploring different product types or looking for inspiration across various categories product discovery space – this platform feels refined, simple, and efficient, allowing users to browse comfortably while quickly locating items that match their preferences and interests.
sweet-bonanza_japl –
sweet bonanza código promocional para registro México [url=https://sweet-bonanza39147.help/]https://sweet-bonanza39147.help/[/url]
Rickyworry –
People searching for knowledge-based inspiration often prefer platforms that support active learning, and explore passion hub – delivers engaging content that helps users stay curious while developing stronger understanding through consistent exploration overall.
melbet_blki –
melbet kz поддержка telegram [url=https://www.melbet17638.help]https://www.melbet17638.help[/url]
Thomasbub –
While exploring online motivation tools I came across a website that focuses on providing daily inspiration to help users stay positive and engaged easily Daily Uplift Network – the content is simple and inspiring offering easy to read messages that encourage users to stay motivated and emotionally uplifted throughout their everyday experiences online
GradyWroda –
Individuals seeking daily motivation often browse inspirational spaces that help them overcome procrastination and focus on action oriented behavior Start Momentum Studio since it highlights the importance of beginning now – The message promotes energy, direction, and continuous improvement through consistent small steps
PatrickKenic –
A number of websites fail to offer a smooth experience, though dream comfort portal succeeds by providing well organized content and easy navigation, making browsing enjoyable for visitors who want useful information without unnecessary complications or distractions.
WilliamHalia –
Many digital shoppers appreciate platforms that balance simplicity with variety, allowing them to explore products without feeling overwhelmed by unnecessary design complexity shopmatrixonline – users find a dependable catalog of items presented in a clean interface that makes browsing and selecting products both easy and reassuring
Marcosjus –
Users looking to enhance motivation in their daily routines often seek structured inspiration that helps them stay productive and goal focused Motivation Rise Zone guiding them toward improved focus, stronger habits, and continuous progress in personal and professional development – It emphasizes energy, discipline, and forward moving mindset strategies.
PhilipSpori –
People who enjoy curated product browsing often search for platforms that keep favorites easy to access, especially when they discover favorites list shopping hub – the site feels structured and intuitive, allowing users to quickly select items while maintaining a pleasant and efficient browsing experience overall.
Robertamoup –
People reviewing online media platforms usually focus on how intuitive the design feels and whether the interface supports easy movement between different sections and features MediaSummit Interface Hub – The SummitMedia website offers a well-designed experience where the clean interface enhances usability, allowing users to browse comfortably and enjoy a visually pleasant structure overall.
Kennethopine –
In my browsing of modern fashion platforms I found a website that showcases fresh fashion updates and stylish ideas through an easy interface Style Trend Fashion Hub – the website feels smooth and modern, helping users explore fashion updates, view trends and navigate effortlessly through a clean and well organized online system
Darrellemere –
During my search for useful online deals and trendy accessories, I eventually noticed easy fashion stop – The pages transitioned quickly between categories, and I appreciated how organized the layout remained without overwhelming banners or distracting graphics appearing throughout the browsing process online.
Thomasbum –
While searching for uplifting websites, I discovered Positive Growth Corner which provided motivational content in a clear and engaging layout that made browsing easy – I enjoy how everything feels fresh, inspiring, and consistently positive without overwhelming the reader with unnecessary complexity
Thomasrurgy –
medication from mexico: Easy Mex Meds – mexican meds
Sheldonduent –
While checking out different online resources, I came across something that felt helpful enough to mention here briefly for others interested in growth topics growth pathway hub – the first impression seems solid, with clear information that is presented in a simple and accessible format
Stevenecobe –
While browsing curated shopping platforms, I discovered Dream Finds Online Hub which offers structured categories and a visually appealing interface that feels easy to use – interesting products are featured and browsing felt smooth and surprisingly enjoyable today throughout the experience
Michaelnow –
While checking various online social hubs I discovered a vibrant community at discovery growth network – the engagement feels organic and the platform encourages people to connect discover opportunities and grow through active participation and shared learning experiences across discussions
DavidHaR –
While browsing modern home decoration websites and art-focused stores, I included decor wall inspiration hub in my notes – I found beautiful wall art that was shipped with care and looked even richer in color and texture than expected.
Robertciz –
Many users exploring online clothing stores prefer platforms that provide structured browsing and clear category layouts for better discovery, and one example is Chic Fashion Portal which is generally described as a fashion browsing site offering stylish apparel categories and curated outfit ideas for users seeking modern looks.
DavidTob –
As users engage with digital guides and recommendation-based articles, they are often introduced to helpful discovery platforms that improve browsing efficiency, and in such moments they encounter NavigateSimpleHub – A well-structured website designed to make searching and exploring content effortless and straightforward.
Terrysef –
While checking online stores I found a website that offers a bright shopping environment where products are displayed in an attractive and organized way for easy browsing Everyday Bright Shop – the platform provides simple navigation and visually appealing product listings making it easy for users to enjoy a smooth and pleasant online shopping experience every day
Josephsmine –
In my exploration of inspiration platforms I found a website that motivates users to start today, act with purpose, and create positive momentum in life Start Motivation Hub – the platform feels uplifting and simple, helping users take initiative, build discipline and turn goals into real achievements over time
Roycesef –
People interested in curated online stores often appreciate platforms that highlight simplicity and elegance, especially when they visit modern elegance marketplace – the site feels structured and visually appealing, offering a smooth navigation experience that allows users to explore products comfortably while maintaining a clean and polished interface throughout.
Stevenslors –
While searching for trustworthy online investment resources and guides, I eventually came across daily finance hub – The website felt stable and well structured, and the information was presented clearly, allowing smooth browsing without cluttered pages or overwhelming advertisements affecting usability online.
MatthewPlalm –
Many shoppers searching for fashionable apparel online appreciate stores that combine visual simplicity with structured browsing, and modern style boutique – presents stylish collections through organized layouts that make discovering products easier and more enjoyable for users exploring current trends.
Thomasmer –
Online buyers often seek platforms that provide clear navigation and secure checkout systems, making the entire process feel predictable, safe, and easy to understand from start to finish safeshopperlane – This reflects a well structured shopping experience where users can explore products confidently while benefiting from a professional and transparent online environment designed for ease and trust
BrockMum –
People using online resources often look for platforms that make information discovery easier through structured layouts and intuitive navigation systems BrandVision knowledge page – the knowledge page structure in BrandVision organizes content in a way that enhances readability and supports faster user comprehension overall.
DavidRew –
After spending time reviewing online educational resources, I eventually visited learning ideas hub and discovered several interesting topics that made the browsing experience enjoyable, encouraging me to revisit later when searching for creative inspiration and thoughtful content.
BillyTub –
Students seeking flexible learning environments often benefit from curated digital platforms that streamline information delivery and simplify concept building LearnHub Today offering structured guidance that supports steady progress – This type of educational layout encourages learners to stay engaged while gradually improving their understanding through consistent exposure.
EddiePhymn –
While browsing motivational websites I discovered a platform that emphasizes inspiring users to start their journey toward meaningful goals and personal growth New Journey Inspiration – the experience encourages users to take action today through uplifting content that supports positive change and helps build direction in life through simple and engaging guidance online
RamiroTuh –
Modern e-commerce users value speed and simplicity when exploring new collections, especially when they want quick results without complicated filters slowing them down quick cart hub – the experience feels straightforward, minimal, and efficient, giving users a sense of fast interaction while browsing various product listings online today.
Jamesvax –
I came across a teamwork-focused website while browsing and thought it might be worth mentioning due to its clean and simple interface collaboration innovation space – the site looks interesting with a clean layout and easy usability that makes everything feel very straightforward
Jasonzep –
While searching for modern lifestyle inspiration sites, I found Unique Style Living Portal which features a clean design and neatly arranged content that improves usability – overall the website feels pleasant and browsing categories is smooth, visually appealing, and simple to explore without confusion
Douglashap –
Online buyers who want to reduce unnecessary expenses often depend on tools that track price fluctuations and highlight beneficial purchasing moments across e commerce sites Cost Cutter Channel – Focuses on helping users identify cost saving opportunities and provides useful insights that improve overall budgeting and shopping efficiency in digital environments
Haroldhoigh –
After checking several online shopping deals sites, I discovered daily savings hub – The platform felt smooth and modern, and the updated content made browsing simple because categories were clearly structured without clutter or unnecessary visual noise online.
StephenBailm –
During my search for flexible e-commerce platforms with smooth interfaces, I worked in global shop selection hub naturally – the product variety is large and the mobile navigation performs well, making the browsing experience efficient and enjoyable overall.
Thomasrurgy –
top 10 pharmacies in india: Easy India Meds – legal online pharmacy
MatthewAreks –
While exploring self improvement platforms I found a website that helps users grow confidence and adopt a positive mindset through structured and simple content Growth Support Confidence Hub – the website feels motivating and clear, guiding users to strengthen mindset, build habits and follow easy development ideas through a clean online system
DavidLyday –
Nice one. Check this out: this page
Stacywed –
Many platforms offering reflective content include embedded tools designed to support understanding, such as clarity journey map integrated within structured paragraphs – This improves readability and encourages users to think more carefully about their personal development path.
Jerryadhen –
While checking e-commerce websites I came across a platform that delivers a happy and cheerful shopping vibe with simple navigation and user friendly design for all visitors Smile Everyday Shop – the platform feels welcoming and easy to explore with a joyful atmosphere that makes online shopping smooth, pleasant and enjoyable for users looking for simple shopping experiences today
CarltonDeema –
People who like reading motivational content often search for platforms that make inspiration easy to understand, especially when they visit daily positivity guide hub – the website feels clear and engaging, helping users stay inspired while offering structured content that supports emotional balance and personal growth in daily life situations.
HarryFique –
While searching for new fashion collections and seasonal outfits, I eventually came across modern wardrobe hub – The website displayed items in a clean and attractive way, and navigating through categories felt effortless because everything loaded quickly without overwhelming distractions or cluttered visuals online.
MichaelDwEri –
Online users interested in self-development often appreciate platforms that combine motivation with practical encouragement, and fresh start station – offers supportive content that helps individuals build confidence and embrace new opportunities with a more positive and determined mindset overall.
Jamessit –
Users comparing digital platforms often prioritize usability, speed, and how effectively the interface helps them locate content with minimal effort ConnectFlow Interface Portal – The UltraConnect platform combines fast performance with a clean design, making browsing simple, intuitive, and visually appealing for all users.
Michaelbeaxy –
Users who prefer organized product listings and clear categories often search for platforms that reduce confusion and improve decision making during online purchases BuySmart Center – A thoughtfully designed shopping environment that emphasizes clarity, structured browsing, and a seamless experience for comparing items across multiple categories without friction.
PhillipGaM –
While exploring modern ecommerce discovery platforms I found a website that focuses on showcasing trending products in a clean and visually appealing layout Trend Discovery Hub – the platform offers a fast and user friendly experience making it easy for users to browse the latest trendy finds while enjoying a smooth and modern shopping interface today
Richardblobe –
During my browsing of community interaction sites, I discovered Together Community Connect Hub which provides a clean design and structured browsing flow that feels intuitive – the community vibe feels strong and engaging content keeps me coming back because it feels active and welcoming
NelsonPes –
Many websites struggle with confusing layouts, although easy structure guide keeps everything simple and organized, helping visitors browse comfortably while finding information quickly without unnecessary effort or distraction during their time on the site.
BrandonWrold –
Shoppers who value purpose driven browsing experiences tend to look for platforms that simplify product exploration and decision making, and an example frequently noted is Intentional Purchase Hub – offering a focused environment where users can explore items with clear descriptions and supportive guidance that helps improve confidence in selecting suitable products.
SamuelRance –
After checking several motivational websites, I discovered modern start journey – The platform felt inspiring overall, and the layout remained clean and enjoyable, making browsing simple across devices without clutter or confusion online.
Jessetar –
During casual exploration of shopping platforms, I discovered Today Shop Trend Hub which provides a visually clean structure and smooth navigation that feels intuitive – I found interesting products and the layout remains modern, simple, and easy to use across all sections
Keithgat –
During my browsing of motivation platforms I came across a website that promotes inspiring change and encourages users toward personal development through clear guidance Inspire Growth Change Hub – the platform feels smooth and encouraging, helping users improve habits, strengthen mindset and follow positive transformation steps through a clean and accessible online experience
Eugenelaw –
Fashion seekers who appreciate refined clothing styles often explore online marketplaces that highlight elegance and modern design thinking Elegant Fashion Storefront offering curated collections that suit both casual wear and formal fashion preferences in one place – The storefront experience focuses on simplicity, ensuring users find stylish apparel without unnecessary complexity or clutter.
JoshuaFruff –
While exploring various shopping websites for clothing and accessories, I eventually came across trendy fashion source – The design felt clean and professional, and everything was arranged in a way that allowed smooth browsing with fast loading pages and no distracting popups interfering with the experience online.
RandomNamehiexy –
People exploring self development often look for tools that help them gain focus and direction, especially when they discover personal growth navigator – the platform feels clean and supportive, making it easier for users to reflect on their goals while receiving structured guidance that encourages clarity and thoughtful life planning overall.
WilliamVeine –
While browsing online idea and opportunity platforms I found a website that offers structured insights designed to help users discover valuable possibilities Opportunity Guide Network – the platform presents clear and useful ideas making it easy for users to explore options and understand potential paths in a simple and effective way for everyday growth today online
Jasonhon –
While exploring performance-based trading platforms and analytical systems, I worked in market tested strategy hub naturally – the strategies performed well, and the backtesting results closely matched real trading conditions, giving me more confidence in their reliability.
Ronaldger –
Many online consumers enjoy platforms that highlight the latest fashion trends through well-organized and visually dynamic product displays daily NovaStyle Market allowing smoother browsing and enhanced product visibility – This reflects how digital retail continues to evolve toward more engaging and efficient shopping experiences.
Marcoeruct –
People browsing for affordable and useful products often rely on organized collections that present information clearly helping them avoid confusion and make faster choices while exploring options Smart Selection Hub collection provides neatly arranged categories that support quick evaluation – Emphasis is placed on simplicity and effective product discovery
Thomasrurgy –
Easy Mex Meds: mexicanrxpharm – Easy Mex Meds
MatthewVex –
People who enjoy lifestyle guidance often prefer platforms that simplify complex ideas into easy steps, especially when visiting balanced life inspiration portal – the site feels smooth and structured, offering helpful insights that promote calmness, consistency, and a more thoughtful approach to daily routines and personal development practices.
JosephThina –
While browsing self development tools I came across a platform that focuses on creativity and structured idea generation for users Think Create Flow – the experience helps users think more clearly, develop useful ideas and grow effectively through engaging content and a simple interface designed for everyday learning and improvement today
HarryBrili –
While browsing idea sharing platforms, I found Possibility Ideas Explorer Hub which features a clean design and structured content layout that improves usability – there are lots of inspiring ideas here and it consistently opens new possibilities daily in a very natural flow of information
DavidLyday –
Good info here. See this link: this page
Ronaldemavy –
Many online visitors prefer websites that feel clean and modern while still offering engaging content and easy-to-navigate structures that improve usability UrbanNexus UI Gateway – UrbanNexus combines interesting content with a simple yet visually appealing design, creating a browsing experience that feels smooth, organized, and enjoyable for users.
Jessestatt –
I spent part of the afternoon exploring creative websites before finding smart ideas space – The ideas presented are inspiring and consistently useful, making browsing smooth and engaging for users looking for creativity and new inspiration online.
CharlesBum –
Anyone trying to shop smarter online should consider browsing resources that aggregate deals and suggestions, especially platforms like deal discovery platform this one, which focuses on highlighting savings opportunities, comparing everyday products, and helping users avoid unnecessary spending on routine purchases easily efficiently.
RandyJak –
Compared with overly cluttered websites that overwhelm visitors quickly, informative content hub keeps the browsing experience comfortable through practical information and accessible presentation, helping users remain engaged while exploring multiple ideas and creative resources online.
RonaldFew –
While browsing different seasonal fashion stores, I eventually noticed modern outfit collection – The collection looked stylish, and the website felt modern and visually appealing, making browsing easy and enjoyable for visitors without confusion or overwhelming design elements online.
Barneyhap –
While checking online gifting platforms I came across a website that showcases nice gift ideas and makes browsing simple, convenient and enjoyable for users looking for inspiration Everyday Gift Picks Hub – the platform feels smooth and user friendly, helping users discover creative and meaningful gift ideas in an organized and easy online environment today
Edwarddaw –
People searching for structured deal listings often enjoy platforms that present savings in a clear and simple layout making browsing easier and more efficient for everyday use Discount Journey Guide – Offers are arranged logically so users can follow a smooth browsing path while identifying the most relevant and beneficial deals quickly.
Dennishiz –
While looking through comparison platforms online, I came across Smart Choice Options Hub which had organized categories and easy navigation flow, making browsing simple and efficient – the content felt clear and genuinely useful for understanding different available choices quickly
Armandousemo –
I had been searching for beginner friendly trading information before discovering daily forex guide – The website looked clean and informative, and the resources were presented in a practical way that made trading concepts easier to understand without overwhelming technical language online.
RandomNamehiexy –
People who appreciate both education and imagination often search for platforms that support curiosity, especially when they visit creative knowledge corner – the website feels organized and inspiring, helping users explore learning materials while encouraging thoughtful discovery and imaginative thinking in a calm and user friendly environment overall.
RaymondPiz –
While checking motivational websites I came across a platform that focuses on inspiring action, creativity and strong personal development through simple ideas Great Start Life Hub – the content feels uplifting and supportive helping users take action, build creativity and focus on consistent personal growth through everyday motivation online today
EddieGax –
People who compare products or services online often waste time on irrelevant details, so using structured resources such as option filtering tool can help narrow down results effectively, offering clearer insights that make decision-making faster, more practical, and significantly less stressful overall.
JosephBrido –
While exploring innovation focused websites I discovered a platform that feels thoughtfully designed and easy to navigate for users interested in creativity Innovation Spark Center – ideas are displayed in a structured format making browsing enjoyable and allowing users to naturally explore useful concepts that encourage inspiration and productive thinking throughout their visit today
Davidstymn –
During my exploration of self development content, I found Dream Path Achieve Hub which offers a smooth interface and well arranged information that feels intuitive – it is a motivational platform with useful tips for personal growth journeys online and supports meaningful life changes
mostbet_avka –
mostbet apk [url=www.mostbet76205.help]www.mostbet76205.help[/url]
mostbet_wmMn –
mostbet yerli kart [url=www.mostbet47152.help]www.mostbet47152.help[/url]
mostbet_xvSi –
mostbet androidda royxatdan otish [url=www.mostbet47190.help]www.mostbet47190.help[/url]
Cynthiahiexy –
During my exploration of online trading mentors and structured coaching programs, I added confident trading mentor hub into my notes – the explanations are patient and easy to follow, helping me feel ready to trade alone starting with small risk first.
Arrondiera –
Users interested in motivation and structured self development resources can visit growth direction guide which offers reflective articles and practical strategies – helping individuals build consistency, improve habits, and maintain focus on long term personal growth through small but meaningful daily actions that compound over time effectively
ArthurLat –
Users interacting with modern websites often prioritize fast response, clean visuals, and logical structure that improves overall navigation flow CoreSystem Power Link – PowerCore offers a structured interface that feels strong and reliable, allowing users to browse comfortably with minimal effort and clear direction.
KevinPet –
In my browsing of goal setting websites I found a platform that helps users discover ideas and dreams through an easy and helpful structure Dream Goal Explorer Hub – the platform feels simple and motivating, helping users identify goals, explore inspiration and find meaningful direction through a clean and accessible online discovery system
DonaldPoemi –
While exploring online trend sources, I eventually found smart trend hub – The platform felt clean and structured, and the latest trends were easy to access quickly because everything was organized clearly without clutter or confusing visual elements online.
Thomasrurgy –
Easy Canada Meds: canadian pharmacy in canada – Easy Canada Meds
Williamhak –
I spent some time browsing deal websites before discovering life savings deals – The deals listed here looked awesome, and browsing felt easy, quick, and convenient today, making it simple to compare offers without confusion or unnecessary clutter online.
JavierPuh –
While browsing through digital platforms designed for content discovery and user engagement, people often encounter streamlined websites that prioritize ease of use and clarity SmoothDiscoverNet which – creates a seamless experience focused on helping users navigate new information quickly comfortably and without unnecessary complexity at all times.
Edwardduh –
While reviewing websites related to positive lifestyle changes and useful guidance, I encountered direction focused website and immediately noticed the quality of the presentation, since the information feels polished and engaging enough to encourage visitors to continue browsing through different sections comfortably.
RogerCal –
During a late night browsing session for fashion websites, I eventually visited smart style hub – The design looked modern and appealing, and mobile browsing felt smooth and enjoyable because the layout stayed simple, responsive, and free from unnecessary clutter or interruptions online.
DavidLyday –
I found this useful. Take a look at this if you need more: this site
Thomasoxype –
Users who enjoy inspirational platforms often look for content that pushes them toward action, especially when they come across make change today space – the site feels structured and energizing, allowing users to move from ideas to action while staying focused on creating meaningful and positive outcomes in real life.
GregoryFus –
Online browsing becomes more efficient when platforms present options in a structured and easy to follow format Direct Selection Point helping users focus on key differences and make informed choices without feeling overwhelmed by too many details during regular shopping decisions online today
Dallashadia –
In my browsing of informational websites I found a platform that delivers useful daily updates with content that feels fresh, relevant and easy to follow Update Daily Flow Hub – the website feels well structured and easy to use helping users stay updated with simple and consistent information in a smooth daily experience online
Larrydop –
During casual exploration of online stores, I discovered Shop And Shine Network which had a smooth interface and responsive structure that made browsing effortless – the site navigation works very well and pages load quickly without any glitches or delays affecting usability
JorgeImido –
People interested in self improvement often explore structured ideas that help them rethink habits and adopt more effective approaches to everyday challenges and goals better habits explorer – A practical development focused approach that motivates users to refine daily routines and adopt smarter behaviors leading to more consistent and meaningful personal progress over time.
Williambeark –
In my recent online browsing of discount platforms I found a website that focuses on smart and practical product selection for users Smart Deal Hub – the platform is easy to navigate and helps users find useful items quickly while providing a reliable and efficient shopping experience across different product categories today
EdwardEnurn –
During casual exploration of interior inspiration platforms, I found Modern Room Design Hub which features a clean and modern interface that enhances clarity – modern designs are showcased well offering perfect inspiration for home upgrades today in a simple and creative flow
BrooksJex –
Users interested in improving their daily mindset often seek inspirational content that challenges rigid thinking and promotes flexibility, frequently engaging with platforms such as Mind Refresh Studio which provide reflective exercises and motivational guidance for personal growth – The focus is on encouraging awareness and new perspectives in life situations.
Michaelgalry –
Online users who prefer consistent and well structured shopping platforms often look for stores that simplify every step, and a frequently mentioned example is Reliable Favorites Product Hub – offering a seamless browsing experience where customers can explore items easily, enjoy clear organization, and complete their shopping journey with comfort and efficiency throughout.
Glenndox –
While exploring personal development content I discovered a platform that promotes better decision making and encourages users to improve their life direction Change Forward Hub – the website feels supportive and motivating helping users build better habits, make positive decisions and move toward long term life improvement and personal success online
Gerardoguert –
While reading through online self improvement resources and inspirational blogs, users often come across platforms designed to support mindset transformation, such as LifeUpgradePortal – The focus is on encouraging growth oriented thinking, embracing change, and building healthier mental habits over time through consistent reflection.
MatthewNup –
I had been searching for easy exploration platforms before discovering exclusive love hub – The website felt pleasant and clean, and categories were well arranged, allowing smooth browsing without unnecessary distractions or complicated navigation issues online.
DavidLot –
In conversations about responsive web systems and performance focused design, users sometimes refer to ascend mark speed portal included in curated lists of efficient browsing platforms and clean interface structures. – It is commonly perceived as quick, reliable, and well optimized overall.
PedroCam –
Creative thinkers often find value in platforms like Creative Spark Network which encourages experimentation and idea sharing – it promotes imaginative exploration, supports innovative thinking, and inspires users to develop original concepts while engaging with content that broadens perspectives and enhances overall cognitive flexibility in meaningful ways.
LanceFlich –
I spent some time exploring different fashion trend websites before discoveringmodern trend hub – The browsing experience felt smooth and enjoyable overall, and the latest trends were updated regularly while being presented in a visually attractive and easy to navigate way online.
Caseyhyday –
People who enjoy idea exploration often search for platforms that simplify creative thinking, especially when they discover idea development portal – the website feels smooth and intuitive, helping users build concepts step by step while maintaining an inspiring and clutter free browsing experience across all sections.
GeraldPeste –
Several online communities often discuss fast websites, and among those suggestions I noticed speed action portal which provides easy navigation and quick page loading across all devices, making it a reliable and convenient browsing experience for users.
Thomasrurgy –
mexico pet pharmacy: Easy Mex Meds – Easy Mex Meds
Michaelbew –
During my search for online creative communities I came across a website that makes sharing ideas feel natural, easy and highly engaging for users Creative Connect World – the platform feels welcoming and smooth allowing users to engage with others and share creativity in a positive and collaborative environment designed for inspiration online
ChesterFiept –
While searching online for motivation tools, I discovered Start New Beginning Hub which provides well arranged content and a user friendly interface that enhances browsing – I enjoyed exploring this platform today and everything felt organized, clear, and easy to move through
Danielcet –
In today’s web exploration I came across a platform that felt emotionally rich and visually easy to navigate Calm Reflection Space – the content is presented in a soothing format that encourages users to slow down and appreciate meaningful digital moments without feeling overwhelmed by complexity
Keithflick –
During my browsing of lifestyle essentials stores, I found Simple Living Essentials Online Hub which presents content in a clean and modern format that is easy to follow – simple living essentials make daily routines easier and better always by helping users focus on what truly matters
DavidLyday –
Very helpful. Check this out: this page
DavidAbory –
Online learners who value structured study experiences frequently appreciate educational tools that simplify navigation, and learning support system – creates a user-friendly environment where lessons feel easier to follow, helping individuals gain confidence and retain information more effectively during long-term educational development.
GerardoRet –
Shoppers looking for fresh seasonal outfits can visit updated style collections online seasonal fashion picks hub offering trendy apparel and accessories suited for changing weather and modern lifestyle preferences – this marketplace encourages users to refresh their wardrobe with practical and stylish clothing solutions
LeonardTes –
Cost focused consumers regularly browse marketplaces that provide structured access to affordable products and deals Everyday Value Store while reviewing different shopping options – The platform is designed to make browsing feel natural, fast, and centered around practical everyday savings for all types of users
Andrewmex –
While browsing guidance resources I came across a platform that helps users find direction and clarity through simple and structured insights Simple Path Guidance Hub – the platform feels engaging and helpful, allowing users to explore life direction, understand decisions and gain clarity through a smooth and accessible online experience
Edwardtep –
After reviewing multiple recommendation sites, I landed on simple choice hub – The platform felt helpful and reliable, and the content was professionally arranged, making it easy for readers to navigate without distractions or unnecessary complexity online.
Robertson –
Individuals looking for enjoyable online discovery experiences frequently prefer websites that make navigation effortless, and hidden wonders portal – provides a smooth and engaging environment where users can explore interesting ideas comfortably while enjoying well-structured content overall.
Henryalott –
Users exploring modern digital platforms often notice how futuristic design choices and structured layouts influence overall browsing comfort and engagement across different sections NovaOrbit Portal Access – NovaOrbit presents a futuristic visual style combined with well-organized content arrangement, making exploration smooth, engaging, and easy for users who prefer intuitive navigation experiences.
Josephjep –
After comparing several online resource pages for useful insights, I landed on daily report link – The content looked consistently refreshed and the straightforward layout helped make navigation easier without distracting advertisements or confusing structures online.
ManuelCow –
Users who appreciate modern ecommerce design often look for platforms that organize trendy products clearly, especially when they come across fashion trend find hub – the website feels structured and visually appealing, allowing users to browse items comfortably while maintaining a simple and efficient shopping flow throughout their experience.
Jamaalsen –
Many people seeking inspiration prefer content that encourages exploration of ideas and experiences while helping them stay grounded, mindful, and motivated in their personal growth journey exploremindset – It supports continuous learning, curiosity, and a balanced perspective on daily life experiences
ArturoDoR –
Several online communities often discuss trend platforms, and among those suggestions I noticed daily trend guide which provides a nice collection of updates that look modern and visually appealing, making browsing enjoyable and easy for users.
MichaelLer –
During my search for online retail websites I came across a platform that offers a simple and clean shopping environment with reliable and well presented products Simply Best Market Hub – the platform feels easy to navigate and structured in a way that helps users browse quickly and enjoy a smooth online shopping experience today online
Josephcic –
Technology enthusiasts often explore online resources that showcase predictions and advancements shaping tomorrow’s digital and scientific landscape forward thinking hub – A mindset oriented discovery space – encouraging exploration of future concepts while presenting structured insights that help users understand potential innovations in an accessible format.
RobertFaurf –
While exploring online fashion catalogs I found a platform that presents new seasonal collections in a visually structured and attractive way Season Trend Showcase – the browsing experience feels smooth and modern making it easy for users to view stylish clothing items while enjoying a clean and appealing interface across all sections today
Stevenlot –
While searching online for clothing ideas, I came across Classy Fashion Trend Hub which provides a modern and visually appealing interface that is easy to browse – elegant styles are highlighted and the fashion selections available feel classy and thoughtfully selected for users
RodolfoMak –
Across studies of modern discovery interfaces, analysts frequently mention the role of embedded links in enhancing comprehension, particularly when exploration desk is included within structured paragraphs – The platform is commonly appreciated for its smooth interaction flow and visually consistent design elements.
Thomasrurgy –
Easy Mex Meds: best mexican online pharmacy – pharmacy in mexico city
Davidmuh –
While searching for accessible fashion websites, I discovered Style Everyday Corner Hub and the interface felt structured and easy to move through, making browsing straightforward – overall it delivers a clean and user friendly experience suitable for daily exploration
JosephSeism –
During my exploration of e-commerce stores I discovered a website that showcases elegant finds and provides a smooth and well organized experience for users Classy Finds Store Hub – the platform feels simple and refined making it easy for users to browse stylish items while enjoying a structured and pleasant online shopping journey today
NormanBig –
Users searching for engaging and informative online content often prefer platforms that guide them toward new discoveries and keep their browsing experience dynamic ExploreMind Network Insight Discovery Portal – it helps users stay motivated to learn and discover new ideas while offering consistent access to interesting online resources
RandomNamehiexy –
Users exploring modern lifestyle concepts frequently prefer resources that combine simplicity with attractive design, and home trend navigator – creates a smoother browsing flow that helps visitors explore practical ideas comfortably while maintaining a visually modern and easy-to-follow experience throughout.
Jackiedib –
I spent some time exploring different online stores before discovering unique trend shop – The shopping experience felt very nice today, and products were displayed clearly and attractively throughout the website, making browsing smooth and enjoyable overall without confusion or clutter online.
Carlosmut –
I was casually browsing through online shopping recommendations when I came across budget friendly corner – The website maintained a simple presentation throughout the visit, and I liked how naturally the sections connected together without endless distractions, overloaded menus, or excessive advertising slowing the overall experience down online.
DavidLyday –
Good info. Check out the following for more details: this website
WilliamCam –
Many digital audiences prefer platforms that provide consistent design and logical structure that improves readability and reduces confusion during navigation TrueLaunch Experience Link – TrueLaunch delivers a clean and reliable interface where information is clearly organized, allowing users to explore content without difficulty or frustration.
Damienram –
Users who enjoy straightforward fashion advice often prefer platforms that simplify outfit creation, especially when they visit simple everyday style hub – the website feels clean and user friendly, offering easy inspiration that helps users create balanced looks quickly while maintaining a visually appealing and practical browsing experience overall.
LouisAnnot –
After reviewing multiple growth platforms, I found smart growth space – The platform is helpful for development, and opportunities appear clear and accessible today, making exploration smooth and user-friendly without clutter or confusion online.
Jerrysiz –
While exploring digital creativity websites I discovered a platform that focuses on helping users develop ideas and grow through simple and practical inspiration Create Idea Hub – the content encourages users to think creatively and grow steadily through structured guidance designed for continuous personal development and meaningful progress in everyday life today online
ElliotNaf –
While browsing informational directories and general content websites, I came across Value Corner Reference Hub featured among similar platforms – The structure feels clean and logical, providing users with an easy and pleasant browsing experience while exploring different sections today.
Josephhiexy –
While checking online retail platforms I found a website that delivers a clean and highly efficient shopping experience for everyday users Top Shop Explorer – the platform feels organized and easy to use allowing users to browse products quickly while maintaining a trustworthy and smooth shopping environment throughout their session today online
Gregorybobia –
During casual browsing of essentials marketplaces, I discovered Your Essentials Finder Hub which provides a structured interface and smooth navigation experience – useful everyday items found quickly with very convenient shopping experience overall for efficient purchasing
pinup_qbSt –
pin-up Payme depozit [url=http://pinup84537.help]http://pinup84537.help[/url]
SamuelEmoda –
A friend recently recommended checking several uplifting websites, and while exploring them I found cheerful content space which stood out because the friendly tone and welcoming design make browsing enjoyable for visitors who want a smooth and pleasant online experience overall.
Tylerambum –
Modern urban shoppers who prefer clean design aesthetics often visit curated platforms for clothing ideas Modern Urban Dressing Hub helping them find outfit inspiration, compare seasonal collections, and improve wardrobe choices efficiently – Hub experience delivers simple and effective fashion browsing tools
CurtisChalk –
While exploring discovery based websites I found a platform that encourages users to imagine dream places and explore ideal destinations through ideas Dream Location Vision Hub – the website feels smooth and inspiring, helping users visualize places, discover inspiration and explore travel ideas through a simple and organized online environment
JimmySak –
Shoppers looking for innovative and uncommon items often browse creative goods explorer which brings together curated product selections helping users find inspiration beyond standard retail – offering access to unique items that improve everyday experiences through originality and thoughtful design choices.
RobertSus –
Users searching for meaningful learning experiences often appreciate platforms that combine creativity and connection, and idea collaboration guide – supports interactive engagement where individuals can share thoughts, develop concepts, and grow together through structured and inspiring creative exchanges overall.
DonaldOmino –
During my exploration of personal awareness websites, I found Every Moment Focus Guide featured among curated resources – The browsing experience felt enjoyable, everything appeared clean and surprisingly easy navigating overall with structured layout and easy to understand navigation flow today.
Richardmef –
Modern online shoppers often look for platforms that combine speed with simplicity, allowing them to access curated deals without struggling through complicated filters or overwhelming product pages Savings Navigator Site – The browsing experience remains smooth and efficient, helping users discover relevant deals quickly while maintaining clarity and avoiding unnecessary steps during the shopping process.
AnthonyIteli –
While searching for idea driven platforms, I discovered Vision Horizon Hub which displayed engaging information in a simple layout that made browsing pleasant – I came across useful inspiration today and I am planning to revisit again soon for more content exploration
Williamken –
While browsing different financial learning websites, I eventually noticedsimple trading corner – The platform was easy to navigate and the information was presented clearly, making it simple for beginners to grasp trading basics without unnecessary complexity or confusing explanations online.
MelvinUtign –
globaltrendmarket – Great marketplace overall, browsing different sections feels smooth and straightforward for everyone.
Thomasrurgy –
canadian pharmacy antibiotics: Easy Canada Meds – Easy Canada Meds
Waynesaike –
People who like value centered online stores often look for platforms that prioritize ease and speed, especially when they discover efficient value marketplace – the platform feels structured and smooth, helping users browse products easily while maintaining a clean and fast shopping experience that supports quick decision making overall.
Bobbylew –
Many users look for content that gently improves mood and adds positivity into their daily scrolling habits across different platforms happy moments portal – The experience feels light and refreshing, encouraging a mindset focused on appreciation, calm satisfaction, and small everyday wins that make routine digital browsing more pleasant and enjoyable.
DanielKef –
Many digital visitors expect platforms to offer intuitive navigation and a well-organized layout that supports quick access to essential tools and information TekInnovate Stream – The InnovaTek design philosophy focuses on simplicity and innovation, delivering a user experience that feels efficient, modern, and highly functional across all key sections.
Felixrounk –
While checking personal interest platforms I discovered a website that is designed to help users explore new hobbies and meaningful activities in a structured way Love Your Interest Hub – the experience feels helpful and easy allowing users to discover passions smoothly while enjoying a simple and engaging browsing journey focused on self discovery today online
MichaelFiefs –
After comparing several inspiration websites, I found daily moment space – The content feels inspiring overall, and each moment is meaningful and well presented, allowing users to explore smoothly without distractions or complex navigation elements online.
Derektwife –
Users who enjoy personal transformation content often search for platforms that combine motivation with practical self expression and confidence building guidance Shine Within Network – The experience promotes authenticity, encouraging individuals to explore new perspectives and communicate their personality through meaningful creative outlets
KennethRon –
In my exploration of digital creativity spaces I found a platform that delivers clean design and meaningful content for users Vision Builder Portal making navigation smooth and enjoyable – it feels structured yet inspiring allowing individuals to focus on building ideas and exploring new possibilities without unnecessary distractions or confusion during browsing sessions today
Williamitand –
During casual exploration of personal development sites, I found Start Awesome Success Hub which offers a clean interface and organized layout that enhances readability – this motivation hub encourages action and fresh creative thinking always for achieving personal goals
MatthewScora –
During my browsing of e-commerce trend platforms and digital product discovery hubs, I found NextGen Trend Market listed among useful resources – Nice collection here, pages loaded smoothly and content felt engaging, giving a clean and intuitive experience while exploring different sections today.
KennethRem –
While exploring digital discovery tools I came across a platform that helps users find something new through ideas and opportunities daily Fresh Opportunity Explorer Hub – the platform feels clear and engaging, allowing users to explore concepts, discover opportunities and stay curious through a well organized and simple online experience
DavidLyday –
Exactly. For further info: visit here
RalphKaw –
Across various educational platforms and creative communities, users frequently search for structured inspiration that can guide their thinking processes while engaging with tools like Innovation Spark Center – providing an environment where experimentation is encouraged, ideas are refined through repetition, and learners gradually build confidence in expressing original concepts across multiple digital mediums
DouglasNUH –
I recently spent time comparing online home stores and eventually found living comfort hub where the product layout is excellent and intuitive, creating a comfortable browsing experience for visitors exploring different home and lifestyle products.
DavidFew –
Users searching for organized home and lifestyle platforms often benefit from stores with intuitive navigation systems, and home style navigator – supports smoother browsing by arranging collections in a logical way that makes shopping feel easier and more efficient for everyday users online.
RobertoFah –
After looking through multiple online recommendation platforms, I eventually opened top browsing destination – The overall experience stayed clean and responsive, allowing content to be explored comfortably without overwhelming distractions online.
Robertjap –
During my search for shopping outlets, I came across modern smart shop – The website presentation felt clean and organized, and everything appeared updated and simple, making product browsing easy without confusion or clutter online.
MauriceUnodo –
People who enjoy contemporary lifestyle inspiration often search for platforms that showcase fresh and stylish ideas, and while exploring they discover modern lifestyle inspiration hub – the content feels clean, modern, and easy to navigate, making it simple for users to explore trendy concepts and stay updated with stylish living ideas without feeling overwhelmed or distracted.
Robertmet –
While searching for creativity focused platforms, I discovered Journey Creative Inspiration Hub which features a structured and modern interface that supports easy exploration – the website has a clean design and the content remains interesting and naturally presented in a clear way
Jerryneing –
While exploring promotional offers and deal shopping websites, I came across Dream Deals Shop Explorer included among curated resources – Nice website experience overall, where pages opened smoothly and content felt genuinely helpful today with fast loading and clean interface design.
Charlesmeeds –
In my browsing of motivational content websites I came across a platform that encourages users to turn dreams into action through structured inspiration Vision Action Hub – the website helps users start building their goals today by offering clear guidance and supportive motivation that promotes consistency discipline and real progress in life online
BurtonDuefs –
Many digital audiences value platforms that feel lightweight and efficient, with layouts that help them find information quickly and without confusion UrbanShift UX Flow – UrbanShift offers a smooth interface where navigation is simple, allowing users to browse pages easily and enjoy a comfortable and efficient experience overall.
Williamced –
During my exploration of content platforms I came across Insight Trail Navigator – the interface felt intuitive and well balanced, offering clear navigation paths and a pleasant reading flow that supports discovering information without unnecessary effort or distraction for general users online today
Thomasrurgy –
canadian pharmacies shipping to usa: Easy Canada Meds – Easy Canada Meds
JeremyMeP –
While exploring online marketplaces I found a website that delivers a smart shopping experience with fast browsing, simple structure and a user friendly design for easy access Smart Online Deals Hub – the website feels smooth and practical, helping users quickly find products, explore offers and shop efficiently through a well organized online system
StevenVor –
While searching for learning inspiration websites, I discovered Fresh Perspective World Hub which offers well structured articles and smooth browsing experience that feels intuitive – fresh viewpoints shared here help broaden understanding every day naturally and consistently over time
GeraldScems –
Those interested in self improvement often seek guidance that is both encouraging and practical, helping them navigate challenges while maintaining focus on long term goals and aspirations steadygrowth keepgrowingforward – this kind of encouragement helps individuals build resilience and maintain consistent effort in their personal journey
Robertcen –
Some websites become difficult to follow after only a few paragraphs, yet this one stayed comfortable to read because the formatting remained clean and the information was arranged logically from one section to another online today. daily curiosity hub – The updated articles and balanced presentation made browsing the platform feel pleasant and consistently easy for readers throughout the session.
Alberteteva –
People interested in updating their wardrobe choices frequently look for online tools that highlight clothing combinations in an easy to understand and visually structured format Modern Wardrobe Atlas making fashion exploration more enjoyable and efficient overall – Trending outfits are grouped in a way that helps users quickly understand how different styles work together in real life.
DavidWer –
In the context of modern online shopping behavior, users often mention platforms that improve product discovery, and one example is Ultimate Shop Discovery Hub which is typically portrayed as a simple and engaging site that allows users to browse efficiently and find new items with ease.
AntonioMar –
People who value readable product descriptions and uncomplicated layouts could probably enjoy everyday shopping link because the site appears designed with simplicity in mind, making it easier for visitors to absorb information naturally while moving through categories without unnecessary distractions or confusing wording patterns.
Spencertewag –
Many online shoppers interested in trendy product collections enjoy platforms with clean organization and practical browsing structures, and daily deals portal – creates a smooth shopping flow that allows users to compare selections easily while exploring categories in a visually balanced environment overall.
RufusTange –
Many creators looking to enhance their artistic abilities often search for platforms that provide both structured guidance and inspirational material, and they frequently encounter resources such as Imagination Journey Spot which support creative thinkers by offering organized inspiration, structured exercises, and tools that encourage long term artistic development and exploration – Encourages imagination and structured creativity for continuous artistic growth.
Kevinmob –
I spent some time comparing knowledge sharing platforms before opening exclusive learning connect – The platform felt structured and user friendly, and the content was interesting, allowing easy browsing without confusion or overwhelming design elements online.
DavidLyday –
Appreciate the share. Learn more by clicking: this page
Georgelum –
During my browsing for lifestyle ideas, I found Style Living Aura Hub which provides a visually balanced interface and smooth navigation flow that feels natural – the atmosphere is nice and relaxing, and browsing is visually comfortable throughout the entire platform
Lonniehap –
Shoppers who want to make informed decisions in daily purchases often search for clarity focused resources, especially when they encounter simple value guide that explains product comparisons in a straightforward manner, helping users navigate different categories with ease while maintaining a calm and efficient browsing experience throughout their decision making process.
Brucecride –
In my recent browsing of discount shopping websites I found a platform that focuses on delivering simple access to everyday savings in a user friendly format Savings Deal Hub – the website provides great offers and makes browsing feel fast, easy and very convenient for users who want a smooth and efficient shopping experience today online
Davidexilt –
During my exploration of happy themed online stores I found a platform that delivers a bright and smooth shopping experience for users Bright Joy Shopping Hub – the site feels easy to navigate and uplifting, allowing users to browse products comfortably while enjoying a positive and cheerful digital environment today across categories
GarryScutt –
While searching for curated style platforms, I discovered Simply Elegant Style Hub which offers a neat layout and smooth navigation that improves usability – stylish items are curated beautifully and make shopping feel effortless and enjoyable for users who love simplicity
JamesLem –
Users exploring informational websites typically expect fast access to content along with a layout that supports easy comprehension InfinitaLink Web Portal – structure insight – The website is designed to support user efficiency, allowing smooth transitions between sections and reducing cognitive load during browsing.
Williamdom –
During my exploration of happiness inspired online shops, I found Happy Shopping Zone Page featured among similar resources – The information felt helpful overall, and layout looks modern and very welcoming for visitors everywhere thanks to intuitive design and smooth browsing experience.
MiguelVar –
While browsing travel inspiration hubs and adventure discovery websites, I discovered Adventure Dream Path Hub featured in a curated list – The browsing experience feels great overall, with a modern design and navigation that is incredibly simple and user friendly for all visitors today.
Thomaswek –
Many bargain hunters who regularly compare prices online use dedicated tools that present organized deal information across different marketplaces such as Deal Smart Explorer – it helps users quickly identify discounted products and streamlines the process of choosing cost effective items during routine shopping activities
WilliamWaync –
While exploring online collaboration spaces, I eventually found discover learning hub – It is a strong community platform where users can share, learn, and grow smoothly, making everyday growth feel natural and consistent online.
Thomasrurgy –
reliable canadian online pharmacy: Easy Canada Meds – Easy Canada Meds
DavidGow –
Users who prefer positive and cheerful shopping experiences often look for platforms that simplify product discovery, especially when they visit joyful living store space – the website feels clean and welcoming, offering a pleasant browsing flow that helps users find lifestyle products easily while maintaining a calm and enjoyable environment throughout their session.
GeraldRaw –
People who enjoy discovering fresh perspectives online frequently appreciate platforms that make learning feel exciting and accessible, and inspired discovery lane – delivers engaging experiences that encourage users to remain curious while exploring educational and creative content in a more enjoyable way overall.
RandomNamehiexy –
During my search for motivational tools, I came across great mindset start – The platform felt positive and welcoming, and page navigation was smooth and natural, making it easy for first-time visitors to browse without distractions or complexity online.
DavidCah –
While browsing gift shopping platforms I found a website that presents gift ideas in an organized and simple layout for a pleasant shopping experience Gift Ideas Hub Store – the platform feels easy to use and well structured allowing users to browse gifts smoothly and enjoy a simple and enjoyable online shopping experience today
LarryVek –
During my exploration of digital education platforms, I found Thrive Learn Academy Space which features a clean layout and easy navigation that supports usability – the educational content helps users grow skills and confidence daily online through consistent and guided instruction
Normanamuse –
Fashion shoppers exploring various e-commerce sites frequently observe that the Everyday Elegance Shop offers a balanced design approach – its structured layout ensures easy access to categories, while the clean visual presentation enhances the overall shopping experience for users of all levels.
AntoniovEt –
When reviewing digital design platforms and interface inspiration resources, people frequently mention bold vista display page included in curated discussions emphasizing engaging visuals, structured navigation, and easy usability. – The layout feels modern, clear, and highly intuitive overall.
Eugeniosix –
Online fashion enthusiasts often search for platforms that simplify outfit selection and trend understanding, and one example is Trendy Wardrobe Guide Portal which is generally seen as a guide for modern style inspiration, curated outfit combinations, and updated fashion insights for daily wear.
DouglasWeith –
After spending some time reviewing different sources, this page was one of the few that actually felt comfortable to read because the content flowed logically and the formatting avoided the usual clutter that slows readers down online. quality information lane – The material was shared with a balanced and professional style that made the overall experience feel smooth and well prepared today.
DavidLyday –
Nice read. See for yourself here: this website
Jeffreynut –
While browsing innovation and future development websites, I found Tomorrow Build Strategy Hub included among similar platforms – Impressed with the organization today, where locating useful sections felt quick and refreshingly simple with a clean layout and easy browsing experience overall.
Ernestget –
Individuals seeking aesthetic upgrades for their homes often turn to inspirational sources that highlight balance and creativity, and websites such as freshdesigndaily freshdesigndaily offer thoughtful ideas that enhance modern interiors while maintaining comfort, usability, and long lasting visual appeal in everyday spaces.
DannyVency –
Users navigating uncertain decisions in fast-changing digital spaces frequently depend on structured assistance systems where clarity compass tool – offers simplified orientation by organizing scattered information into clear directions, allowing individuals to better understand available possibilities and reduce decision fatigue during complex research processes.
TimothyHousy –
Many online shoppers appreciate platforms that balance aesthetics and functionality when showcasing discounted product selections browsing deal station – A station like browsing concept where products are displayed neatly, allowing users to explore offers in a smooth and visually structured environment designed for ease of use.
mostbet_oiel –
mostbet kifizetés visa [url=www.mostbet2024.help]www.mostbet2024.help[/url]
mostbet_eyea –
mostbet crash стратегия [url=http://mostbet45631.help]mostbet crash стратегия[/url]
melbet_mqPt –
melbet кэфы [url=http://melbet15928.help/]http://melbet15928.help/[/url]
Thomasrurgy –
Easy Canada Meds: drugs from canada – maple leaf pharmacy in canada
Bryangib –
During casual browsing for stylish discounts, I discovered Fresh Style Offers Hub which features a clean and organized layout that enhances usability – the platform offers trendy fashion deals with great prices and variety available everywhere today for everyday online shoppers
Carlosseene –
When discussing how modern buyers evaluate different online marketplaces, some examples are used illustratively, including explore Pure Choice catalog which is frequently mentioned in descriptive contexts as a model of structured browsing systems, highlighting how categorized product presentation and simplified interface design can support a smoother shopping journey for users seeking variety and convenience.
Jerrynum –
Visitors to informational websites often appreciate when content is arranged logically and supported by simple navigation elements. GrandLink online guide – The GrandLink online guide style helps improve usability, ensuring users can follow sections easily and locate information without difficulty.
Larrymof –
I usually move quickly through pages like this, but the structure and readability here made me stay longer because every section flowed naturally and the content remained easy to follow without sounding repetitive or overly technical today. easy networking source – The overall presentation felt polished and engaging, giving the platform a stronger and more dependable appearance compared with similar websites online.
AlbertHig –
Consumers looking for stylish and functional lifestyle content often appreciate resources that combine clarity with appealing presentation, and style ideas station – supports easier discovery of modern concepts by organizing content clearly and maintaining a visually balanced layout throughout the browsing process.
DavidLyday –
Nice share. Take a look at this: this page
Benniewen –
Individuals who enjoy self-growth content frequently search for uplifting material that can improve their mindset and emotional outlook during daily routines and challenges Positive Living Guide offering guidance that helps maintain clarity and motivation throughout the day while building healthier thought patterns – This resource focuses on encouraging small positive actions that gradually shape a more balanced and fulfilling lifestyle through consistent inspiration
WilliamHah –
Anyone planning to refresh their interior spaces usually benefits from browsing inspiration that balances creativity with practicality for real home settings Interior Spark Studio – such ideas support gradual improvements, helping users visualize changes that enhance comfort, functionality, and overall atmosphere in a natural and achievable way.
JamesDus –
While exploring discount shopping platforms and deal discovery websites, I found Pro Deals Savings Network included within curated listings – Great browsing experience overall, with content quality appearing consistent and nicely maintained throughout recently, offering smooth navigation and a clean, user friendly layout today.
Dennisneatt –
During casual exploration of gift idea platforms, I came across Gift Creativity Online Hub which presents items in a visually appealing and structured format – the site is a perfect spot for unique gifts and includes many creative ideas available online for shoppers
RandomNamehiexy –
Individuals who want to stay focused on continuous improvement can benefit from progress mindset hub which provides inspiration and structured ideas that support steady development, helping users build resilience and maintain forward movement even when facing challenges or uncertainty in their personal growth journey.
Michaeltib –
In reviewing personal growth websites and guides, I found Rapid Mindset Builder listed among productivity resources – The site includes several interesting sections, and the design feels clean, welcoming, and well structured, making it easy for visitors to understand content quickly.
RobertVut –
People browsing online systems often expect intuitive navigation tools and layouts that allow them to reach content quickly without frustration or delay VertexSky Clean Access – The SkyVertex design offers a smooth browsing experience with clear structure and simple navigation, ensuring users can access content efficiently across all sections.
Davidexine –
While browsing e-commerce websites I discovered a platform that provides a good selection of products with smooth navigation and a clean organized interface for shopping Best Corner Shop Hub – the platform feels practical and modern, guiding users to find items quickly, view options clearly and complete purchases with ease
Thomasrurgy –
cheapest online pharmacy india: top 10 pharmacies in india – no rx needed pharmacy
Davidpep –
While searching for styling advice platforms, I discovered Fashion Style Updates Hub which offers a neat interface and organized sections that enhance browsing clarity – fashion updates and styling tips make browsing enjoyable very much by helping users stay current with trends
ArronDiz –
For individuals focused on innovation and idea development, innovation thinkers hub provides structured inspiration and collaborative insights – it encourages users to engage with modern thinking approaches while improving creativity and developing stronger problem solving strategies across different areas of interest.
OllieNat –
In reviewing e-commerce savings and promotional offer websites, I discovered Super Deals Insight Hub featured among curated listings – The platform felt smooth to use, pages loaded quickly and navigation worked perfectly everywhere today, making deal browsing simple and enjoyable.
Raymondparma –
Users exploring tech websites generally expect fast performance, clear structure, and minimal distractions that allow them to focus on content easily LinkCraft RapidView Portal – LinkCraft provides a well-optimized experience where pages load quickly and navigation remains simple across all sections.
RobertSoale –
As I was checking online stores for affordable household items I came across value explorer site – The platform performed reliably, pages opened quickly, and the product descriptions were clear enough to make understanding each offer simple and efficient throughout my browsing today.
Rickyworry –
People interested in expanding their knowledge often value platforms that encourage curiosity and engagement, and curious mind portal – delivers inspiring content that helps users explore topics actively while developing a more focused and learning-oriented mindset overall.
JasonGep –
During my browsing of self improvement platforms, I found Stay Motivation Power Hub which features a neat interface and well organized structure – motivational content keeps energy high and mindset strong every day helping users build strong habits
JeffreyCloft –
People looking for stylish and exclusive online finds can explore luxury elegance hub which showcases curated high quality products and refined selections – helping users discover premium items that reflect sophistication exclusivity and modern luxury appeal across fashion lifestyle and accessory categories.
Thomasrurgy –
Easy Mex Meds: Easy Mex Meds – affordable pharmacy
AntonioToisp –
During an evening session of browsing fashion inspiration websites I visited style exploration hub – The platform felt visually attractive, and discovering useful fashion details was simple, smooth, and enjoyable throughout my time spent on the site today.
Robertbiony –
During my search through creative inspiration and idea development platforms, I found Modern Creative Concepts Hub featured among curated listings – The website felt pleasant overall, with discovering interesting content smooth and naturally engaging today thanks to well structured categories and simple browsing flow.
JasonIcema –
Many digital explorers appreciate systems that organize suggestions into meaningful pathways, and they may encounter Explore Sphere in curated guides – the rewritten comment explains how it provides a broader perspective on available options and improves browsing clarity across multiple categories.
Carrollpat –
While searching for personal style websites, I found My Fashion Zone Style Hub which offers a clean layout and well organized sections that improve usability – personal style ideas make fashion exploration fun and very useful for exploring new clothing combinations
StephenNek –
People interested in expanding intellectual creativity often explore idea expansion hub which offers structured inspiration and cognitive tools aimed at broadening thought processes and improving mental adaptability – enabling users to generate more innovative solutions while developing consistent habits of reflective and strategic thinking over time.
JamesSon –
Many websites attempt to appear creative but quickly become repetitive, although thought provoking portal feels much more engaging because the material encourages curiosity and leaves visitors interested in exploring more content during future browsing sessions online.
Thomasver –
In reviewing online shopping inspiration hubs and product discovery sites, I discovered TrendStop Flow Guide featured among curated recommendations – The browsing experience felt clean and modern, with fast category navigation that was refreshingly simple and easy for users today.
WilfordTible –
Many online visitors prefer platforms that reduce clutter and instead focus on clean organization that enhances readability and supports effortless navigation UrbanScale Interface Hub – UrbanScale delivers a visually structured experience where balanced layout design ensures users can browse easily and understand content without unnecessary distraction.
Antoniomum –
When individuals look for motivation to improve their life path, the concept of Life Renewal Beacon serves as guidance – it represents hope, direction, and the steady light of progress that encourages continuous self-improvement and personal evolution.
Nathannaw –
During my browsing of personal development resources, I discovered daily growth space – which offers uplifting content designed to inspire users daily, keeping their motivation strong and their focus on continuous self-improvement and positive thinking.
pinup_vfKi –
pin-up deposit [url=http://pinup27096.help]http://pinup27096.help[/url]
FreddieFaf –
While exploring curated e-commerce platforms, I discovered Trendy Style Gallery Hub which provides a modern and well organized interface that highlights products beautifully – I am impressed by the stylish presentation and everything appears carefully selected for quality and aesthetic harmony
mostbet_tjSa –
mostbet aviator kirish [url=https://mostbet61870.help/]https://mostbet61870.help/[/url]
aviator_opsn –
aviator mines Malawi download [url=www.aviator84217.help]www.aviator84217.help[/url]
mostbet_zzPn –
мостбет электронный кошелек [url=mostbet64830.help]mostbet64830.help[/url]
JesusShise –
While browsing various online deal discovery and offers platforms, I came across a section featuring Great Offers Finder Hub which stood out for its clarity – Nice layout here, everything seems organized carefully and easy understanding for newcomers today with smooth navigation and clearly structured categories throughout the experience.
Thomasrurgy –
india online pharmacy: Easy India Meds – online pharmacy without scripts
Williamhoile –
Students and self learners seeking direction can explore knowledge success path which offers curated learning materials and structured guidance – helping individuals build consistency, stay motivated, and achieve academic and personal goals through gradual improvement and effective study strategies applied over time consistently.
BruceVialp –
After checking several related websites this evening, this one stood out because the explanations remained concise and the design focused on readability instead of unnecessary distractions that often interrupt the browsing experience online today. easy browsing center – The fresh updates and clean organization helped create a very comfortable and enjoyable reading experience from beginning to end today.
DavidBug –
While reviewing branding inspiration collections and UI showcase examples, people often mention brand crest insight portal included in discussions focusing on structured identity design and accessible browsing experiences across digital platforms. – The interface feels modern, clean, and pleasantly easy to use.
GlennShisa –
During my search for leadership inspiration sites I came across a platform that promotes creativity, inspires action and helps users become better leaders in life and work Inspire Lead Creativity Hub – the website feels empowering and structured, guiding users to generate ideas, take initiative and build strong leadership qualities
CharlesBex –
I recently spent time comparing online creativity platforms and eventually found balanced online collection where the material feels approachable and the content structure helps visitors follow along naturally while exploring different educational and creative ideas online.
Jamiespurl –
During my search for lifestyle simplification resources, I came across Everyday Ease Network which offers clear and useful information presented in a neat layout – the browsing experience remains smooth across all sections and everything feels easy to access
Jamestweby –
People who regularly consume digital content for educational or informational purposes often prefer sources that feel organized and predictable, and they may rely on trusted-data-stream – which is commonly seen as a consistent provider of structured content that helps users stay informed in a calm and straightforward manner.
Thomasscops –
Many digital shoppers appreciate websites that turn routine browsing into a calm and enjoyable experience without pressure or urgency Casual shopping day page – providing a relaxed interface where users can explore different products comfortably while enjoying a smooth and pleasant online shopping journey throughout the day.
Jasonmow –
While reviewing motivation and self improvement platforms online, I discovered Unlock Your Potential Hub included in curated resources – Smooth experience browsing here, where information looked reliable and nicely presented throughout the website with organized structure and easy usability.
Williaminviz –
Consumers looking for budget-conscious online experiences frequently prefer websites that emphasize simplicity, transparency, and easy product discovery without overwhelming layouts SimpleValue Market supporting a cleaner browsing journey that reduces friction – This variation describes how practical digital platforms enhance user comfort by focusing on clarity and functional design over unnecessary complexity.
EddieKIP –
While researching lifestyle and interior upgrades, I came across home styling resource – the platform delivers a calm and accessible experience, allowing users to comfortably explore different decorating approaches and practical suggestions for improving living spaces in a visually pleasing way.
Thomasrurgy –
Easy Mex Meds: Easy Mex Meds – Easy Mex Meds
Davidboage –
People evaluating online platforms usually focus on how clearly information is structured and how easily they can navigate through different sections without confusion or delay HorizonPure Navigation Hub – The PureHorizon interface feels fresh and minimal, offering users a calm browsing experience where content is easy to explore and visually organized in a simple way.
Patrickabaxy –
A number of modern websites overload visitors with unnecessary information, though simple inspiration hub seems to focus more on meaningful writing and engaging articles, creating a pleasant atmosphere for visitors interested in thoughtful discussions and easy to follow content online.
Conradbom –
During an extended session browsing shopping and product recommendation websites, I found daily value corner embedded in a recommendation section, and the experience felt useful since browsing sections were smooth and naturally organized across all categories.
DanielZed –
While searching for updated product catalogs online, I came across Buy Collection Network – listings feel well maintained, and the interface gives a sense of order and reliability for frequent visitors who appreciate structured browsing systems on platform usage
DavidInobe –
I spent part of the afternoon exploring partnership networks before finding simple partnership guide – The platform felt well organized, and the content was engaging and easy to follow, allowing visitors to navigate without unnecessary distractions or complex layout issues online.
RandomNamehiexy –
During my search through online deals and shopping value websites, I came across value choice site included in a recommendation block, and the platform felt really useful as everything was organized well and easy for visitors to browse different sections efficiently.
JeffreySquak –
During a session of reading self growth content and mindset reset guides, I found New Dawn Beginnings Network naturally included in the article – Starting fresh feels easier now, thanks for this awesome space, and it gave me the push I needed to start again with a clearer and calmer mindset
DennisKab –
While going through various online platforms that highlight everyday recommendations and light browsing content, I noticed a section featuring Daily Browse Spot placed within the main text flow that felt naturally aligned – The overall experience was smooth and enjoyable, with quick access to simple and practical daily ideas.
PeterLex –
Individuals trying to build better mornings often look for gentle guidance that helps them start the day with intention, and they visit easy morning flow tips which share practical ideas for creating calm routines, improving focus, and maintaining steady energy throughout the day without unnecessary pressure or complication.
Thomasgrene –
While browsing various lifestyle improvement websites and digital magazines for ideas, I noticed the section was particularly organized and helpful because Lifestyle Hub Guide – Everything seems arranged nicely, and finding important sections was surprisingly easy for newcomers exploring content for the first time today with minimal confusion and clear navigation structure overall.
MatthewNam –
While reviewing online concentration and focus improvement websites, I discovered Focus Track Vision Hub included among curated listings – Appreciate the clean structure here, where browsing through pages felt comfortable and straightforward today with organized content and easy usability.
ClydemeT –
My idea stayed unfinished until I gave it proper direction using BuildIt Online Studio which helped me organize everything in a way that made execution simple and achievable – I’ve finally launched my project and it feels incredibly fulfilling
Brianhat –
People interacting with web platforms often appreciate when navigation is simple, predictable, and supported by a clean design that reduces cognitive load during browsing NexaVision Interface Hub – The NexaSphere platform integrates usability and modern design principles effectively, offering a smooth digital experience where clarity and performance remain consistently prioritized throughout usage.
LeroyDit –
While exploring online platforms about meaningful living, I found value creation guide – which provides thoughtful insights that inspire users to focus on building projects and habits that contribute positively to their long-term happiness and fulfillment.
Ramironic –
People who enjoy browsing lighthearted fashion and decorative online shops often seek platforms that feel cozy, pastel themed, and visually soothing while still offering modern trendy items for everyday use Daisy Cove Boutique Collection – it feels like a sweet curated space with adorable items that make browsing enjoyable and relaxing, encouraging repeat visits for casual shopping moods
mostbet_lySl –
mostbet mobil versiya [url=http://mostbet02759.help/]mostbet mobil versiya[/url]
Jamesdwefe –
Users who enjoy luxury items often carefully plan purchases to ensure they feel meaningful and worth the investment over time Dream Buy Premium Watch Hub – I found my dream watch here after months of saving, and it was totally worth it because it felt like a personal milestone that I was finally able to achieve
Dannycof –
While comparing different online retail stores, I found that some had cluttered layouts, but savings style hub offered a clean browsing interface with fast loading sections and easy navigation that made shopping more enjoyable and simple for all users.
MatthewGluri –
While checking various creativity blogs and online idea hubs, I noticed artistic inspiration hub placed within curated content, and I really enjoyed exploring recently because the content felt fresh and visually comfortable throughout with easy navigation and clean design.
AlvaroDenry –
Many users searching for high-quality stylish products appreciate websites that keep layouts simple and elegant, and elegance browse point – offers a refined shopping experience that helps visitors find premium items more easily while maintaining a smooth and visually attractive interface overall.
RobertSwemi –
People who build consistent habits often include small enjoyable activities in their mornings, like coffee and browsing, to create a more positive and stable daily rhythm Morning Habit Hub – My morning ritual has become coffee and browsing here daily, and it honestly makes waking up feel much more enjoyable than before
Thomasrurgy –
Easy Mex Meds: Easy Mex Meds – mexican drugstore
StephenHurge –
Earlier today I was checking different trading education sites before opening modern trader academy – The platform felt helpful and well structured, and the layout stayed simple and easy to understand, allowing users to learn without confusion or overwhelming design features online.
DuaneUnece –
During casual exploration of learning websites, I came across Interactive Learning Corner which delivers content in an engaging and user friendly style that encourages active participation – the overall experience feels inspiring and perfect for anyone interested in building knowledge and generating new creative ideas
Michaeltow –
Before finally moving into my first apartment I spent evenings scrolling through home ideas and stumbled upon starter apartment design hub which offered simple but effective decorating tips – it helped me picture how I want my rooms to look in detail planning style now.
Lloydrhift –
During a casual review of personal growth blogs and motivation focused platforms, I found Vision Empowerment Network naturally included in the article – Finally feeling heard, your vision really does matter here, and it provides a sense of validation that helps strengthen confidence in personal ideas and long term plans
Dustinkat –
In browsing fashion trend platforms and lifestyle inspiration websites, I came across Style Matters Knowledge Base included in a recommendation list – Enjoyed checking this website, pages loaded quickly, and the information felt genuinely useful with a clean and structured browsing experience today.
GeraldNah –
Keeping my wardrobe updated is something I enjoy but I always try to make practical decisions so I don’t go beyond my spending limits, and while looking for inspiration I found Everyday Style Market which helped me see many affordable outfit ideas – It gives me confidence in choosing clothes that look good while still being budget friendly and easy to manage
MichaelOxife –
During an evening session exploring online creativity tools and idea generation websites, I came across a platform that featured Creative Flow Space naturally inside its article section, making the browsing experience feel smooth and organized – The page delivered a calm and inspiring experience, with fresh ideas flowing easily through each section I explored.
KellyAlema –
Many aspiring leaders look for structured environments that encourage motivation and creativity Growth Mindset Lab helping them build stronger habits while focusing on leadership development and purposeful action in everyday life situations.
RandomNamehiexy –
While checking various online savings and deal comparison platforms, I noticed daily savings portal embedded in curated content, and the experience felt useful as everything appeared well structured and easy for visitors to browse across multiple categories.
Waynehathy –
Users who think they are not creative often discover otherwise when they engage with supportive learning platforms designed for beginners Unlock Hidden Creativity Studio – I didn’t know I could draw at all, but their advice helped me try and I genuinely surprised myself with how natural it started to feel after a few attempts
ThomasDah –
During a casual browsing session across idea and creativity-focused websites, I found innovation concept guide placed inside a recommendation block, and the experience felt pleasant since pages open quickly while information stays clearly arranged across categories.
JeffreyDiT –
People who appreciate artistic and low key online shops often stumble upon curated marketplaces while browsing for aesthetic and creative items Drift Orchard Secret Shop the atmosphere feels soft and inviting – it truly feels like finding a hidden gem on the internet filled with charming and thoughtfully crafted selections
GeraldTaK –
Users who appreciate gentle happiness often focus on small purchases that add comfort and positivity to their environment without requiring major lifestyle changes Gentle Joy Hub – I picked up a plant and a mug and it showed me that small joys are truly what matter most in everyday life experiences overall
Leroywible –
Several online communities often discuss websites with easy navigation, and among those suggestions I noticed organized browsing source which appears designed to keep things simple and accessible for visitors who want a straightforward and comfortable browsing experience.
BuddySoulk –
After checking several shopping value websites, I discovered smart deals hub – The browsing experience felt easy and pleasant, and products were displayed clearly in an organized and visually appealing way without clutter or confusing navigation online.
JamesVog –
In a fast changing world where distractions are common and focus is often difficult to maintain, many individuals turn toward helpful online resources such as clarity-growth-center – these platforms encourage reflection reduce mental clutter and help users regain control over their goals by reinforcing structured thinking and purposeful daily habits.
Davidlew –
During browsing of personal growth blogs and opportunity expansion platforms, I came across Discover Opportunity Hub placed within the article structure – Opens up so many doors, and I never thought I’d find this, since it made me realize how many new directions I can take if I stay open minded
WilliamAmest –
In my search for goal oriented websites I came across a platform designed to help users create a better future through planning, motivation and personal development strategies Future Planning Inspire Hub – the website feels supportive and clear, helping users set direction, stay focused and build habits that lead to long term success
Jamesdar –
While looking for engaging educational content for my child, I found a website that focuses on interactive learning experiences, designed to make studying feel more like play and less like a task Fun digital kids academy – My daughter loves the kids section because it provides engaging activities that help her learn new skills while enjoying colorful visuals and simple challenges that keep her motivated daily.
Williamfup –
During my recent search for helpful comparison platforms, I discovered Options Discovery Portal which offered well organized content and straightforward layout, making it easy to follow different sections – overall the experience felt practical, with clear information that supported better understanding during browsing sessions
DanielQuarl –
While exploring curated online fashion stores and minimalist outfit platforms designed for daily wear, I discovered Bright Style Wear Hub embedded within the content flow – Simple elegant picks here make it perfect for everyday casual wear, giving a clean and effortless look that works well for both relaxed and slightly polished outfits
Jamesdus –
During a quiet evening at home I explored multiple shopping blogs before stopping at fashion picks hub – The website gives a polished impression overall, content updates appear frequent, and navigating through different pages feels responsive, simple, and enjoyable for visitors using any modern browser today.
ShaneInfit –
During a session of exploring idea sharing platforms and digital creativity spaces, I found Concept Creativity Zone – The platform is full of unique concepts everywhere, and it keeps me returning for more daily because it consistently delivers fresh inspiration for different creative needs.
JefferySic –
Users who like efficient shopping experiences often prefer platforms that make every step from payment to return easy and stress free Daily Shopping Ease Zone – checkout is fast and simple, returns are easy to process, and I would definitely shop here weekly because everything feels practical and well optimized
RandallStito –
Individuals exploring innovative thinking often value resources that help them begin building ideas confidently, and creative spark hub – provides inspiring content that encourages users to start new initiatives and focus on turning imagination into practical and meaningful creations effectively.
WilliamOnemi –
While checking different online discount offer websites, I noticed smart deal hub embedded within curated content, and the browsing session felt great overall as visitors can easily navigate different categories without confusion across pages.
Curtisson –
Users who like practical home improvements often look for shelving that is both strong and aesthetically pleasing, helping them maintain a clean and functional living environment without sacrificing design quality Smart Home Shelves Hub – I finally got shelves that don’t look cheap and the build quality is extremely sturdy, which makes them perfect for everyday use around the house
KevinBow –
https://freshpharm24.com/ reliable online pharmacy
Rogermoina –
While exploring various online fashion and urban lifestyle platforms earlier today, I eventually discovered urban fashion hub placed within a curated recommendation list, and I enjoyed checking it recently because the design feels modern and extremely comfortable for smooth browsing across all sections.
AlbertElale –
During a late night search for trading education sites, I eventually visited trusted trade hub – The platform felt informative and structured, and everything was updated and easy to access, making navigation smooth and quick without clutter or overwhelming design elements online.
Stevenheend –
People drawn to refined artistic collections often appreciate stores that maintain strong material quality alongside expressive color themes Garnet Stone Creative Vault offers a curated selection where craftsmanship feels solid and rich tones enhance the aesthetic experience, making browsing feel both inspiring and dependable
ArnoldNib –
During exploration of streetwear marketplaces and urban clothing platforms focused on affordable fashion trends, I found Street Urban Style Outlet Hub naturally included in the article – Cop some nice streetwear pieces, prices are actually fair too, and it feels like a great place to shop without worrying about overspending
AngeloToupt –
Anyone interested in well maintained and diverse online content may appreciate creative update platform because the site offers a wide range of topics that feel fresh and professionally managed, making it easy for visitors to stay engaged while browsing.
KevinTag –
Many people struggle with rising monthly bills and look for practical approaches to manage their finances more effectively, which is why I recently explored different strategies and came across useful advice on smart savings hub that helped me rethink everyday spending habits and reduce unnecessary costs significantly over time.
KennethCob –
Choosing outfits used to take me forever until I discovered Look Style Navigator and followed the recommendations – it simplified my wardrobe choices and gave me a structured way to build outfits that actually make sense together.
Jamesaceta –
While exploring various personal development and productivity platforms online, I came across a section featuring Vision Matters Hub which stood out due to its clarity – Helpful platform here, discovering different sections felt smooth and very convenient overall with intuitive navigation and well structured categories that made browsing easy for first time users today.
Stephenedign –
People who like saving money while traveling often search for resources that make trip planning easier and more enjoyable without lowering the quality of their experiences Passion Travel Tips Hub – these travel guides helped me plan a surprisingly smooth budget trip that turned out enjoyable, well organized, and far more affordable than I initially expected when I started planning
Gregoryjindy –
While searching for exploration inspiration online, I found Awaits Discovery World Hub which offers a well structured layout that supports easy browsing – the website feels inspiring today and encourages visitors to explore new possibilities and embrace new experiences confidently
Mariomet –
During an afternoon of browsing online marketplaces and discount tracking platforms, I stumbled upon Bargain Explorer Hub – Managed to secure a great deal earlier today, and it really improved my shopping mood while helping me cut down expenses on items I needed.
LewisAnamI –
In the middle of exploring creativity and innovation content, I found imagination boost page – which shares helpful reminders to stay creative every day and encourages users to develop original ideas in their daily activities.
FrankWhatt –
Browsing modern ecommerce sites often involves checking how well each platform balances design quality with usability and responsiveness for everyday users across devices now Trend Fusion Storefront Online Style Access – The platform offers a clean and responsive layout that enhances user engagement through updated visuals and structured content presentation for everyone today consistently.
TeodoroElump –
Users who like feel good content often search for websites that provide small daily reminders of positivity, helping them feel more relaxed and uplifted during ordinary moments online Positive Vibes Content Hub – I smiled at least three times while reading their posts because the simplicity of the content makes it feel genuine and unexpectedly effective in a comforting way
Georgenix –
People who enjoy exploring online retail often look for curated platforms that highlight emerging styles and seasonal collections especially when browsing trendy fashion outlet – the website presents a clean modern layout that makes discovering new arrivals feel smooth and visually organized while giving users a comfortable shopping flow overall without confusion
Jeffreytrita –
During exploration of productivity optimization blogs and habit building systems, I came across Daily Micro Change Network embedded within the article flow – Small smart changes daily create a huge difference over time, and it showed me how powerful small consistent actions can be when applied regularly
Rodneyacess –
I had been searching for beauty product outlets before discovering daily glow outlet – The website looked beautifully designed, and browsing products felt smooth and enjoyable every visit, allowing simple exploration without clutter or overwhelming design features online.
KevinBow –
https://freshpharm24.com/ pharmacy websites
Vernonped –
Shoppers interested in floral drift inspired rustic aesthetics often look for online boutiques that combine soft motion inspired visuals with earthy design harmony Floral Drift Stone Boutique the store feels airy and gently artistic with balanced textures – it creates a calming shopping experience where drifting floral beauty and rustic stone elements merge into a visually soothing and creatively elegant environment
EdwardBup –
I was reviewing my weekly plans and looking for inspiration when I crossed paths with content tied to Dream Scaling Resource and it fit perfectly into my reflection process – after that moment I naturally started pushing myself toward more ambitious and structured personal targets.
EdwardgeF –
People interested in handmade crafts often use inspiration platforms to develop skills that allow them to produce high quality gift items at home Handcraft Ideas Hub I made handmade gifts for friends and they thought they were store bought due to how polished they looked – Made handmade gifts for friends, they thought I bought them professionally
RandomNamehiexy –
Users who enjoy educational variety often rely on platforms that present different facts every day to keep learning interesting and consistently engaging Knowledge Refresh Hub – every visit gives me one new fact that keeps my brain engaged, and I enjoy how it turns simple browsing into a learning experience without effort
MichaelSew –
During an afternoon of browsing e-commerce websites, I discovered modern shopping portal where the layout feels very organized and clean, allowing users to quickly browse products in a convenient way without wasting time searching through cluttered or poorly arranged sections.
RobertPaype –
Many people searching for inspiration online appreciate platforms that make discovering ideas feel effortless, and idea flow center – delivers a smooth interface where users can browse creative content easily while enjoying a clear and engaging layout throughout the platform overall.
Stevenaddip –
While exploring various online trend and style platforms, I discovered trend hub paradise included within curated recommendations, and the browsing experience felt great overall because everything loaded quickly across all devices and worked seamlessly during navigation.
AndrewTwero –
While checking different e-commerce trend analysis sites and fashion update blogs, I noticed Future Trend Hub integrated naturally into the content flow – Spot on trends here, way ahead of other stores honestly, and it gave me a clear sense of what styles are rising before they become widely available elsewhere
RobertJuick –
During my exploration of motivational websites focused on personal growth strategies I encountered Achievement Climb Site highlighted within a curated list of development tools that seemed quite promising and practical – the overall interface feels polished, user friendly, and thoughtfully maintained with recent updates improving usability making navigation easier for new visitors seeking structured guidance today.
HaroldGlady –
While browsing digital shopping platforms, I discovered Fresh Choice Product Hub which presents items in a neat and structured way that supports easy navigation – the product selection is diverse and browsing feels pleasantly simple and convenient throughout the entire experience
Anthonygop –
Users who enjoy cozy home aesthetics often look for simple items that bring warmth and personality into living spaces without needing major redesign or effort Cozy Corner Living Hub – getting a plant and a mug made my room feel more inviting and emotionally uplifting, reminding me that small joys can completely change a space
RogerOvarm –
While exploring multiple online idea discovery platforms and unique websites, I discovered innovation uniqueness portal included within curated recommendations, and I was impressed with the layout as browsing remained simple and enjoyable throughout all pages.
Derekvag –
During a casual session of exploring online marketplaces for everyday products and household essentials, I found Everyday Smart Picks Network embedded within the article section – Solid picks for daily needs, never disappointed with my choices, and it has made my routine shopping much easier by offering consistently reliable product options
Andrewclisk –
After checking several trading websites, I discovered smart trading hub – The information felt useful overall, and the structure was clean and professionally maintained, making it easy for users to understand without clutter or confusion online.
Gabriellon –
After struggling with applications for months, I finally refined my approach using advice from Career Boost Guide and noticed immediate improvements in my CV structure and confidence, which eventually helped me secure better responses and move closer to real interview invitations than before.
RonaldGem –
Fashion lovers who follow trending styles often search for online stores that showcase popular items seen across influencers and social platforms where new looks spread quickly and gain attention Viral Style Finder Hub – got the viral jacket everyone is talking about, and it instantly made my outfits feel more modern, trendy, and aligned with what people currently consider fashionable
Michaelbluse –
People who start over professionally often realize that fear is temporary but regret from not trying lasts much longer New Start Collective I switched careers at thirty five and it felt overwhelming, but now I see clearly it was worth it – Switched careers at thirty five, scary but so worth it now
RobertCravy –
Shoppers who prefer minimal and pure aesthetic brands often look for products that feel fresh, simple, and naturally balanced in design Quartz Orchard Fresh Aura Market – the experience feels clean and calming, offering crisp and pure products that support a refreshing and mindful lifestyle approach for everyday usage and comfort
Thomasscops –
Online visitors often prefer simple and calming shopping experiences that do not overwhelm them with too many choices at once Daily Leisure Shop site – designed to give users a relaxed way of exploring items while maintaining a smooth and enjoyable browsing flow throughout their entire shopping session online.
NormanSob –
People looking for motivational and insightful online content may enjoy self discovery hub because the platform offers fresh ideas and helpful perspectives that encourage visitors to reflect on their abilities and take meaningful steps toward personal development and growth.
Timothyhep –
While exploring different curated gift websites and unusual product collections for special occasions, I found Hidden Gem Gift Portal integrated within browsing sections – I bought a gift nobody else had, such a great find that it instantly made the moment more meaningful and memorable for the person receiving it
Howardfak –
Users who value speed often look for shopping platforms that simplify the process from browsing to checkout, making it easier to handle daily needs efficiently Instant Shopping Hub – This store feels like a grab and go solution, ideal for busy weeks when I just want to get what I need quickly and keep moving
AlbertblinI –
While checking different online shopping inspiration pages for ideas, I found Next Trend Shop Hub which stood out among similar sites for clarity and structure – Browsing this website felt simple, layout stayed clean and easy to understand throughout the visit today with no confusion while navigating sections.
Michaelsex –
While checking out different digital storefronts, I encountered Urban Deals Outlet which had a neat structure and smooth browsing flow that made moving between categories easy and pleasant – I like how the platform maintains clarity in design and supports a stress-free browsing experience overall
Carlossow –
People who enjoy discovering new lifestyle updates often prefer platforms that highlight trends in a simple and engaging way, especially when they visit trend discovery daily hub – the site feels smooth and modern, making it easy for users to explore content and stay updated without unnecessary distractions or complicated navigation.
Jamesleast –
During an extended search for motivation and inspiration websites, I noticed inspiration stream portal placed in the middle of a recommendation list, and the shared information felt helpful while navigation stayed smooth, simple, and easy for first-time users browsing the content.
Edwardfal –
During a session of exploring e-commerce product curation tools and wishlist platforms, I noticed Favorite Picks Organizer Hub integrated into the article – Bookmarked several items already, coming back for more later, and it has made managing interesting finds much easier than keeping random notes or tabs open
RandomNamehiexy –
People who enjoy reliable online suggestions often look for platforms that consistently provide strong recommendations that work as expected across different categories Consistent Picks Hub – their recommendations never miss, I’ve tested three already and all of them have delivered exactly what was promised
Wesleycok –
While browsing different gift idea websites, I eventually noticed smart gift corner – The collection felt interesting overall, and finding unique products here was effortless and convenient, allowing users to shop easily without clutter or complex interface elements online.
ThomasCow –
Many individuals searching for fashion inspiration often appreciate platforms that keep updates simple and well structured, and modern outfit hub – delivers fresh style content that allows users to explore ideas easily while enjoying a clean and visually appealing layout overall.
AlfonsoVop –
People often try different motivational tools online hoping for something useful but rarely expect a real shift in perspective during casual discovery sessions life improvement hub – I ended up pleasantly surprised because it offered more meaningful insight than I thought it would when I first opened it without expectations
CarlosKIG –
People who frequently visit informational websites often appreciate when everything feels orderly, particularly when they encounter platforms such as together growth portal that provide helpful and professionally maintained content, making it easier to absorb information without unnecessary effort or confusion during browsing sessions.
BernardSerne –
During a late night browsing session for motivational content, I found personal growth library – The platform was neatly organized with easy to read sections, making it enjoyable to explore different learning materials focused on self development and confidence enhancement.
Williamthoxy –
While researching social impact websites, I came across a platform that shares powerful and emotional volunteer journeys Better World Stories portal featuring individuals contributing to global and local change – After reading them, I decided to start volunteering in local initiatives that focus on education and food security programs.
narkologicheskii stacionar_yfSl –
лечение в наркологическом стационаре [url=https://narkologicheskij-staczionar-sankt-peterburg-13.ru]лечение в наркологическом стационаре[/url]
ChesterDig –
During a casual browsing session for inspiration websites, I discovered modern discovery guide – The platform was thoughtfully designed with a clean layout, making it easy to navigate while everything felt modern, organized, and enjoyable to explore today.
Robertpem –
People focused on personal achievement often look for structured motivational systems that help them stay consistent, build confidence, and achieve meaningful career milestones over time Dream Achievement Path Hub – I used their guidance and manifested a promotion, which felt surprising at first but eventually became a very real and rewarding experience in my professional life
Scottacari –
While browsing through various fashion related websites online, I came across trendy style hub and noticed the presentation feels very polished, making the browsing experience enjoyable and visually satisfying for visitors exploring different fashion ideas and categories across the platform in a smooth way.
ArnoldLal –
As I explored different online shops for heartfelt and meaningful present ideas, I discovered a lovely boutique page that caught my attention gift happiness corner – I selected a perfect gift for my mom that made the experience feel warm and fulfilling.
Williamuseri –
During a session of exploring social growth platforms and positive community spaces, I found Grow Together Network placed within the content section – It genuinely feels rewarding to be part of this, as the supportive environment makes sharing ideas and progress feel natural and encouraging every time
Matthewhib –
During a casual exploration of online fashion hubs, I came across creative style fashion guide – The platform offers a really nice fashion selection and smooth browsing experience overall today, making navigation simple, stylish, and enjoyable for users.
mostbet_txmi –
мостбет crash 2026 [url=https://www.mostbet58019.help]мостбет crash 2026[/url]
mostbet_fcKl –
mostbet kazino yutugi [url=http://mostbet75681.help]mostbet kazino yutugi[/url]
melbet_cqei –
мелбет кыргызстан официальный сайт [url=https://melbet72804.help]https://melbet72804.help[/url]
JamesDak –
During a casual review of fashion inspiration websites and minimalist style shopping platforms, I found Simply Chic Style Network naturally included in the article – Clean and elegant style, doesn’t try too hard honestly, and it delivers a subtle aesthetic that feels natural and very easy on the eyes while browsing
Reabilitaciya alkogolikov_vvpa –
платный нарколог на дом москва [url=https://reabilitaciya-alkogolikov-moskva-1.ru]платный нарколог на дом москва[/url]
MarioKet –
While searching online for fashion matching ideas, I came across Perfect Look Wardrobe Finder Hub which features a modern interface and simple navigation that feels user friendly – it helps users discover outfits that match their personality really easily and encourages confident styling decisions
KevinBow –
https://freshpharm24.com/ reputable overseas online pharmacies
Jesselax –
People who enjoy browsing random sites often discover unique platforms that feel exciting enough to share right away with others Amazing Discovery Point Hub – I stumbled upon this gem and already recommended it to several friends because it felt useful, fun, and worth sharing with anyone who enjoys discovering new online experiences
WilliamCen –
After comparing a variety of related pages this evening, I found this one noticeably more approachable because the writing style stayed natural and the layout avoided the cluttered appearance that often makes browsing frustrating and time consuming online. elegant online picks – The presentation remained professional and easy to follow, helping every section feel organized and enjoyable to explore from start to finish.
Reabilitaciya alkogolikov_doer –
вызов нарколога на дом круглосуточно [url=https://reabilitaciya-alkogolikov-moskva-2.ru]вызов нарколога на дом круглосуточно[/url]
JeffreyRorgo –
Digital shoppers increasingly value simplicity and speed when searching for promotions, and smart offer finder provides a consolidated way to explore various deals efficiently – feedback often emphasizes its usefulness in reducing browsing time and helping users quickly identify worthwhile savings opportunities that match their everyday shopping needs
GrantLizot –
While thinking about taking a break from routine life and exploring new places, I started browsing travel inspiration content that turned out to be more helpful than expected adventure planning guide – I’m currently piecing together a travel plan and discovering different scenic locations and tips that are making the whole process feel more engaging and less stressful than usual.
PatrickMob –
While browsing different online analytics and growth tools, I eventually noticed trusted signal hub – The platform felt fast and efficient, and everything loaded quickly without clutter, making it easy to explore content without distractions or unnecessary design elements affecting usability online.
Robertciz –
Many fashion enthusiasts who prefer online shopping experiences often look for websites that provide both variety and ease of navigation, and one frequently discussed example is Pure Style Collection which is typically described as offering broad clothing selections along with modern fashion inspirations suitable for different personal styles and seasonal updates.
RichardWex –
After exploring multiple websites related to recommendations and trending topics, I eventually discovered reader friendly source highlighted among popular suggestions, and the platform provided a clear layout that allowed visitors to locate useful content efficiently without confusion while browsing different categories online.
RandomNamehiexy –
In my effort to stay aware of what’s trending across lifestyle, tech, and culture topics, I started using a source that presents updates in a very digestible format for everyday reading Trend Pulse Hub – It helps me stay informed without feeling disconnected from current events, giving me exactly the kind of light but consistent awareness I was looking for.
Zacharyhor –
People trying to build discipline often need reminders that progress starts with action, not planning, especially when they are stuck in cycles of delay and uncertainty Action Mindset Hub – I stopped waiting for things to happen and started doing them myself, and this really pushed me forward in a powerful way
Richardferse –
While exploring online knowledge and information websites, I came across smart helpful hub corner – The website had useful content and a smooth browsing experience, making navigation simple, enjoyable, and well organized across all pages.
DonaldAcupt –
While reviewing various online motivation hubs and personal growth platforms, I came across a section that featured Motivation Always Shop Link embedded naturally among recommended resources embedded naturally among recommended resources making it easier to discover related content without extra searching effort – Smooth navigation and consistent visual hierarchy help users stay focused, though deeper articles may require more exploration to fully benefit
JamesLom –
While exploring online choice and variety-based platforms, I came across modern decision space – The platform delivered great selection options with easy navigation, ensuring a smooth and enjoyable browsing experience throughout all sections.
Robertoknice –
While exploring daily inspiration platforms and mindset development resources, I found Morning Momentum Hub naturally placed in the content flow – I now read this every morning, keeps me going strong, and it has become an essential part of my routine that helps me stay motivated and mentally sharp
DavidBuh –
In my search for online discount hubs I discovered a platform that delivers daily deals and shopping promotions in a clean and user friendly interface for all users Deal Zone Smart Daily – the platform feels quick and useful, helping users find savings opportunities and enjoy a more efficient shopping journey overall
DavidNub –
While browsing affordable shopping websites and online outlet stores offering consistent quality across all purchases, I found Fresh Value Shopping Hub placed within the content section – Great bargains every time, and the quality stays consistent across orders, which makes it easier to trust what I’m buying without second guessing
JasonThish –
Shoppers who enjoy dreamy aesthetic retail experiences often seek stores that feel soft and magical, and they come across Dreamy Cove Sparkle House and like it – the theme creates a gentle glowing atmosphere that makes browsing feel relaxing, imaginative, and visually enchanting throughout
RonaldZek –
People interested in digital teamwork often look for platforms that combine education with collaboration and creative interaction Connect Build Learn Hub – I found new online friends here and learning together feels amazing, as it creates a strong sense of community and shared growth while working on creative projects
BobbyMub –
During casual browsing of product discovery sites, I discovered Smart Shopping Picks Hub which provides a structured interface and smooth navigation that feels intuitive – smart shopping experience includes useful product suggestions for everyone online improving decision making for shoppers everywhere
Jeffreylit –
Compared with many crowded and overly complicated websites online, bright idea website feels easier to appreciate because the atmosphere remains calm and optimistic, while the content encourages visitors to continue exploring without becoming overwhelmed by excessive distractions or difficult wording patterns.
DavidVot –
Online customers often search for platforms that make browsing simple while keeping product information organized and accessible for smooth experience daily use SwiftShop Arena helping users navigate through various online sections with ease and improved clarity across product selections – This description shows how streamlined shopping systems improve usability and user satisfaction.
narkologicheskii stacionar_gpSl –
наркологический стационар в спб [url=https://narkologicheskij-staczionar-sankt-peterburg-13.ru]наркологический стационар в спб[/url]
BernardSerne –
During a late night browsing session for motivational content, I found personal growth library – The platform was neatly organized with easy to read sections, making it enjoyable to explore different learning materials focused on self development and confidence enhancement.
Lowellwresy –
I was exploring different platforms to upgrade my skills for better career opportunities when I came across Career Learning Path and it guided me through step by step lessons that felt relevant, actionable, and easy to follow even without prior advanced knowledge.
Douglashap –
Consumers aiming to stretch their budgets usually explore websites that organize daily deals and present them in a more accessible and easy to understand format Everyday Discounts Guide – Provides structured deal listings and practical saving tips that support users in making better financial decisions during routine online shopping activities
Reabilitaciya alkogolikov_mapa –
вызов нарколога цена [url=https://reabilitaciya-alkogolikov-moskva-1.ru]вызов нарколога цена[/url]
Kevinvok –
While comparing a few online stores for household essentials earlier this week, I ended up spending extra time browsing through daily value picks because the categories felt intuitive and the product descriptions actually sounded practical instead of exaggerated marketing copy – The overall layout felt efficient, browsing stayed hassle free, and everything appeared thoughtfully arranged for normal everyday shopping needs.
KevinBow –
https://freshpharm24.com/ international pharmacy
Robertmet –
During casual exploration of creative inspiration hubs, I found Creative Journey Studio Hub which offers a neat and organized interface that enhances readability – the design is clean across the site and the content stays naturally presented and interesting for visitors
Henryfut –
Users who love smart online purchases often search for stores that consistently offer deals on stylish footwear, making it easier to find quality items at reduced prices Smart Purchase Hub – I bought leather boots half off, and it felt like a steal because the discount was so good that I couldn’t ignore it at all
KennethChoox –
During a casual search for structured shopping experiences, I came across creative value retail guide – The platform offers a useful experience with meaningful products and clean modern layout today, making navigation simple, clear, and enjoyable throughout.
Michaelkew –
After dealing with an exhausting schedule and feeling mentally drained I was scrolling online for something lighthearted when I discovered a page called cheerful break portal which surprisingly lifted my mood and helped me unwind during the evening more than expected overall experience.
Abrahamamign –
During an online session browsing community and growth-focused websites, I found daily support space – The platform offered engaging information and a positive atmosphere, making the experience smooth, easy to navigate, and enjoyable across different sections.
Reabilitaciya alkogolikov_bcer –
нарколога на дом москва [url=https://reabilitaciya-alkogolikov-moskva-2.ru]нарколога на дом москва[/url]
Bradleydat –
People who follow fashion trends often search for platforms that combine international style inspiration into one place, allowing them to explore outfits without endless scrolling or searching elsewhere Global Outfit Hub – I love how I can discover worldwide fashion inspiration while relaxing on my couch, which makes staying stylish feel effortless and much more enjoyable every day
RichardSip –
While checking different motivational platforms and personal development tools focused on taking action without delay, I noticed Move Forward Action Hub integrated naturally into the content flow – I stopped overthinking and acted, best decision I made recently, and it really helped me break out of hesitation that was slowing my progress
Robertlilky –
After browsing various online communities and recommendation pages focused on trending topics, I encountered general information portal among highlighted suggestions, and the responsive design together with fast page transitions created a smooth experience while exploring multiple categories and recently updated sections online.
ShaneJah –
While exploring online shopping trend platforms and fashion discovery hubs, I found Modern Trend Stop Network integrated into the article – There is cool stuff everywhere, and my friends always ask where I shop because the styles always feel distinctive, fashionable, and noticeably more appealing than standard stores
Herbertrar –
While analyzing several curated online marketplaces designed to enhance shopping efficiency and improve product discovery for users seeking structured browsing experiences, I found Your Trendy Market Guide placed in a central content position that improved readability and helped maintain a steady browsing experience while moving through different product categories and recommendations – The platform offered a clear and structured flow, making exploration feel natural and uncomplicated
VincentGam –
While browsing for home transformation ideas inspired by autumn landscapes I discovered a thoughtfully designed platform that highlights seasonal beauty in a subtle way chestnut coast style hub – The overall presentation encourages cozy living spaces filled with warm hues and natural decorative accents
EdgarIcoth –
I sometimes search for affordable online shops and during that process I found a helpful shopping platform at Happy Buy Center which offers a very pleasant experience and easy navigation – I always end up satisfied because purchases feel safe and the products match expectations perfectly
Terrystore –
While exploring productivity and intentional living websites, I discovered Grow Intent Focus Network included among similar resources – Helpful content overall, where the website appears updated frequently and very simple navigating for visitors with well structured sections and easy navigation flow.
Haroldhoigh –
During my search for online savings websites, I came across trusted value hub – The platform appeared simple and helpful, and the updated content made it easy to browse through clearly arranged categories without clutter or overwhelming design elements online.
BrandonWrold –
Shoppers who enjoy structured and informative online platforms often prefer experiences that make product discovery easier, and one example frequently noted is Guided Commerce Experience – delivering a smooth shopping journey where users receive clear guidance and can confidently explore different products with ease.
Felixerash –
While exploring online shopping value resources, I found modern value finder guide – The website delivers good value content and useful shopping information, making navigation easy, clear, and practical for everyday users.
Timothynix –
People trying to improve their professional direction often search for tools that help simplify choices and provide clarity through structured planning and realistic goal setting Pathway Clarity Hub – My career felt fuzzy and uncertain, but now I have a clear and practical plan that helps me stay focused and move in the right direction
DavidRet –
While checking different websites related to online growth tools and optimization resources, I found myself browsing through smart visibility tools since the layout appeared practical, modern, and much more user friendly compared to many overloaded platforms available online today – The pages responded quickly and the overall presentation gave a polished and reliable impression during browsing.
narkologicheskii stacionar_oaSl –
нарколог стационар [url=https://narkologicheskij-staczionar-sankt-peterburg-13.ru]нарколог стационар[/url]
Williamfluot –
While exploring tech solutions for improving household convenience, I found a store offering practical smart devices Connected Home Solutions Hub and the browsing experience was smooth – I was convinced by the smart home section and ended up ordering multiple gadgets that I now use regularly.
Reabilitaciya alkogolikov_pbpa –
нарколог на дом круглосуточно [url=https://reabilitaciya-alkogolikov-moskva-1.ru]нарколог на дом круглосуточно[/url]
RalphIcogy –
Users who prefer streamlined shopping often look for websites that eliminate distractions and focus entirely on delivering meaningful savings and useful product offers Simple Savings Hub – just good deals with no fluff at all, exactly what I needed right now, and it made everything feel quick, simple, and genuinely useful for my situation
ArnoldVok –
Fashion focused users who follow street inspired trends often prefer platforms that make browsing effortless and visually engaging, especially when they visit city fashion studio – the site feels structured and stylish, helping users quickly explore clothing options while maintaining a clean, modern layout that enhances the overall shopping experience significantly.
Younglix –
While reviewing online lifestyle and inspiration resources, I discovered daily style space – The content was well structured and felt fresh, offering a smooth browsing experience that made exploring different ideas both useful and enjoyable throughout the session.
Felipeelene –
While browsing slow fashion blogs and sustainable outfit collections, I found Timeless Wear Collective Hub placed within the content section – The pieces here last far beyond seasonal trends, and there is no fast fashion garbage, just clothing that feels stable, stylish, and built for real everyday use
RandomNamehiexy –
discoverpossibility – Interesting platform offering creative ideas and practical resources for everyday inspiration online.
KevinBow –
https://freshpharm24.com/product/viagra no script pharmacy
Normanerown –
online pharmacy top online pharmacy
Russellnum –
While browsing through online self improvement resources and motivational articles, I noticed Momentum Mindset Space in the middle of the page – I really needed this today, feeling motivated after browsing around here and it encouraged me to take action on things I had been postponing for a while
Josephral –
Online consumers increasingly rely on curated platforms that simplify the process of finding global fashion items and lifestyle products efficiently for better shopping flow experience Fashion and lifestyle hub – A centralized hub bringing together fashion and lifestyle products from multiple global sources offering users an organized browsing experience with updated trends and curated recommendations
Patrickheito –
People searching for creative resources often find that Inspiration Hub – Helpful platform lately, everything appears accessible and easy for new visitors. The layout is described as intuitive, offering visitors a straightforward path to explore various topics, while also keeping the overall experience light, practical, and easy to understand for beginners.
SamuelRance –
I had been searching for inspiration websites before discovering great journey hub – The platform felt inspiring overall, and the layout stayed clean and enjoyable, making browsing simple across devices without clutter or confusion online.
DonaldSeigh –
During my exploration of online shopping websites I analyzed how design and checkout performance work together to create a seamless user experience for buyers brightstone fast cart and observed navigation flow carefully – The cheerful layout paired with fast checkout made the entire browsing and buying experience feel smooth efficient and surprisingly pleasant
mostbet_yget –
mostbet букмекерская контора Кыргызстан [url=https://mostbet50693.help]mostbet букмекерская контора Кыргызстан[/url]
melbet_vsKn –
мелбет пополнение элсом [url=http://melbet59738.help]мелбет пополнение элсом[/url]
RobertItefs –
While searching for self development inspiration platforms, I discovered smart growth journey space – The website provides motivational content with useful ideas and personal development focus, making browsing smooth, simple, and encouraging for users.
Reabilitaciya alkogolikov_qeer –
вызвать врача нарколога на дом срочно [url=https://reabilitaciya-alkogolikov-moskva-2.ru]вызвать врача нарколога на дом срочно[/url]
DarrenDub –
People who focus on timeless clothing often prefer minimal designs that don’t rely on branding, allowing the outfit itself to speak without unnecessary visual noise Timeless Fashion Hub – I really enjoy how there are no loud logos everywhere, just clean minimal styles that feel practical and easy to wear anywhere
CharlesBum –
Anyone interested in improving their shopping habits can benefit from platforms that consistently offer everyday essentials guide discount updates, curated essentials, and practical advice designed to help users save money while making better purchasing decisions across daily needs without unnecessary complexity added easily.
MichaelEquig –
During a long browsing session focused on career opportunities and online resources, I encountered professional growth hub, and I appreciated the clean presentation because the platform felt authentic and consistently maintained while keeping navigation smooth and visually well organized.
KellyDed –
While exploring online development and improvement websites, I found Unlock Infinite Potential Page included among curated listings – Smooth experience browsing here, where information looked reliable and nicely presented throughout the website with clean design, intuitive navigation, and well structured content sections.
JamesMam –
I recently explored multiple online shopping stores with cluttered interfaces before arriving at recommended online products where the category structure looked more organized and easier to understand than many competing websites currently online – The browsing experience remained comfortable throughout and the smooth navigation made everything feel much more pleasant overall.
Ernestodox –
Online bargain hunters often celebrate finding stores that consistently offer high quality products at lower prices Discount Elite Picks this platform repeatedly proves itself with strong deals and dependable product performance – Quality to price ratio is insane, definitely coming back for more
Davidevope –
Home styling enthusiasts often search for easy inspiration that helps them upgrade bedrooms into visually appealing environments that feel both comfortable and aesthetically refined Dream Space Ideas Hub – I used their renovation ideas and my bedroom now looks incredibly stylish and put together, almost like something you would see in a luxury home magazine
JerrodWew –
During exploration of online shopping hubs and deal focused marketplaces with useful product selections, I came across The Best Corner Discovery Hub embedded within the article flow – My go to spot now, always finding something worth buying, and it has become a dependable place where I can quickly find items that actually make sense to buy
Reabilitaciya alkogolikov_bwpa –
нарколог на дом в клинике москва [url=https://reabilitaciya-alkogolikov-moskva-1.ru]нарколог на дом в клинике москва[/url]
RonaldBrarp –
While searching for self improvement and motivational online platforms, I discovered success mindset space – The website had a clean interface and motivating content, making browsing enjoyable and encouraging repeated visits for inspiration and helpful goal setting ideas.
Stevesaivy –
During a session of exploring brain development and self improvement websites, I found Mind Expansion Learning Hub naturally included in the article – Their articles feel like a brain gym workout every day, keeping my thoughts active, structured, and more open to learning new concepts
Andrewfuerb –
While reading long form discussions on mindset and perception across different online platforms, I came across structured content that challenges conventional thinking, and within one article I found Broaden Horizons Hub naturally included which made the experience feel more insightful and ultimately reshaped how I view everyday topics in a more reflective way
Georgekit –
During a casual browsing session for online stores, I found smart favorite retail hub – The platform delivers a nice store experience with simple design and useful products today, making navigation smooth, structured, and easy for users.
RonaldFew –
After reviewing several fashion season platforms, I found daily outfit season – The website felt stylish and structured, and everything was modern and visually appealing, making browsing easy for visitors without clutter or confusing navigation online.
Randellapake –
Users who appreciate frugal shopping often search for sites that make it easy to apply multiple discounts so they can enjoy products while spending significantly less money Frugal Savings Hub – I used stacked coupons and saved forty dollars, and it felt like a surprise win that made my shopping experience unexpectedly fun and rewarding
SergioabIsh –
During an extended browsing session across idea and inspiration platforms, I found insightful perspective hub embedded in a recommendation paragraph, and the experience felt smooth since the website was clean and navigation worked perfectly across different sections today.
Arrondiera –
Anyone aiming to improve productivity and personal habits can benefit from self growth guidebook which offers motivational insights and reflective content – encouraging users to take small consistent actions that build discipline and support continuous improvement in both mindset and lifestyle choices over extended periods of time.
Williamcaups –
Users who enjoy calming digital environments often prefer stores that feel soft, slow paced, and visually comforting during night hours Soft Moonlight Cove Storefront – browsing here at night feels dreamy and relaxing, offering a soothing experience that makes product discovery feel effortless and peaceful throughout the session
Jordankar –
During an online session searching for trending shopping collections and stylish product pages, I found trending deals corner – The structure of the website was clear and easy to follow, and the smooth navigation made browsing different sections feel enjoyable and naturally engaging from start to finish.
Stephenedign –
Users who enjoy exploring new destinations often rely on structured travel guides that help them maximize enjoyment while staying within budget limits easily and effectively Explore Passion Travel Hub – these travel guides helped me organize a budget trip that felt smooth, well planned, and full of great memories without unnecessary financial pressure at any stage of travel
DavidHef –
Many teams find that dedicated brainstorming environments help transform rough ideas into polished outcomes more efficiently than unstructured discussions Innovation Workspace The brainstorming sessions conducted here resulted in my best work yet, something I would strongly recommend to any creative team – Brainstorming sessions here led to my best work yet seriously
RobertGrout –
During exploration of curated online shopping hubs and product inspiration websites, I noticed Day Shopping Inspiration Network integrated into the article – I lost track of time browsing, as there were so many cool things to see that kept me curious and engaged far longer than intended
Rodneybib –
During an afternoon search for online growth resources and helpful service platforms, I came across featured traffic assistance where the information looked well arranged and the layout felt noticeably cleaner than many overloaded websites online – The website appeared modern and browsing through different sections felt easy and comfortable for visitors throughout the experience.
narkologicheskii stacionar_evSl –
наркологический стационар в спб [url=https://narkologicheskij-staczionar-sankt-peterburg-13.ru]наркологический стационар в спб[/url]
Reabilitaciya alkogolikov_ller –
наркологическая помощь на дому москва [url=https://reabilitaciya-alkogolikov-moskva-2.ru]наркологическая помощь на дому москва[/url]
WilliamItesk –
In reviewing digital curated picks platforms and recommendation pages, I discovered Choice Picks Explorer Space featured among similar resources – The content arrangement is impressive, making category exploration surprisingly enjoyable today overall with smooth transitions and a clean browsing experience throughout.
DonaldQuoma –
During an extended browsing session across fashion inspiration sites and style platforms, I found luxury fashion edit embedded in recommendation content, and the platform felt stylish because browsing sections were smooth and visually appealing with a refined and modern design approach.
abhmabtus –
Get ready to Feel the Rush of premium online games and sports betting, with the chance to win big on a range of different slots, live games, and sports and lucky numbers markets. The RTP of Sugar Rush is 96.50%, which is strong for a high volatility slot. The theme of Sugar Rush 1000 isn’t just about sweets; it’s about an immersive experience where every detail contributes to a feeling of whimsy and joy. The animations are smooth, and the symbols are designed with meticulous attention to detail, drawing players in with their charm. Meanwhile, the upbeat soundtrack enhances the overall playful vibe of the game. We’ve been dedicated to giving you a phenomenal online casino experience that is entertaining and rewarding offering betting services for a range of online slots live games, virtual games and e-sports, as well as several sports, including football, rugby, horse racing, tennis and more. You can also bet on weekly Lucky Numbers draws– this is fixed odds betting on lotto draws
https://theagentasset.com/classic-fun-with-patrick-spins1-classic-slots-in-the-uk/
Interbet International (Pty) Ltd is licensed by the Western Cape Gambling Board as both a bookmaker and manufacturer. National Responsible Gambling Programme toll free counselling line 0800 006 008 or WhatsApp Help to 076 675 0710. The platform maintains a database of previously banned players, preventing re-registration attempts through alternative email addresses or slight name variations. Address verification cross-checks ensure single household compliance, preventing family members from claiming multiple welcome bonuses. Kingmaker is one of those online casinos that focuses on providing users with a comprehensive, all-in-one platform. You’ll be able to choose from pokies, live dealer games, and even a complete sportsbook. This review shares my experience with the site, along with some helpful information that you should keep in mind when you’re considering whether or not to gamble on this website.
KevinBow –
https://freshpharm24.com/product/priligy online drugs order
Normanerown –
Fresh Pharm 24 online pharmacy no prescription needed
Jamesinhip –
In the middle of a long week filled with hesitation and unfinished plans that kept piling up, I started questioning why I keep delaying the things I genuinely want to build, Forward Motion Desk gave me clarity in that moment – and eventually today became the moment where I chose progress over procrastination and felt surprisingly good about it
LeslieBlusa –
While browsing modern home and lifestyle trend websites online, I found daily interior style space – The website featured a stylish collection of ideas and an easy navigation structure, making browsing smooth, enjoyable, and visually engaging throughout.
ZacharyHEM –
While checking out different online marketplaces and shopping platforms for everyday products, I noticed Trusted Cart Zone integrated naturally into the content flow – Every purchase has been smooth, no complaints so far yet, and I have found the overall process consistently easy, with no issues during ordering or delivery experiences
JoshuaCoify –
While browsing online fashion style and shopping websites, I found modern style marketplace guide – The website provides modern styling ideas and smooth shopping experience for visitors online, making the experience easy, elegant, and pleasant throughout the platform.
EdwardLal –
Users who enjoy creative shopping often explore mystery bundles that combine surprise and usefulness, making each order feel like a rewarding experience Creative Finds Hub – I tried the mystery box option and it was surprisingly good, giving me items that I didn’t expect but ended up appreciating a lot
DonaldPoemi –
While browsing different fashion and trend platforms, I eventually noticed daily style hub – The platform felt smooth and intuitive, and the latest trends were clearly arranged, making it simple to access content quickly without confusing layouts or distractions online.
Stephenaxory –
People interested in flexible careers often look for inspiration from others who successfully transitioned into freelancing and created better work life balance through independence Flexible Work Journey Hub – leaving my old job and starting freelancing was a big decision, and this site helped me stay motivated while adjusting to a completely different way of working
Michaelgalry –
People who enjoy reliable and easy digital shopping often choose platforms that reduce friction in browsing and checkout, and one example is Smooth Shopping Essentials Site – delivering a dependable experience where users can quickly discover products, navigate categories effortlessly, and complete purchases with confidence in a stable and user friendly environment.
OscarSoold –
After browsing through various online marketplaces today, I eventually discovered structured vendor studio hub, and the experience felt really pleasant, with carefully arranged products and easy navigation across all sections of the site.
StuartTub –
During a longer browsing session across multiple websites today, I explored modern petal corner platform and found the browsing really smooth, with clearly organized categories and a genuinely user friendly website experience overall.
Ellisviark –
Many beginners exploring design tools often find that guided workshops make learning software like Photoshop much easier and more approachable than trying to learn alone Creative Learn Hub I joined a workshop recently and picked up Photoshop basics quickly, which made me feel more confident using design tools already – Joined a workshop last week, learned photoshop basics super fast
PatrickHaide –
During exploration of online engagement platforms and supportive community networks, I came across Growth Connect Community Hub placed within the article section – Met wonderful people here, and the community feels genuine and supportive, making it a reliable space for positive interaction, learning, and meaningful social connection
Terryodock –
While exploring different online collections focused on aesthetic products and cozy themed designs I came across a charming website that felt like a sweet escape from routine browsing cozy caramel collection and I found myself scrolling longer than expected – The atmosphere felt soothing visually pleasing and gently uplifting making the entire experience feel like a small pleasant break from daily routine
Thomasvot –
Shoppers comparing products across different categories often noted how helpful it was to have fast-loading pages and clearly structured sections during their browsing process purchase navigator while reviewing deals and featured items – they felt the platform maintained excellent organization and responsiveness throughout their entire experience online.
KermitWrope –
https://freshpharm24.com/product/priligy medicine online order
Thurmantub –
While reviewing ecommerce stores connected to household and lifestyle products, I eventually found convenient product showcase where the categories looked cleaner and the overall presentation felt easier to navigate than many competing websites online currently – Everything seemed properly organized and the browsing experience remained comfortable enough to return again sometime later.
RandomNamehiexy –
During exploration of online hobby discovery platforms and personal growth websites, I noticed New Horizons Curated Hub integrated into the article – Found hobbies I never considered, and it has made life feel richer, more engaging, and filled with refreshing new ways to spend my time
StevenGlync –
While searching for informational exploration platforms online, I discovered daily discovery space – The website delivers interesting content with engaging structure and easy browsing flow, making navigation smooth, fast, and enjoyable across all pages.
MarcusWetly –
Users interested in personal growth often experiment with routine changes that improve energy levels and focus, especially during early hours when productivity habits have the strongest long term impact Productivity Reset Hub – I completely changed my morning routine and it surprisingly made me feel more productive almost immediately after just a few days of consistency
Clydeter –
During my search through online gift recommendation websites and inspiration platforms, I discovered Gift Finder Perfect Page included among curated resources – The platform felt great today, pages opened fast and everything felt thoughtfully designed throughout with clean structure and easy browsing experience.
CharlesDuh –
While reviewing several organized browsing platforms and online inspiration collections, I found popular inspiration network – The website offered a clear structure, visually pleasant content presentation, and categories that were simple to explore while searching for fresh ideas and useful inspiration online.
JamesWer –
During an online browsing session for simple living platforms, I found calm simplicity space – The content was organized nicely and the website felt comfortable to browse, making the experience smooth and easy throughout the visit.
Glennmen –
Earlier today I explored several websites dedicated to innovation and creative resources before finding helpful concept platform, where I discovered multiple interesting details and the overall experience stayed simple and enjoyable while navigating through different sections of the site.
DonaldBic –
Shoppers who value clarity often search for stores that present only meaningful deals, avoiding unnecessary clutter and making it easier to quickly find what they actually need Pure Value Deals Hub – just good deals without any fluff, exactly what I needed right now, and it felt great to shop without being distracted by unnecessary offers or confusing promotions
Williammom –
generic viagra online pharmacy without prescription
MatthewNup –
I spent the evening exploring discovery platforms before discovering modern interest hub – The website felt smooth and user friendly, and categories were clearly arranged, making navigation easy without confusion or clutter affecting the browsing experience online.
GerardoRet –
People who enjoy discovering new fashion trends online can explore diverse selections trendy outfit discovery hub curated apparel and accessories designed for modern everyday styling and seasonal fashion updates – the marketplace helps users stay current while building a more expressive and personalized wardrobe over time
Michaelbom –
While checking different e-commerce deal platforms and promotional offer websites, I noticed Discount Treasure Hub integrated naturally into the content flow – There are steals everywhere, my wallet stays happy and so do I, because I always manage to find better deals here compared to regular online stores without much effort
AnthonyDiday –
Many individuals discover that changing their outlook on daily habits can transform even the simplest parts of life like waking up early Fresh Outlook Space I used to dread mornings, but now I wake up with energy and anticipation that I never thought I would have – Used to hate mornings, now I wake up excited somehow
ThomasHoutt –
After browsing through various online marketplaces today, I eventually discovered structured collective echo hub, and I found it a nice website overall, with thoughtfully presented products and pages loading quickly without issues.
DouglasCug –
Many individuals searching for organic inspired decor prefer platforms that emphasize texture, simplicity, and a calming visual atmosphere in their collections Organic Texture Boutique – it creates a soothing environment through its product selection, making it easy to design spaces that feel balanced and naturally inviting.
KevinBow –
https://freshpharm24.com/ medicine online
Shannonpiopy –
During my review of online shopping websites, I found a site that feels clean and highly responsive, and MeadowGoods mystic marketplace offers smooth browsing overall – The pages load fast, the layout is organized, and users can explore products comfortably without interruptions or usability issues affecting the experience.
Andreskaw –
While reviewing several online inspiration hubs and productivity tools, I noticed a website that placed Momentum builder site within its main content area, making the browsing experience feel structured, fluid, and visually consistent from top to bottom
RandomNamehiexy –
During exploration of mindfulness blogs and gratitude oriented online spaces, I came across Moments Matter Awareness Hub embedded within the article flow – Makes me appreciate small things more, and the mindset shift feels real, gently changing how I respond to everyday situations with more patience and awareness
Claudgak –
While exploring online idea discovery platforms, I found smart creative space – The website presents unique items and creative ideas in a simple layout, making the browsing experience smooth, clear, and easy to enjoy throughout.
Normanerown –
viagra top online pharmacy
Matthewdob –
People who compare online deals regularly often notice when pricing feels artificially inflated, so finding a store that avoids that completely can feel surprisingly trustworthy Trust Price Hub – The name checks out perfectly, it genuinely feels like pure value with no markup games or hidden pricing tactics being used at all
MarioMaw –
I had been reviewing several digital marketplaces and service platforms before eventually finding organized ecommerce center where the categories looked clearly arranged and the information felt straightforward for regular browsing online – The website provided useful content consistently while the overall browsing experience remained smooth and reliable throughout my session.
Stevengaw –
During my review of online retail websites, I came across a platform that feels structured and easy to use, and Frost Lane Emporium shopfront offers smooth navigation overall – Everything is organized clearly, pages load quickly, and users can browse comfortably without distractions or clutter affecting usability.
RandomNamehiexy –
happyhomefinds.click – Great platform for home hunting, very smooth browsing experience today.
RogerPoogy –
While reviewing online fashion inspiration and trend platforms, I discovered trendy style gallery – The page design was visually appealing and well organized, offering useful content that made browsing enjoyable, smooth, and engaging across different sections and categories.
Calvinsheef –
People who enjoy timeless elegance often look for curated fashion collections that avoid excess while maintaining a polished and graceful appearance Classy Finds Pure Elegance Store – the designs embody understated luxury, giving a calm and sophisticated feel that enhances style without ever becoming overwhelming or visually loud in presentation
Edwardtep –
After reviewing multiple recommendation sites, I landed on simple choice hub – The platform felt helpful and reliable, and the content was professionally arranged, making it easy for readers to navigate without distractions or unnecessary complexity online.
OllieWex –
In exploring future oriented learning and building platforms, I discovered Future Path Builder Network featured in a curated list – The organization felt strong, and finding useful sections was quick and refreshingly simple with smooth navigation and a well arranged interface throughout today.
NormanBig –
Many users who spend time online looking for useful information often appreciate platforms that simplify exploration and introduce them to engaging content regularly Daily Insight Navigator Curated Discovery Flow – it helps users explore new ideas efficiently and encourages consistent interaction with informative and inspiring online materials every single day
JeffreyWrafe –
While casually exploring internet platforms and online collections during the day, I visited cleanly designed web source and found the organized categories and smooth browsing flow especially pleasant and comfortable for extended browsing sessions.
Myronnuago –
During browsing sessions focused on lifestyle trend platforms and digital inspiration websites, I came across Modern Trend Lifestyle Network placed within the article structure – Keeps me updated on trends without feeling overwhelmed at all, and it presents everything in a smooth, easy to follow format that never feels cluttered
Davidcom –
As I continued reviewing websites connected to motivation and online publishing trends, I encountered resourceful inspiration hub among highlighted recommendations, and the latest content updates paired with stable performance created a very natural browsing experience without slowdowns while exploring different sections available there.
CameronJew –
During my recent online apparel order, I found a store that made returning and exchanging items extremely simple and convenient Fashion Swap Return Center and everything worked as expected – I exchanged multiple items for different sizes and the entire process was smooth without any complications or stressful steps involved at all.
Freemanflego –
During a search for organized shopping websites and online browsing platforms, I discovered easy shopping hub – The layout was clean and well structured, and the content was displayed clearly, creating a smooth browsing experience that felt practical, engaging, and easy to use throughout the session.
Claudetiess –
While exploring inspirational and artistic websites online, I came across creative discovery guide – The platform shared inspiring creative ideas with practical resources, making browsing smooth, enjoyable, and valuable for users seeking daily online inspiration.
Williamlew –
During a session of exploring global trading marketplaces and online goods platforms with varied inventory, I noticed Creek Harbor Product Trading Network integrated into the article – Quality goods here, shipping was faster than expected too, and it made the entire ordering process feel efficient, simple, and surprisingly consistent in delivery performance
JasonDon –
I spent part of today reviewing different online stores and eventually landed on recommended echo marketplace hub, and I enjoyed the platform overall, with clean layout and navigation that stayed very comfortable from start to finish.
Dominicnop –
Users who appreciate smart living often search for platforms that showcase clever gadgets that make everyday life easier and more efficient in unexpected ways Smart Living Gadget Hub – I found a gadget I had never seen before, and now I can’t live without it because it has completely improved how I manage daily tasks
Jeffreybeice –
While searching for clean and airy design inspiration online I stumbled upon a gentle website that felt visually relaxing and easy to browse airy textile meadow point which I navigated for a while enjoying its soft palette and minimal layout style – It felt like a calm spring afternoon with soft winds moving across peaceful natural fields
CoreyTycle –
Many online readers searching for curated knowledge often appreciate platforms that organize topics clearly and present information in a simple accessible way modern ideas hub making discovery smoother and more practical for everyday users who prefer structured browsing experiences overall and find the information presentation easier to follow without confusion.
MichaelBraks –
After comparing multiple ecommerce websites this morning, I eventually explored trusted product listings where the categories seemed thoughtfully arranged and the browsing process felt smoother than several competing stores online today – The overall experience remained comfortable and the website pages loaded rapidly without unusual issues appearing during navigation.
Shannonpiopy –
During my review of online marketplaces, I noticed a site with strong usability and fast response times, and Meadow Mystic goods market offers a smooth browsing experience overall – Pages load quickly, the layout is clear, and users can explore products without unnecessary distractions or confusing interface elements.
JeromeShugh –
While analyzing lifestyle and creativity focused websites online, I noticed a platform that feels clean and intuitive for readers, and Trendy Living Hub delivers a smooth browsing experience overall – The design is modern, categories are well structured, and users can explore inspiring lifestyle ideas without distraction.
Jackiedib –
While comparing different shopping websites, I eventually opened modern shopping hub – The shopping experience felt nice today, and products were shown clearly and attractively throughout the website, allowing users to browse easily without clutter or confusing layout elements online.
Leonardwab –
During a casual search for useful online platforms, I discovered creative essentials info hub – The platform offers helpful practical content with an enjoyable browsing experience that feels simple, smooth, and easy to navigate across different sections.
TimothyDop –
New web enthusiasts often search for beginner friendly guides that make learning practical and rewarding instead of overwhelming Start Building Online Studio – I created my first website with their support and felt extremely accomplished today, like I had taken a real step forward into the world of digital creation and design
JimmySak –
Online shoppers who prefer exploring rare and interesting items can use uncommon finds directory which gathers niche products and creative selections from various sources offering users a simplified browsing experience – helping them identify unique items that are often overlooked in mainstream marketplaces and retail platforms.
KevinBow –
https://freshpharm24.com/ online pharmacy
RobertAnorn –
During exploration of online education tools and continuous learning platforms, I came across Explore Knowledge Achieve Network embedded within the article flow – Learned something new today, already applying it to work, and it has already made my workflow smoother and more efficient than before
Jamesprosy –
During an online search for shopping and discovery websites, I found daily shop discovery space – The platform provides a great shopping experience with interesting finds and smooth navigation here, making the experience simple, clear, and pleasant across all sections.
DennisMum –
While reviewing e-commerce platforms and product discovery websites, I found Perfect Shopping Zone Network featured within similar resources – Helpful browsing experience overall, where layout appears clean and navigation remains very intuitive everywhere today with easy access to categories and smooth page flow.
JamesDew –
During exploration of rustic lifestyle websites and cozy inspired shopping platforms, I came across Caramel Stone Mountain Hub embedded within the article flow – Cozy vibes all around, it reminds me of peaceful mountain retreats, and it brings a soft calming feeling that feels like a natural place to unwind and relax
Stanleyverse –
People using recommendation tools often find podcasts that feel like hidden treasures and quickly become part of their routine listening Everyday Discovery Hub I came across a podcast I’m now fully obsessed with and I never miss an episode – Discovered a podcast I’m obsessed with, thanks for the recommendation
Randallbit –
Users who enjoy streetwear fashion often prioritize hoodies that offer both insulation and style, helping them build layered outfits that still look clean and modern during colder months Street Warmth Hub – These hoodies are thick and warm, and they work perfectly for winter layering looks that actually feel practical and stylish at the same time
Normanerown –
Fresh Pharm online pharmacy
Larryutefe –
During comparison of online shopping websites, I noticed a platform that feels organized and efficient, and Collective Frost Meadow shop provides smooth browsing overall – Content is clearly structured, pages load quickly, and users can explore products easily without confusion or clutter.
Loganlanna –
People searching for chic and modern fashion with a royal touch often explore curated boutiques that feel unique, and they discover Crownstone Chic Collective – it provides a refined aesthetic that enhances personal style while keeping everyday fashion simple, elegant, and accessible.
Williamsit –
While browsing different online education hubs and informational websites, I noticed smart info guide included in a recommendation block, and the website felt informative because visitors could easily access useful resources without distractions during a clean and smooth browsing experience.
Michaelkab –
During comparison of personal fashion guidance websites, I noticed a platform that feels clean and informative for users, and Style Insight Hub provides a smooth browsing experience overall – The tips are straightforward, making it easier for users to understand and improve their everyday fashion choices.
Jerrysuets –
While exploring different online shopping websites this morning, I spent time on valuable grove marketplace hub, and I found the layout helpful overall, with detailed information and browsing that remained simple throughout the experience.
MelvinUtign –
globaltrendmarket – Great marketplace overall, browsing different sections feels smooth and straightforward for everyone.
Michaelciz –
People exploring new digital tools often highlight the importance of usability and responsiveness, particularly when visiting resources such as entryway portal where the interface remains smooth, pages adapt well to screen sizes, and browsing feels comfortable even during longer reading or exploration sessions online.
RandomNamehiexy –
pixelharvest – Great looking website design here, information feels updated and naturally well presented.
HaroldChiff –
While reviewing online marketplaces, I came across a platform that feels simple and structured, and Urban Petal product showcase delivers smooth browsing experience overall – The interface is clean, items are well organized, and users can easily find products without unnecessary complexity or distractions.
JamesFex –
After comparing a few different websites during my research earlier today, I eventually came across quality shopping reference and noticed that everything from the navigation menus to the loading speed felt impressively refined, making the website appear consistently maintained and very user friendly overall.
Brianblino –
While searching for self development and motivational websites, I discovered momentum start corner – The content was easy to follow and thoughtfully organized, offering practical ideas that help users build consistent habits and stay inspired in their daily activities.
CraigTheat –
Users who love discovering new creative concepts often appreciate platforms where content flows continuously and feels engaging rather than overwhelming Creative Ideas Flow Center – endless scrolling here actually feels good, full of imagination and inspiration that makes me want to keep exploring because every section brings something fresh and interesting to discover
RalphKaw –
Students and educators seeking modern inspiration tools frequently explore online platforms that provide structured brainstorming support such as Idea Generation Studio – enabling collaborative thinking, improving ideation speed, and supporting a wide range of creative disciplines from writing to design and multimedia production processes
Richardlal –
While exploring online success and self growth platforms, I came across a href=”[https://startsomethingawesome.click/](https://startsomethingawesome.click/)” />smart success guide – The platform had a motivating tone and smooth website performance across all pages, making browsing simple, fast, and enjoyable throughout the entire experience.
PatrickKib –
While exploring various online deal platforms and shopping offer websites during a casual browsing session, I came across smart savings deals hub – The platform offered helpful deals and offers with clear presentation and easy browsing, making the experience smooth and convenient throughout.
WilliamUtink –
During exploration of productivity and manifestation blogs online, I noticed Create Belief Focus Network integrated into the article – Manifested a small win today, and this site helped me focus by reinforcing a positive mindset that made goal setting feel more achievable and grounded
WayneVom –
Those who enjoy clean, earth toned interior aesthetics often discover curated shops such as Minimal Earth Style Storefernstonecollective.shop – The design approach focuses on simplicity and natural harmony, with products that feel sturdy, visually calm, and carefully aligned with a lifestyle that values understated elegance and organic inspiration.
RobertCefly –
Users preparing for speaking opportunities often benefit from structured confidence advice that helps them feel ready and in control when presenting ideas Ready Speak Hub – I nailed my presentation thanks to confidence tips I found here, and it made a huge difference in how confidently I expressed myself throughout
Georgekem –
DIY enthusiasts often enjoy simple hands-on projects that bring families together while teaching practical building skills and encouraging creativity in children through guided step by step instructions Creative Build Hub I built a birdhouse with my nephew using their DIY guide and it turned out better than expected – Built a birdhouse with my nephew using their diy guide
DanielSop –
Many people prefer wardrobe staples that combine simplicity, durability, and comfort, especially when selecting clothing suitable for both work and casual environments Daily Wear Essentials Shop Daily Wear Essentials Shop – this option provides a consistently comfortable experience that works well for everyday routines, offering reliability and ease without unnecessary complexity or distraction.
Davidsed –
During exploration of fashion promotions and online shopping resources, I found a website that feels structured and welcoming for style enthusiasts, and Fashion Deal network provides a smooth browsing experience overall – Pages respond quickly, offers are displayed neatly, and visitors can enjoy browsing discounted clothing items without distractions.
Robertjap –
I spent some time exploring different online shopping outlets before discovering smart selection outlet – The website presentation felt very clean overall, and everything appeared updated and simple, making it easy to find useful products without confusion or clutter during browsing online.
RobertTum –
While exploring multiple online savings and deal websites, I discovered smart savings guide included within curated recommendations, and the browsing experience felt impressive as categories appear well organized and easy to navigate without issues.
KermitWrope –
https://freshpharm24.com/product/priligy top online pharmacy
Williammom –
pharmacy fresh pharm no rx needed pharmacy
Herbertbot –
People who like unique wardrobe pieces often prefer fashion sources that provide original designs instead of repetitive and uninspired clothing seen everywhere Fresh Fashion Wardrobe Hub – this store finally gave me clothes that don’t resemble the same boring outfits others wear, making my style feel more confident and refreshingly different
BrandonMit –
After exploring multiple online marketplaces and browsing different digital stores today, I eventually visited trusted echo harbor hub and found the website feels polished, with categories arranged clearly and content reading naturally everywhere throughout the experience.
DavidPluck –
While exploring online shopping platforms and outlet collections, I discovered daily value outlet embedded in curated content, and I really enjoyed the browsing experience because the pages were well organized and comfortable for navigating product categories easily.
KevinBow –
https://freshpharm24.com/ pharmacy no prescription required
Terrymag –
During exploration of creativity boosting websites and idea generation platforms, I came across Innovation Creative Builder Network embedded within the article flow – Got my creative juices flowing, and I built something I’m proud of, and it reminded me how rewarding it is to transform ideas into real projects
Williamchage –
While analyzing ecommerce websites, I noticed a platform that feels well organized and fast, and UrbanPetal retail store offers a smooth browsing experience overall – Pages load quickly, navigation is simple, and users can browse products without unnecessary complexity or visual noise.
RonaldWally –
While browsing digital fashion trend platforms, I discovered modern style update hub – The website provides trendy styles and useful updates for modern fashion lovers today, making navigation smooth, clean, and visually appealing throughout.
Myronlew –
Users focused on self improvement often use journaling to track positive actions and achievements, making it easier to stay motivated and mindful throughout the week Reflect & Grow Hub – I began journaling again and capturing small wins feels surprisingly uplifting, like I’m actually noticing progress instead of letting it slip by unnoticed
DavidPoids –
While reviewing several digital growth platforms this afternoon, I eventually explored simple online resources where the information looked clearly arranged and the browsing process appeared smoother than many alternatives online currently – The platform maintained a clean user friendly structure where everything felt accessible and easy to explore during navigation.
DavidWer –
People who regularly browse online stores for inspiration and convenience often mention platforms that simplify product discovery, and one such example is Discover & Shop Network which is generally portrayed as a modern browsing space designed to help users explore different categories and enjoy a relaxed shopping experience without unnecessary complexity or confusion.
Jackzes –
Reading this brought back an idea I had set aside months ago, and a stop at unlocknewpotential added more substance to that idea, content that revives dormant projects in my own thinking is content with serious creative value and this site is contributing to my own work in ways I had not expected when first clicking through.
RobertOdOmi –
While analyzing ecommerce websites, I noticed a site that feels polished and modern, and FrostPetal emporium network provides a smooth browsing experience overall – The interface is visually appealing, loads quickly, and users can browse comfortably without unnecessary complexity or distracting elements.
Normanerown –
Fresh Pharm medstore online pharmacy
Richardmaw –
During exploration of relaxation themed platforms and peaceful lifestyle websites, I found Calm Cove Stress Relief Network naturally included in the article – Relaxing brand overall, great for unwinding after long days, and it supports a mindset shift toward calmness and emotional recovery after busy schedules
Wernerhon –
Those who enjoy interior styling often search for minimalist furniture solutions online, and they discover Modern Apartment Style Co curated design inspiration that feels smooth – the sleek furniture ideas completely reshaped my space into something more refined, adult, and visually coherent that finally feels like a grown up home.
DomingoVus –
While comparing different online style resources and organized fashion browsing destinations, I discovered top outfit network – The categories were displayed neatly, the navigation process worked efficiently, and the website presentation helped make the overall experience feel relaxed and visually satisfying overall.
MauriceRip –
People interested in transforming their daily habits usually prefer platforms that combine inspiration with actionable strategies, and they might find Reality Shaping Resource offering structured insights – The content remains fresh and relevant, helping users stay focused on meaningful progress while building effective routines for personal and professional development.
Clintonthume –
While exploring online idea-based platforms and informational websites, I found modern thinking space – The content was well organized and engaging, making browsing enjoyable, smooth, and easy while discovering different structured and interesting perspectives throughout the site.
WilliamByday –
While exploring motivational content platforms, I found a website that feels simple and practical for everyday users, and Vision Mindset Guide delivers a smooth browsing experience overall – The content encourages users to develop clarity, stay focused, and move steadily toward important personal and professional goals.
RaymondGox –
People who enjoy saving money while shopping often prefer stores that help them feel like every purchase is a worthwhile investment rather than a loss Better Spend Deals Hub – getting more value per dollar spent has made shopping feel satisfying again, and my wallet actually feels healthier instead of constantly depleted
Kevinmob –
I spent part of the afternoon exploring learning platforms before finding simple knowledge share – The website structure felt clean and easy to use, and the content shared today was interesting, allowing smooth browsing without clutter or distracting design elements online.
Stevenbloor –
During my online browsing session today, I checked multiple platforms before landing on useful harbor commerce hub, and I found it a helpful platform overall, where navigation worked smoothly and information appeared clear for visitors throughout the experience.
DustinCob –
During exploration of online startup resources and motivational business content platforms, I came across Big Ideas Action Hub embedded within the article structure – Great mindset tips here, helped me launch my project quicker, and it encouraged me to stop waiting for perfection and start building immediately
Nathanmot –
While checking creative thinking enhancement tools and inspiration platforms online, I found Idea Inspiration Mind Network placed within the content flow – Sharp ideas everywhere, and it was exactly what my brain needed right now, helping me generate new concepts I hadn’t considered before in my projects
Stephenmaync –
While checking various internet shopping platforms earlier today, I came across helpful petal iron hub and noticed a great browsing experience overall, with fast page loading and products that were clearly and professionally organized throughout.
Michaelflicy –
While exploring online shopping outlets focused on simplicity and clean user experience, I came across minimal choice outlet hub – The platform offers a clean outlet experience with good selection and simple navigation online, making browsing easy, smooth, and pleasant throughout.
Wilburzer –
After reviewing several online marketplaces and catalogs today, I eventually found trusted amber oak store, and I enjoyed browsing here, with clean pages and no loading delays during the visit.
Robertnag –
Users who like being ahead in style often explore digital platforms that organize current and emerging trends in one easy place Trendy Choice Focus Hub – it helps me stay ahead of the curve, and friends often ask how I consistently keep track of what’s trending before it becomes mainstream
Stanleyned –
During browsing sessions on modern online marketplaces that combine quality and affordability, I came across Crown Cove Elegant Outpost Network embedded within the article structure – Premium feel without crazy prices, definitely ordering again soon, and the overall experience felt smooth, trustworthy, and visually appealing in a way that encourages repeat visits
Thomaswek –
Online consumers who want to maximize their budget often explore websites and applications that simplify deal tracking and highlight useful offers such as Bargain Discovery Center – it delivers structured deal listings and practical suggestions that assist shoppers in identifying better prices and improving everyday spending habits overall
JamesKic –
During my exploration of productivity websites and focus tools, I came across clear mindset hub embedded in a list of useful resources, and the platform felt helpful because its content presentation remained structured and easy for all users – Navigation was simple and comfortable throughout.
Davidillus –
I recently browsed multiple digital service websites before eventually stopping at simple optimization tools because the layout looked clear and the categories felt easier to navigate than many overloaded platforms online currently – The clean interface stood out and the services seemed helpful for regular visitors.
Davidscals –
While exploring different online growth and inspiration platforms, I discovered positive change portal embedded within curated recommendations, and the browsing experience felt smooth as sections opened quickly across all devices with stable performance.
MichaelplOfe –
During my exploration of online productivity and mindset resources, I found a platform that feels structured and user friendly for goal oriented readers, and Personal Success guide offers a smooth browsing experience overall – Pages load quickly, motivational content is presented clearly, and users can focus on improvement strategies without confusion or overwhelming design elements.
Rodneyflott –
Came in expecting another generic take and got something with actual character instead, and a look at bestpickscollection carried that personality forward, finding a distinct voice on a saturated topic is impressive and worth pointing out when it happens because most sites end up sounding identical to their nearest competitors quickly.
RandomNamehiexy –
During my search for motivational tools, I came across great mindset start – The platform felt positive and welcoming, and page navigation was smooth and natural, making it easy for first-time visitors to browse without distractions or complexity online.
Williammom –
Fresh Pharm trusted online pharmacy
Jamesesons –
While exploring online fashion lifestyle stores, I came across creative fashion outfit hub – The website had a modern design and useful information, making the browsing experience smooth, enjoyable, and visually engaging across all sections today.
KevinBow –
https://freshpharm24.com/product/norvasc reputable overseas online pharmacies
RobertoDiews –
During an online search for personal development and motivation websites, I discovered forward progress inspiration space – The platform provides motivational content and helpful guidance for personal progress every day, making navigation simple, clear, and encouraging across all sections.
melbet_knMa –
melbet apk скачать [url=https://www.melbet36091.help]https://www.melbet36091.help[/url]
mostbet_jxKn –
mostbet o‘yin translyatsiya [url=https://mostbet93504.help]https://mostbet93504.help[/url]
pinup_vqml –
pin up ilovani yuklab olish [url=pinup61802.help]pinup61802.help[/url]
DennisLah –
During browsing of innovation driven websites and modern thinking resources, I discovered Modern Concept Space placed naturally in the article – It offers fresh modern takes on everything, exactly what I was seeking, and it gave me a more practical and updated understanding of various topics I explore online
DonaldAnesy –
During comparison of online shopping experiences, I noticed a platform that feels well organized and fast, and Petal Frost store network provides smooth browsing overall – Content is neatly structured, navigation is easy, and users can browse without confusion or clutter interfering with usability.
KevinSoipt –
After spending time reviewing multiple recommendation websites and informative browsing collections, I found best browse reference – The navigation remained straightforward, the overall design looked modern and appealing, and the content structure made browsing different sections feel simple and naturally comfortable throughout the experience.
Normanerown –
Fresh Pharm trustworthy online pharmacy
Robertnag –
People who enjoy discovering new trends early often use online sources that highlight what is gaining attention in culture and fashion Trendy Choice Flow Hub – it keeps me ahead of the curve, and friends often ask how I always seem to anticipate what becomes popular next in style and lifestyle
Rogerpitle –
While exploring different web platforms earlier today, I came across organized mystic horizon collective and appreciated the clean structure, with smooth navigation and reliable website performance across all pages of the visit.
Eugeniosix –
Online fashion enthusiasts often search for platforms that simplify outfit selection and trend understanding, and one example is Trendy Wardrobe Guide Portal which is generally seen as a guide for modern style inspiration, curated outfit combinations, and updated fashion insights for daily wear.
KevinThomo –
During comparison of multiple content platforms emphasizing clarity and user experience, I came across a website that used PerspectiveVision Hub within its mid content section, and the overall presentation felt smooth, structured, and naturally organized for easy browsing
Erichtailm –
After exploring several online marketplaces and browsing different digital stores today, I eventually visited trusted amber petal hub and noticed everything looks well structured, with content easy to understand quickly throughout the experience.
BarryBus –
During an afternoon search for online marketplaces and digital service platforms, I eventually came across featured seller directory because the structure looked balanced and navigation felt smoother than many overloaded websites online today – I enjoyed browsing the platform and everything appeared neatly organized and professionally maintained throughout the experience.
Curtiswef –
During exploration of digital marketplaces for trending lifestyle items, I found a platform that feels structured and easy to browse for shoppers, and Modern Shop Trends offers a smooth browsing experience overall – The platform highlights products clearly, allowing users to explore everyday goods without unnecessary distractions.
SteveMic –
I had been checking various online resources earlier today before discovering well designed commerce portal, and the website felt modern, with neatly arranged categories and content that reads naturally throughout the visit.
JasonGef –
During a casual search for online knowledge platforms, I discovered daily insight space – The website provided informative content and useful learning material, with a clean user friendly design that made browsing smooth, easy, and enjoyable across different sections.
RobertTep –
During a casual search for modern idea platforms online, I discovered modern ideas connection space – The platform delivers creative modern ideas and useful networking inspiration for users today, making navigation simple, clear, and user friendly throughout.
Mateoelags –
The structure of the post made it easy to follow without losing track of where I was, and a look at theperfectgift kept the same logical flow going, this site clearly understands that organisation is half the battle in keeping readers engaged from the first line to the last across any kind of post.
Briangeast –
During a late night exploration of online inspiration and opportunity based platforms, I found New Path Explorer embedded smoothly in the article section – I took a chance and it paid off, highly recommend exploring since it opened up helpful ideas and gave me a fresh direction when I needed it most
MichealCheld –
Many users exploring personal development tools appreciate platforms that offer clarity, reflection, and actionable guidance in one accessible place Find Your Way Studio focuses on simplifying complex decisions and helps people feel that needed direction and found it here is more achievable than they previously believed in their daily lives
Carlosseene –
In discussions about digital shopping ecosystems and user experience design, a commonly used illustrative reference is Pure Choice Marketplace Entry which is generally portrayed as an example of how structured online platforms present multiple product selections in a clean, organized interface aimed at simplifying browsing and improving accessibility.
DavidGlirl –
During an extended search across inspiration and discovery websites, I came across possibility world portal embedded in a recommendation list, and the browsing experience felt smooth since the design is modern and easy for visitors today.
Leroyjeafe –
During my search across several digital marketplaces this afternoon, I eventually visited high quality opal collective hub, and there was a nice collection available, with comfortable browsing and genuinely informative descriptions throughout the session.
GeorgeCeM –
While reviewing online educational and inspiration platforms, I came across a site that feels clean and engaging, and Pure Outlet value space provides smooth navigation overall – The interface is minimal, ideas are clearly presented, and users can learn and create without confusion or unnecessary complexity affecting usability.
PeterVax –
While browsing different online resources for knowledge and information, I eventually explored helpful info shelf because the layout looked clean and the content felt easier to follow than many competing platforms online today – The content quality appeared strong and the website was useful for reliable information seekers.
Justinbloms –
https://stromectolvip.com/# ivermectin 6mg dosage
RandomNamehiexy –
amberpetalmarket – Smooth experience overall, categories are clearly arranged and useful today.
RogerSoimi –
While exploring stylish and luxury product websites online, I came across creative luxury shopping hub – The platform delivers luxury products and stylish finds presented in an elegant way online, making navigation easy, elegant, and enjoyable throughout.
Elmerfluby –
http://cialisvip.com/# Cialis Vip
Williamraigh –
While reviewing creativity-focused websites and inspiration platforms online, I came across artistic ideas hub – The website provided structured and helpful information, making browsing smooth, engaging, and inspiring while exploring different creative sections and learning materials.
DamienFug –
While searching for fashion inspiration and online style platforms, I discovered smart fashion space – The platform featured attractive content and a clean layout, making browsing easy, enjoyable, and smooth while exploring various fashion ideas online.
RobertAnopy –
During comparison of knowledge-based websites, I noticed a platform that feels simple and efficient, and Pine Frost resource collective provides smooth browsing overall – The interface is clean, navigation is intuitive, and users can access helpful content without confusion or clutter affecting usability.
Rogerref –
generic stromectol [url=http://stromectolvip.com/#]stromectol in canada[/url] stromectol online pharmacy
Chrisvoica –
best price for viagra 100mg Sildenafil Vip Order Viagra 50 mg online
AlbertPyday –
People who want easy everyday outfit inspiration often search for fashion guidance that is simple and functional, and they come across Style Reality Tips Store – the advice is focused on practical fashion that works in real life situations, making it easier to dress well without unnecessary stress or confusion
Davidkek –
A thoughtful read in a week that has been mostly noisy, and a look at purechoiceoutlet carried that thoughtful quality across more pages, finding pockets of considered writing in a week of distractions is one of the small wins of careful curation and this site is providing those pockets at a sustainable rate.
Robertdap –
While browsing several online shopping resources and recommendation pages earlier today, I eventually discovered daily savings corner featured among popular suggestions, and the overall website structure looked clean and organized while product details remained easy to access and comfortable to explore throughout the visit.
MarshallVor –
Got something practical out of this that I can apply later this week, and a stop at brightnewbeginnings added more details to think about, this is exactly the kind of content I bookmark for future reference rather than the throwaway listicles that dominate most search results these days for almost any common topic.
ShaneJah –
During exploration of online fashion discovery platforms and trend-based shopping guides, I came across Trendy Look Finder Hub embedded within the article flow – Cool stuff everywhere, and my friends always ask where I shop since the products always stand out and give a more modern and stylish impression compared to standard stores
OctavioEmbex –
Now feeling something close to gratitude for the fact this site exists, and a look at amazingdealscorner extended that gratitude, the rare site that produces this kind of response is the rare site worth defending in conversations about whether the modern internet is still capable of producing genuinely valuable independent content for serious adults.
Austiniders –
A piece that brought a sense of order to a topic I had been finding chaotic, and a look at discovernewhorizons continued that organising effect, content that imposes useful structure on messy subjects is doing genuine intellectual work and this site is providing that organisational function across multiple posts I have read recently here.
WesleyTew –
Found the section structure particularly thoughtful, and a stop at dreambiggeralways suggested the same care across the broader site, structural choices guide the reader through the material in ways most people do not consciously notice but feel the absence of when those choices are made carelessly or not at all.
Ianwonee –
Did not expect much when I clicked through but ended up reading the whole thing carefully, and a stop at purestylemarket kept that engagement going, sometimes the unassuming sites turn out to deliver more than the flashy ones which is something I have learned to look out for over time online lately and across topics.
RandomNamehiexy –
Anyone who struggles with procrastination and wants to develop a more active mindset may find take charge portal useful for learning how to build discipline, create structure, and maintain steady progress toward goals by focusing on consistent effort rather than delay or hesitation.
Nicotuddy –
Approaching this with the usual skepticism I bring to new sites and being slowly persuaded, and a stop at createimpacttoday continued that gradual persuasion, the careful path from skeptical reader to genuine fan is the only one I trust and this site has walked me along that path through patient consistent quality across pieces.
KevinCef –
While exploring self care and wellness resources focused on healthy growth, I found a website that feels organized and uplifting for thoughtful browsing, and Dream Wellness online delivers a smooth browsing experience overall – Featured topics are displayed clearly, navigation is intuitive, and readers can focus on supportive wellness strategies without clutter.
Robertdreah –
While exploring various online marketplaces earlier today, I eventually stopped at simple luxury hub because the interface looked clean and the categories appeared easier to browse than many cluttered ecommerce platforms online currently – I really appreciated the modern layout and the pages felt polished and easy to navigate throughout.
Jamespox –
During an online exploration of self improvement content platforms, I came across daily inspiration ideas hub – The platform offers inspired thinking and helpful ideas for personal growth journey, making the browsing experience simple, structured, and enjoyable.
HowardAmall –
After exploring several online marketplaces and digital stores today, I eventually visited trusted twilight petal hub and noticed everything seems organized properly, with pages opening smoothly and content remaining easy to understand throughout the visit.
Chesternit –
After comparing several internet platforms and websites this afternoon, I spent some time on organized online destination, where browsing through the available information felt simple and comfortable thanks to the fast loading pages and clean presentation style.
Justinbloms –
https://sildenafilvip.shop/# Sildenafil Vip
HenryGem –
During an online exploration of gift inspiration websites, I discovered unique creative space – The website featured a variety of interesting ideas, and the browsing experience felt smooth and enjoyable, making it worth returning to again for future updates.
KendallViaro –
Looking forward to seeing what gets published next month, and a look at everymomentmatters extended that anticipation across the broader site, finding myself looking forward to a sites future content rather than just consuming its existing content is a stronger commitment level than I usually reach with new finds and this site triggered that.
Elmerfluby –
http://sildenafilvip.com/# Viagra without a doctor prescription Canada
MaxPub –
Honest take is that I will probably forget most of what I read online today but this post is one I will remember, and a stop at trendylifestylehub kept that same memorable quality going, certain writing leaves a residue in the mind in a way most content simply does not manage.
Benjic –
Worth pointing out that the post avoided the temptation to summarise everything at the end, and a look at thinkbigmovefast continued that confident closing approach, content that trusts readers to retain the substance without being reminded of it at the end is content that respects the reader and this site practices that respect.
Davidkek –
Honest assessment after reading this twice is that it holds up under careful attention, and a look at purechoiceoutlet extended that durability across more pages, content that survives a second read without revealing weak spots is rarer than the average reader probably realises and this site clearly cleared that bar.
JordanWexia –
Now thinking I want more sites built on this kind of editorial foundation, and a stop at bestchoicecollection extended that wish into a broader hope, sites built on substance and care rather than on metrics and growth are the kind of sites I want to see more of and this one is a small example worth supporting.
TrumanWen –
While checking different personal growth and motivation platforms online, I noticed Action Mindset Hub integrated into the content flow – I am actually taking action now, this site gave me the push that helped me finally stop hesitating and start doing the things I kept postponing for too long
ArronDiz –
Users looking for continuous idea flow and innovation support can visit idea flow platform which offers curated inspiration and structured thinking tools – it encourages creative exploration while helping individuals improve their ability to generate and organize ideas effectively.
DylanPonry –
Good quality through and through, no rough edges and no signs of being rushed, and a quick look at yourfashionoutlet kept the same polish going, the kind of site that respects its own brand by maintaining consistency across pages which is something I always appreciate as a reader looking for trustworthy information online today.
KellyJat –
During a casual browsing session for lifestyle and design-focused websites, I came across smart home style corner – The platform offered a clean interface and engaging content, making it easy to explore ideas while enjoying a smooth and visually pleasing browsing experience overall.
Chrisvoica –
buy cialis pill buy cialis pill п»їcialis generic
LorenKiz –
While exploring inspirational lifestyle and mindfulness websites focused on personal growth and reflection, I found a clean and meaningful platform that feels easy to navigate, and Every Moment Matters hub delivers a smooth browsing experience overall – The content encourages readers to appreciate daily experiences while presenting thoughtful ideas in a calm and organized way that feels welcoming and uplifting.
Danielthype –
During a casual search for learning development platforms, I discovered modern explore learning space – The platform offers educational content and motivation to learn, explore, and achieve, making browsing easy, structured, and enjoyable across the entire site.
WilliamWex –
During my review of online retail platforms, I came across a website that feels structured and fast, and Shore Frost commerce goods offers smooth navigation overall – Pages load quickly, content is well organized, and users can browse comfortably without confusion or clutter affecting usability.
ArthurMum –
Closed the post with a small satisfied sigh, and a stop at perfectbuyzone produced the same gentle exhale, content that ends well is content that respects the rhythm of reading and the writers here have clearly thought about how their pieces close rather than just trailing off when they run out of things to say.
PeterMef –
I spent part of my day browsing SEO-related websites before eventually stopping at easy ranking bridge hub where the structure looked simple and navigation felt smoother than several competing platforms online today – The website loaded without delays and appeared trustworthy and genuinely helpful for users during my visit.
RaymondSaime –
During my online browsing session this morning, I explored multiple websites before discovering quality urban emporium hub, and I really liked exploring it, as the website felt modern and browsing remained simple for visitors overall.
Ronaldted –
While searching for online fashion and style platforms, I discovered smart outfit space – The website offered stylish content and simple navigation, creating a smooth and enjoyable browsing experience across multiple categories.
Yorkgexus –
Felt like I was reading something written by someone who actually thinks about the topic rather than reciting it, and a look at creativegiftplace reinforced that impression, the difference between recited content and considered content is huge and this site clearly belongs to the latter category which I appreciate as a careful reader looking for substance.
IrvingPaf –
Learned something from this without having to dig through layers of fluff, and a stop at learnexploreachieve added a bit more context that helped tie things together for me, definitely a useful corner of the internet for anyone who wants real information without the usual marketing nonsense around it that often ruins similar pages.
Dannycic –
Working through this site has been a small antidote to the shallow content that fills most of my reading time, and a stop at modernideasnetwork extended that antidote function, sites that quietly improve the average quality of my reading by being themselves are sites worth supporting through return visits and recommendations consistently.
BurtonWed –
Picked up several practical tips that I plan to try out this week, and a look at findyourfocus added a few more I will be testing alongside, content with practical hooks that connect to my actual life is the kind that earns my repeat attention rather than the merely interesting that I forget within a day.
Justinbloms –
https://cialisvip.com/# Cialis Vip
Chandlerlix –
Cuts through the usual marketing fluff that dominates this topic online, and a stop at trendforlife kept the same clean approach going, this is the kind of writing that respects the reader’s time rather than wasting it on repetitive setups before finally getting to the point at hand which is what most sites do.
ShaneJah –
During a session of exploring fashion trend websites and lifestyle shopping platforms, I came across Trendy Style Vault Hub integrated into the content flow – Cool stuff everywhere, and my friends always ask where I shop since everything always looks fresh, stylish, and significantly more interesting than typical retail experiences online
Michaelallog –
During an online browsing session focused on casual shopping, I found daily fun product hub – The platform delivers a relaxed shopping experience with fun products and easy navigation online, making the experience smooth, simple, and enjoyable throughout.
Kennethtib –
During exploration of online shopping deal hubs, I found a website that feels practical and engaging for bargain hunters, and Dream savings network offers a smooth browsing experience overall – The interface is intuitive, promotions are highlighted effectively, and users can explore discounted products without unnecessary distractions.
Elmerfluby –
https://stromectolvip.online/# stromectol generic name
JamesSak –
After opening various internet resources and shopping websites this morning, I eventually found organized browsing portal, and the combination of structured product displays with informative descriptions made the overall experience very pleasant.
mostbet_wmpi –
бонус за первый депозит мостбет [url=www.mostbet78053.help]бонус за первый депозит мостбет[/url]
mostbet_gakr –
мостбет домени нав [url=https://www.mostbet62590.help]мостбет домени нав[/url]
melbet_dypt –
мелбет служба поддержки [url=http://melbet18095.help]мелбет служба поддержки[/url]
Jameswog –
During a late evening search for SEO platforms and marketing tools, I eventually came across trusted SEO store hub because the design looked neat and browsing felt more stable than several alternatives online currently – The website felt great overall, and accessing information and products was simple and comfortable throughout.
Chrisvoica –
Viagra online price Sildenafil Vip Generic Viagra for sale
Matthewsib –
I explored several internet stores and product websites this morning before discovering professional fern urban marketplace, and it was a helpful platform overall, with easy categories and comfortable product discovery throughout the experience.
Rogerref –
Cheap Cialis [url=http://cialisvip.com/#]Cialis 20mg price[/url] Cheap Cialis
WalterLef –
During a casual browsing session focused on online shopping trends, I came across hot finds hub – The website presented several interesting products in a clear and organized format, making it feel engaging and worth visiting again for future browsing sessions.
BrysonThero –
Strong recommendation from me, anyone curious about the topic should make time for this, and a look at findsomethingamazing only sharpens that recommendation further, the kind of resource that holds up against careful scrutiny rather than crumbling at the first critical question is rare and worth pointing other people toward when the topic comes up.
Donaldfug –
During an online exploration of success and motivation platforms, I came across creative motivation hub – The site had a strong positive atmosphere with inspiring information, making it stand out online and ensuring a smooth, enjoyable browsing experience throughout.
StephenNek –
Anyone aiming to improve imagination and analytical reasoning can explore visionary thinking desk which shares curated content focused on enhancing cognitive flexibility and idea generation skills – supporting users in developing stronger creative habits while encouraging continuous intellectual growth and improved problem solving approaches across various scenarios.
ShaneJah –
While browsing different online fashion discovery platforms and modern shopping inspiration sites focused on unique styles and trend collections, I came across Trendy Style Finder Hub naturally placed within the content flow – There is cool stuff everywhere here, and my friends always ask me where I shop because the selections always look unique, fresh, and different from typical stores
Robertkep –
While reviewing lifestyle focused shopping websites that emphasize positive experiences, I came across a platform that feels engaging and pleasant, and Happy Choice Market delivers a smooth browsing experience overall – The layout is structured, product listings are clear, and users can enjoy browsing items that feel rewarding and useful.
Georgecerma –
While reviewing different service websites, I came across a platform that feels clean and practical, and Web Service Boosters hub offers a smooth browsing experience overall – The design is simple, navigation is easy, and users can explore services without clutter or confusing visual elements.
Justinbloms –
http://sildenafilvip.com/# Sildenafil Vip
Robertrak –
I recently checked several informational websites before eventually reaching featured update hub where the interface looked organized and navigation felt smoother than many cluttered platforms online today – The updates were interesting and the design felt clean, visually balanced, and easy to browse during the visit.
Glennecona –
During a comparative review of several online marketplaces focusing on user experience and accessibility, I noticed AmberRidge product listings – that this platform maintains a clean interface; browsing is relatively simple, and product sections are clearly separated for better user understanding and engagement.
Elmerfluby –
https://cialisvip.com/# Cialis Vip
Michaeldroro –
While casually checking online marketplaces earlier today, I came across cleanly arranged lattice hub and found a good experience overall, with trustworthy information and smooth navigation across all sections.
Chrisvoica –
Viagra Tablet price Generic Viagra for sale Viagra online price
Williamhoile –
Learners who want to achieve consistent progress in studies can use knowledge skill hub which provides educational materials and motivational guidance – helping individuals strengthen their learning habits, stay committed to goals, and achieve success through structured practice and ongoing self improvement efforts.
Rodrick –
I like the helpful information you provide for your articles.
I’ll bookmark your blog and test again right here regularly.
I’m relatively certain I will be told a lot of new stuff proper right
here! Best of luck for the next!
Also visit my web page – hexable game online (Franziska)
ShaneJah –
While browsing digital fashion platforms and curated trend shopping pages, I noticed Style Vault Trend Hub embedded within the article structure – There is cool stuff everywhere here, and my friends always ask where I shop because the collection always feels unique, modern, and more stylish than regular online stores
CharlesFup –
During my review of educational growth platforms, I came across a website that feels structured and practical, and Future Ideas workshop offers smooth navigation overall – The interface is intuitive, pages load quickly, and users can explore inspiring concepts without unnecessary complexity or clutter.
Phillipbom –
While checking multiple online recommendation pages for something new and useful, I found wonder finds page</a positioned naturally inside an article section, and the browsing experience felt easy, modern, and consistently updated for anyone exploring different categories – Everything looked organized and pleasant, making navigation feel completely effortless.
Skylardrymn –
Found the writing surprisingly fresh for what is by now a well covered topic, and a stop at fashionforlife kept that freshness going across the related pages, original perspective on familiar ground is hard to come by and this site has clearly earned its place in the conversation rather than just rehashing old ideas.
MiguelDrike –
While exploring a variety of online stores and digital resources this morning, I came across useful online reference and appreciated the appealing design style along with the smooth browsing experience that felt easy and user friendly throughout.
Richardten –
While exploring online platforms focused on improving daily routines and organization, I found streamlined living hub – The website provided clear, practical information that felt easy to use and understand, making the browsing experience smooth and genuinely helpful for simplifying everyday tasks and decisions.
Justinbloms –
https://stromectolvip.com/# generic ivermectin for humans
Harryhoult –
I recently checked multiple logistics and parcel tracking websites before eventually landing on trusted delivery portal where the interface appeared structured and browsing felt smoother than several competing platforms online today – The site was helpful and easy to navigate, making it something I would definitely bookmark for later use.
TimothyPaype –
While analyzing various online stores for interface quality, I noticed Aurora Street shopping interface which offers a smooth browsing experience, and the layout feels balanced, allowing users to explore items easily while maintaining clarity and structure across different sections of the website overall.
Thomasscops –
People who enjoy slow paced browsing often look for platforms that make discovering new products feel easy and enjoyable Enjoy your shopping day site – delivering a calm and friendly browsing experience that encourages users to explore various items while maintaining a relaxed and pleasant shopping atmosphere online.
Darrensance –
While exploring different online shopping websites this morning, I spent time on valuable meadow goods marketplace, and the website design appeared appealing, with products clearly shown and pages loading fast and consistently.
LarryVaf –
While searching for online fashion inspiration platforms, I discovered modern look space – The website had a strong modern presentation and easy navigation structure, making browsing smooth, enjoyable, and visually pleasant across all style related sections.
KevinStarm –
During exploration of online bargain listing websites, I found a platform that feels clean and efficient for discovering discounts, and Online Discount marketplace offers a smooth browsing experience overall – The interface is clear, pages load quickly, and shoppers can explore promotions without confusion or complexity.
Hermannex –
While reviewing various SEO support tools and dashboards, I found a site that feels modern and efficient in its execution, and WebRank insights tool delivers a smooth browsing experience overall – The system is responsive, and the interface makes it easy to interpret ranking data clearly and quickly.
GeorgeLit –
During a search for stylish apparel collections that merge craftsmanship from different parts of the world, I came across refined style marketplace guide – the collection emphasizes Japanese denim heritage and Italian leather elegance, offering a balanced global curation that feels both modern and rooted in timeless fashion traditions overall experience.
Claytonthura –
However selective I am about new bookmarks this one made it past my filter, and a look at learnsomethingeveryday confirmed the bookmark was worth the slot, the precious slots in my permanent bookmark folder are difficult to earn and this site earned one without making me think twice about whether the slot was justified by the quality.
JustinNib –
While checking multiple fashion discovery platforms and trend websites, I discovered fashion trend corner included in a curated section, and the stylish collection was nicely displayed while navigation worked smoothly across different categories and pages.
Coreygaick –
While browsing several modern ecommerce and catalog-style websites earlier today, I eventually spent time exploring organized product shelf hub because the layout felt clean and navigation was smooth compared to many cluttered platforms online currently – The website felt responsive and well organized, and I genuinely enjoyed looking through different pages and categories.
BryanRurne –
During an evening search for interesting online shopping resources and curated browsing collections, I found shopping inspiration page – The website delivered smooth category navigation, an attractive overall design, and enough organized content to create a browsing experience that felt both relaxing and visually satisfying throughout the visit.
Richardmeack –
While testing several creative commerce websites, I experienced a generally fluid browsing journey, and Azure Grove crafts directory offers dependable page responsiveness with an organized layout, making it easier for users to explore items without encountering slowdowns or confusing structural elements during navigation sessions.
KendallRor –
While reviewing shopping discount platforms, I came across a site that feels clean and user friendly, and Amazing Corner deals hub delivers smooth navigation overall – The design is minimal, offers are easy to understand, and users can explore discounts without clutter or confusing visual elements affecting usability.
CraigDaf –
While searching for fashion inspiration and styling guides online, I discovered elegant style finder – The website provided engaging content with a polished interface, making browsing smooth, visually appealing, and easy to explore across multiple sections.
Justinbloms –
http://stromectolvip.com/# stromectol price in india
BradleyNeult –
While casually browsing digital shopping platforms this afternoon, I came across organized petal urban site and enjoyed browsing here, with everything appearing well maintained and content reading naturally throughout.
Rogerref –
generic sildenafil [url=https://sildenafilvip.com/#]Sildenafil Vip[/url] Viagra without a doctor prescription Canada
MatthewPeeld –
Sildenafil 100mg price Sildenafil Vip Viagra without a doctor prescription Canada
Ronaldnub –
I spent part of the afternoon comparing several internet stores and eventually visited recommended web resource, and I immediately noticed how easy the navigation felt while the content seemed actively updated and professionally organized.
AndrewBleds –
Many new runners find motivation in structured plans that make each workout feel purposeful and bring them closer to completing a real race Momentum Fitness Hub I ran my first 5k after following their training plan and I still can’t believe I finished it – Ran my first 5k after following their training plan, wow just wow
Ginorak –
Now thinking the topic is more interesting than I had given it credit for, and a stop at exploreinnovativeideas continued that elevated interest, content that revives my curiosity about subjects I had set aside is doing genuine work in the structure of my interests and this site is providing that revivifying effect today actually.
Terrysaics –
While casually exploring online information platforms earlier today, I found myself reviewing simple info corner hub because the interface looked neat and browsing felt more comfortable than many competing websites online currently – The content was nice overall and everything seemed updated and carefully arranged for visitors browsing the platform.
JeanJek –
Now realising this site has been quietly doing good work for longer than I knew, and a look at makesomethingnew suggested an archive worth exploring, sites with deep archives of consistent quality represent a different kind of resource than sites with viral hits and this one looks like the durable kind based on what I see.
Gregorythymn –
During comparison of logistics information platforms, I noticed a website that feels modern and well structured, and ParcelWise logistics hub provides smooth browsing overall – The interface is intuitive, pages respond quickly, and users can access service information without unnecessary complexity or distracting design elements.
Justinbub –
As part of a longer search for reliable websites sharing updated information, I came across recommended information spot included in a curated list, and the platform maintained a simple structure while the latest content additions looked authentic, carefully managed, and consistently refreshed for active visitors online.
Thomasrog –
During exploration of artistic innovation communities, I found a platform that feels simple and motivating for creative professionals, and Design Concept online hub offers a smooth browsing experience overall – Articles are organized neatly, browsing feels natural, and users can focus on fresh creative perspectives without clutter.
Chrisvoica –
sildenafil 50 mg price Cheap generic Viagra online Cheap generic Viagra online
Elmerfluby –
https://stromectolvip.online/# ivermectin 400 mg brands
Williekab –
While searching for online shopping deal platforms, I discovered modern smart deals hub – The platform featured interesting content with smooth navigation, making browsing enjoyable, easy, and worth revisiting regularly for new offers and ideas.
Allended –
During exploration of online shop directories, I viewed Blossom Bay shop directory which keeps everything organized with a simple navigation structure and well spaced elements – The browsing experience feels easy and well structured.
GerardoDUM –
I spent part of today exploring online stores and digital platforms before finding easy navigation pine urban site, and I found a nice browsing experience overall, with organized categories and smooth, reliable functionality throughout the entire visit.
HubertDok –
Browsing new collections late at night became addictive because every refresh showed something fresh and exciting from trending streetwear releases Urban Fit Finder I ended up grabbing a pair I had wanted for weeks and the fit and comfort were genuinely better than expected
TerranceKal –
Picked this site to mention to a colleague who would benefit, and a look at uniquevaluezone added more material I will pass along, recommending sites to colleagues is a higher bar than recommending to friends because the professional context demands more careful curation and this site cleared the professional bar without me having to think.
Stevenmef –
While searching for collaborative learning websites and online knowledge platforms, I came across smart education hub – The layout was clean and easy to understand, offering a comfortable browsing experience where users could quickly access valuable information and explore different categories with ease.
StanleyJably –
ivermectin 3 mg: stromectol Vip – stromectol 6 mg tablet
LeonardSkyMn –
During an online search for shipment tracking tools and courier updates, I explored easy parcel navigator since the layout felt intuitive and neat – The browsing experience felt pleasant today, and the website design looked modern, welcoming, and naturally inviting for users tracking deliveries efficiently.
Justinbloms –
https://cialisvip.com/# Cialis Vip
Billylog –
While reviewing online promotions websites, I came across a platform that feels engaging and simple to navigate for shoppers, and Offer Hunter space delivers a smooth browsing experience overall – The interface is clean, promotions are organized clearly, and users can explore savings opportunities without distractions or confusion.
Brucegaugh –
I spent some time reviewing online collections and digital storefronts today before reaching reliable online showcase, where the website structure and category arrangement made finding products quick and straightforward.
RonaldGeova –
A satisfying piece in the way that good meals are satisfying rather than just filling, and a look at thebestvalue extended that satisfaction, the metaphor between content and meals is one I find useful and this site reads as a satisfying meal rather than the empty calories that most content provides for casual readers.
AnthonyDoG –
People who care about sustainability often start their journey by focusing on reducing plastic dependence in daily life Eco Future Hub I began recycling more carefully and cutting down plastic usage, and it feels like a meaningful improvement – Started recycling more and using less plastic, small steps matter
StevenTum –
Earlier this afternoon I checked different online communities and content-sharing websites before finding well designed resource page, where the responsive pages and carefully balanced visual structure created a seamless experience while moving through multiple categories and highlighted sections.
RobertGak –
While exploring various ecommerce websites for general usability and design quality, I came across a clean and responsive platform, and Blossom Haven product hub provides a neat browsing flow – The site feels modern in design with simple navigation patterns that allow users to explore categories comfortably without distractions or unnecessary complexity in layout.
Stanacalm –
Now adding the writer to a small mental list of voices I want to follow, and a look at believeinyourideas reinforced that follow intention, the few writers whose work I actively track are writers who have demonstrated sustained quality and this writer has clearly demonstrated that sustained quality across the pieces I have sampled here today.
EldonRouri –
I spent time browsing various online catalogs today before discovering reliable urban ridge site, and I appreciated the simple navigation, with accessible products and stable performance throughout the visit.
BrianHes –
While comparing several informational and value-based platforms, I noticed a site that feels structured and easy to use, and UniqueCorner value hub provides a smooth browsing experience overall – The interface is simple, content is well arranged, and users can browse comfortably without unnecessary distractions or complex design elements.
mostbet_hlEi –
mostbet ocolire blocare Moldova [url=http://mostbet41079.help/]mostbet ocolire blocare Moldova[/url]
Danieldab –
http://stromectolvip.com/# ivermectin 3
ivermectin cream cost
WilliamBeist –
During my review of contemporary streetwear websites, I came across a platform that feels engaging and easy to use, and Street Style Outlet offers a smooth browsing experience overall – The layout is modern, categories are well organized, and users can browse trendy urban outfits designed for everyday modern lifestyles.
Chrisvoica –
п»їcialis generic Cialis Vip buy cialis pill
Waynemit –
While reviewing online browsing platforms and recommendation pages with organized categories, I found modern explore center – The layout looked thoughtfully designed, the sections were simple to move through, and the platform provided enough useful information to keep the browsing session engaging throughout.
Elmerfluby –
http://sildenafilvip.com/# Sildenafil Vip
FreddieNeage –
Compared to the usual results for this kind of search this site stands well above the average, and a quick visit to urbanfashioncorner kept the standard high, you can tell within seconds whether a site is going to waste your time or actually deliver and this one clearly delivers without any false starts.
PedroFaige –
While analyzing various handmade product websites for usability, I came across a platform that feels easy to navigate and visually balanced, and BrightForge craft collection offers a structured browsing experience overall – Everything is arranged logically, making it simple for users to find products while enjoying a smooth and clutter-free interface.
Juliouncew –
After opening multiple online shopping websites today, I eventually reached recommended velvet cove portal, and the website felt really pleasant, with regularly updated information and enjoyable browsing throughout the session.
Michaelicola –
During a relaxed session browsing online fashion and lifestyle shops, I came across fashion style corner placed in a list of recommended links, and the browsing experience felt smooth as product pages were clean, well organized, and enjoyable to explore.
Justinbloms –
https://stromectolvip.com/# stromectol over the counter
melbet_axEa –
melbet slots argent réel [url=www.melbet62913.help]www.melbet62913.help[/url]
mostbet_wsSl –
mostbet ekspress kupon necə edilir [url=https://mostbet01859.help/]https://mostbet01859.help/[/url]
JamesWef –
During comparison of personal growth and productivity websites, I noticed a website that feels modern and efficient for self improvement readers, and Focused Living center offers a smooth browsing experience overall – The layout is straightforward, featured guidance is easy to follow, and visitors can improve daily productivity without distractions.
mostbet_upSl –
mostbet pul çıxarma olmur [url=www.mostbet01859.help]www.mostbet01859.help[/url]
Earnestbew –
During my search across several online stores this afternoon, I eventually visited high quality web platform, where the polished interface and smooth page loading helped create an enjoyable browsing experience for all visitors.
mostbet_rdsa –
mostbet plati [url=http://mostbet18305.help/]mostbet plati[/url]
Rogerref –
buy viagra here [url=http://sildenafilvip.com/#]Buy Viagra online cheap[/url] generic sildenafil
seogrove –
Bookmark added with a small note about why, and a look at seogrove prompted another bookmark with another note, the bookmarks I annotate are the ones I expect to return to deliberately rather than stumble into and this site is generating annotated bookmarks at a higher rate than my usual content sources by some margin.
mostbet_cnPl –
mostbet live baccarat [url=mostbet87124.help]mostbet87124.help[/url]
mostbet_iaEi –
mostbet acces oglinda [url=mostbet41079.help]mostbet41079.help[/url]
MelvinPaype –
Well structured and easy to read, that combination is rarer than people think, and a stop at urbanstylemarket confirmed the same standard runs across the rest of the site, definitely the kind of place I will be coming back to when this topic comes up in conversation later again over the weeks ahead.
aviator_myKn –
aviator download free [url=http://aviator50638.help]aviator download free[/url]
RogerElumb –
During an online search for exploration-focused and travel-related websites, I discovered global insight hub – The platform featured organized content and a modern layout, making browsing easy while everything felt updated, structured, and thoughtfully designed for users exploring different categories.
Ralphcib –
During comparison of online retail experiences, I noticed a platform with strong optimization and fast response times, and CloudForge craft marketplace offers smooth performance overall – The site reacts quickly to navigation, allowing users to browse comfortably and efficiently without delays or interruptions in page loading.
Carlostaf –
During my search across several digital marketplaces this afternoon, I eventually visited high quality field velvet hub, and it was a great platform overall, where pages loaded quickly and categories were organized very professionally.
mostbet_pcSl –
mostbet depozit bonusu necə alınır [url=mostbet01859.help]mostbet depozit bonusu necə alınır[/url]
RichardBurry –
While exploring productivity and self improvement websites focused on helping people stay organized and mentally sharp, I found a clean and practical platform that feels easy to navigate, and Find Your Focus hub delivers a smooth browsing experience overall – The content encourages stronger concentration habits while presenting useful productivity ideas in a calm and easy to understand format.
mostbet_nxsa –
mostbet suport pentru probleme acces [url=https://mostbet18305.help/]https://mostbet18305.help/[/url]
Elmerfluby –
https://sildenafilvip.com/# Cheap Viagra 100mg
seoharbor –
Felt the post handled a sensitive angle of the topic with appropriate care, and a look at seoharbor extended that careful handling across related material, sites that can navigate delicate territory without causing damage are rare and require a level of judgement that comes from experience rather than from following any clear playbook.
Justinbloms –
http://cialisvip.com/# Cialis Vip
aviator_akKn –
aviator promo [url=https://aviator50638.help]https://aviator50638.help[/url]
mostbet_kwSl –
mostbet 18+ qeydiyyat [url=https://mostbet01859.help/]https://mostbet01859.help/[/url]
Gordontom –
While testing various online retail platforms, I found a simple and structured browsing system, and CloudMeadow collective shop hub delivers smooth navigation overall – The content is clearly arranged, allowing users to browse and read product details easily without distractions or complicated interface design.
Williamtaigo –
While reviewing ecommerce stores, I found a platform that feels modern and user friendly, and Trend Shop World store offers a smooth browsing experience overall – The interface is well organized, products are easy to find, and users can explore without unnecessary complexity or distractions affecting usability.
DarylNuh –
Probably the kind of site that should be more widely read than it appears to be, and a look at trendsettersparadise reinforced that quiet wish, the gap between a sites quality and its apparent reach is sometimes large and that gap exists for this site in a way that makes me want to mention it more.
aviator_keKn –
aviator game official site [url=http://aviator50638.help/]http://aviator50638.help/[/url]
Tyronenak –
After opening multiple online trading platforms and digital marketplaces today, I eventually reached recommended trading showcase, where the website performance stayed stable and the information appeared detailed enough to make browsing straightforward and easy.
aviator_dkKn –
aviator deposit with airtel money Malawi [url=www.aviator50638.help]www.aviator50638.help[/url]
Chrisvoica –
ivermectin eye drops stromectol Vip stromectol drug
DanielSpugs –
After navigating through several online marketplaces today, I eventually visited professional oak whisper listing, and I noticed the website felt reliable, with browsing staying smooth and descriptions appearing clear and easy to understand.
Elmerfluby –
https://cialisvip.com/# Tadalafil Tablet
SamuelTwene –
During exploration of different online shopping platforms, I came across a site with a simple and elegant layout, and Petal Collective cloud store delivers a visually clean interface overall – Everything is arranged in a structured manner, allowing users to browse products easily while maintaining clear readability and smooth navigation across all pages.
LeonBew –
Quality you can feel from the first paragraph, the writer clearly knows the topic and how to share it, and a quick look at findyourinspiration confirmed the same depth runs throughout the rest of the site as well which is rare and worth pointing out when it happens online for any reader passing through.
Justinbloms –
http://stromectolvip.com/# stromectol 0.5 mg
BryonGef –
During my exploration of learning and inspiration sites, I found a website that feels modern and clear, and MindExpand exploration hub delivers smooth browsing overall – Content is well structured, pages load quickly, and users can enjoy reading without unnecessary distractions or cluttered design.
Chestershoni –
bütün oyun siteleri pin up
melbet_pnEa –
melbet site en français [url=http://melbet62913.help/]http://melbet62913.help/[/url]
MichaelPsymn –
After browsing through several shopping platforms today, I eventually discovered structured online shop, where the helpful browsing experience made it easy to view clearly displayed products and descriptions that read naturally and smoothly.
DavidFLING –
While reviewing different online shopping pages this afternoon, I visited organized grove mystic listing, and I found a helpful experience overall, with well arranged products and comfortable navigation across the browsing flow.
mostbet_kvPl –
mostbet kurzové sázení Česko [url=https://mostbet87124.help]mostbet kurzové sázení Česko[/url]
WilliamSOOSY –
During my review of online shopping platforms, I found a site that prioritizes fast page loading, and Petal Cloud marketplace network delivers a stable experience overall – Pages open quickly, and the browsing flow feels smooth, ensuring users can explore products without delays or performance interruptions affecting usability.
Chrisvoica –
ivermectin 50 stromectol Vip ivermectin 10 mg
DreDug –
A piece that was confident enough to leave some questions open rather than forcing closure, and a look at everydaychoicehub continued that intellectual honesty, content that admits the limits of its scope is more trustworthy than content that pretends to total understanding and this site has the right calibration on certainty consistently.
mostbet_hrPl –
mostbet blackjack [url=https://mostbet87124.help]https://mostbet87124.help[/url]
melbet_ewEa –
melbet bonus en fcfa [url=http://melbet62913.help]http://melbet62913.help[/url]
Justinbloms –
https://sildenafilvip.com/# Sildenafil Vip
melbet_mlEa –
melbet retrait maximum [url=www.melbet62913.help]melbet retrait maximum[/url]
Charleslix –
During comparison of inspiration websites, I noticed a platform that feels modern and clear, and NextYourAdventure space provides smooth browsing overall – The interface is simple, content is engaging, and users can explore without confusion or clutter affecting usability.
Carlosplogy –
During comparison of online stores, I found a platform that emphasizes simplicity and clear navigation, and Petal Cloud shopping store delivers smooth browsing overall – The interface is structured and easy to follow, making it user friendly and comfortable for browsing products without confusion.
mostbet_jasa –
mostbet timp de răspuns suport [url=mostbet18305.help]mostbet timp de răspuns suport[/url]
Ramonwes –
I spent time exploring several online stores today before landing on reliable floral showcase, and I enjoyed the experience since the professional organization and perfectly working navigation made everything easy and smooth.
mostbet_xjEi –
mostbet Grigoriopol [url=http://mostbet41079.help]http://mostbet41079.help[/url]
SilasCip –
The way the post stayed on topic throughout without going on tangents was really refreshing, and a look at discovernewhorizons kept that focused approach going, discipline like this in writing is rare and worth recognising because most writers cannot resist wandering off into related subjects that dilute their main point and confuse readers along the way.
mostbet_uvEi –
mostbet conectare [url=https://mostbet41079.help]mostbet conectare[/url]
Chrisvoica –
Buy Tadalafil 10mg Cialis Vip п»їcialis generic
DennisHeemo –
During a casual online search for product browsing and shopping discovery websites, I came across modern product guide – The interface was clean and easy to understand, and the structured content helped create a naturally engaging browsing experience that felt simple and enjoyable overall.
Justinbloms –
http://stromectolvip.com/# stromectol medication
mostbet_mkPl –
mostbet live sázky fotbal [url=https://mostbet87124.help]https://mostbet87124.help[/url]
JosephIllit –
While exploring digital shopping platforms, I came across a well designed interface that feels user friendly, and CloudRidge goods shop hub delivers a pleasant browsing experience overall – The structure is clear and organized, making it easy for users to quickly find products without confusion or unnecessary complexity.
RobertNum –
While exploring uplifting online platforms, I found a website with a clean and welcoming design, and BrightBeginnings inspiration hub delivers a smooth browsing experience overall – Everything is structured neatly, making it easy for users to navigate and explore content without confusion or unnecessary visual complexity.
MarvinUnult –
Generally I find the content on similar topics frustrating in specific ways and this post avoided all of them, and a look at findbetteropportunities continued that frustration free experience, content that sidesteps the standard failure modes of its genre is content with editorial awareness and this site has clearly studied what fails elsewhere consistently.
Chrisvoica –
ivermectin 50 stromectol Vip ivermectin purchase
seohive –
Liked the way the post balanced confidence and humility, and a stop at seohive maintained the same balance, knowing when to assert and when to acknowledge uncertainty is a sign of mature thinking and the writers here have clearly developed that calibration through what I assume is years of careful work on their craft.
Carlosemece –
Earlier today I explored various online stores before landing on featured shopping site, and I noticed how the clean website design and organized categories helped browsing stay simple and smooth for everyone visiting.
FrankTieby –
While analyzing ecommerce websites, I came across a platform that emphasizes readability and structure, and Cloud Spire product marketplace delivers stable performance overall – Everything is arranged neatly, making it easy for users to browse and read content without distractions or clutter affecting the experience.
Justinbloms –
https://sildenafilvip.shop/# Cheap generic Viagra
Donaldalobe –
While reviewing online deal collections and recommendation websites for useful shopping information, I discovered daily outlet collection – The categories were presented clearly, the browsing process remained efficient, and the overall structure helped visitors explore available content without unnecessary distractions during the experience.
seolift –
Really clear writing, the kind that makes you want to share the link with someone who has been asking about the topic, and a quick browse through seolift only made me more sure of that, the information here stays useful long after the first read is done which says a lot.
MatthewGoolo –
Thanks for treating the topic with the seriousness it deserves without becoming pompous about it, and a stop at thefashionedit continued that balanced treatment, the gap between earnest and self serious is huge and writers who can stay on the right side of it earn my respect when I find them online today.
mostbet_elsa –
mostbet meciuri live [url=http://mostbet18305.help/]mostbet meciuri live[/url]
Rogerref –
ivermectin cost [url=http://stromectolvip.com/#]stromectol tablets[/url] ivermectin human
Chrisvoica –
Cialis without a doctor prescription Cialis Vip cheapest cialis
JamesApota –
While exploring digital community websites, I found a platform that feels well organized and accessible, and Connect Share Grow portal delivers a smooth browsing experience overall – Content is structured neatly, pages load quickly, and users can access information easily without unnecessary distractions.
Larryknone –
While comparing several ecommerce stores, I noticed a platform with strong organization and fast loading performance, and FrostGoods harvest store offers a stable browsing experience overall – The interface is clean and structured, making it easy for users to move through categories while enjoying quick page response and visually organized content throughout the site.
Justinbloms –
https://sildenafilvip.shop/# Sildenafil Vip
seoloom –
Reading this triggered a small but real correction in something I had assumed, and a stop at seoloom extended that corrective effect, content that updates my beliefs through evidence rather than rhetoric is content with intellectual integrity and this site has earned that label consistently across the pieces I have read so far today.
JulioNut –
While spending time online reviewing different shopping resources and recommendation hubs with active content updates, I discovered daily promotion access – The website navigation was smooth, the content arrangement made browsing easier than expected, and the featured sections included enough variety to create a pleasant and naturally flowing online experience overall.
ByronFak –
While casually browsing different online platforms this afternoon, I came across organized web collective and found the experience good overall, as the information looked trustworthy and pages loaded smoothly without any noticeable delay issues.
Iangat –
Polished and informative without feeling overproduced, that is the sweet spot, and a look at everydayinnovation hit it again, you can tell when a site has been built with care versus thrown together for the sake of having something to put online and this is clearly the former approach taken by the team.
Chrisvoica –
where to buy stromectol ivermectin 3mg stromectol tab 3mg
seomagnet –
Now thinking I want more sites built on this kind of editorial foundation, and a stop at seomagnet extended that wish into a broader hope, sites built on substance and care rather than on metrics and growth are the kind of sites I want to see more of and this one is a small example worth supporting.
Justinbloms –
http://cialisvip.com/# Cialis Vip
Davidutilm –
During my exploration of productivity motivation sites, I found a website that feels structured and inspiring, and MoveBig ThinkFast hub delivers smooth navigation overall – Content is clearly presented, pages are simple, and users can focus on ideas without distraction or visual clutter.
CraigBex –
Even just sampling a few posts the consistency is what stands out, and a look at trendandfashionhub confirmed the broader pattern, sites where every piece I sample lives up to the standard set by the others are sites with serious quality control and this one has clearly invested in whatever editorial process produces that consistency reliably.
Davidfraxy –
During a search for motivational education platforms and self improvement tools, I discovered smart study resource – The website provided clear guidance and helpful sections that made it easy to find useful content while maintaining a smooth and engaging browsing experience throughout.
seometric –
Walked away with a clearer head than I had before reading this, and a quick visit to seometric only sharpened that, the writing has a way of cutting through the noise that surrounds most topics online which is something I will definitely remember the next time I am searching for an answer to anything.
Justinroula –
A piece that brought a sense of order to a topic I had been finding chaotic, and a look at believeandcreate continued that organising effect, content that imposes useful structure on messy subjects is doing genuine intellectual work and this site is providing that organisational function across multiple posts I have read recently here.
Anthonyrhymn –
I explored various internet marketplaces and digital catalogs this morning before discovering professional woven hub, and I found it really interesting overall, with browsing staying comfortable and everything appearing carefully maintained throughout the experience.
Chrisvoica –
Cialis 20mg price in USA Cialis Vip Cialis over the counter
Justinbloms –
https://stromectolvip.online/# stromectol 3 mg
Vaughnseage –
Honest reaction is that I want to send this to a friend who would benefit from it, and a look at yourstylezone added more material I will pass along too, the impulse to share is the strongest signal I have for content quality and this site is generating that impulse cleanly across multiple posts.
Alethea –
I am really happy to glance at this website posts which includes plenty of useful facts, thanks
for providing these statistics.
My website – sex power booster
seomotion –
Now feeling confident enough in this site to use it as a reference point for evaluating others on the same topic, and a look at seomotion continued the comparison friendly quality, sites that serve as quality benchmarks for their topic are precious and this one has clearly become a benchmark for me on this particular subject area.
Thomaswaw –
While exploring ecommerce discount platforms, I found a website that feels structured and easy to navigate, and FreshOutlet savings hub delivers a smooth browsing experience overall – The interface is minimal, products are well organized, and users can browse value offerings comfortably without clutter or distractions.
Claytonthura –
Strong recommendation, anyone interested in this topic owes themselves a visit, and a stop at learnsomethingeveryday extends that recommendation across more of the site, this is the kind of resource that makes me more optimistic about the state of the open web than I usually am these days actually for once which is genuinely refreshing.
Tadmom –
A piece that handled the topic with appropriate weight without becoming portentous, and a look at trendforlife continued that calibrated seriousness, content that takes itself seriously without becoming pompous is something this site has clearly figured out and the balance shows up in every piece I have read across multiple sessions now.
seomotive –
Now noticing how rare it is to find a site that does not feel rushed, and a look at seomotive extended that calm pace, content produced without time pressure has a different quality than content shipped to meet a deadline and this site reads as written without urgency which produces a different and better experience for readers.
Chrisvoica –
ivermectin tablets order stromectol pill stromectol online pharmacy
Rogerref –
sildenafil 50 mg price [url=http://sildenafilvip.com/#]Sildenafil Vip[/url] buy Viagra over the counter
Justinbloms –
http://cialisvip.com/# Cialis 20mg price
Scottset –
I explored several internet shopping platforms this morning before discovering professional online directory, and I appreciated the simple navigation along with accessible products and consistent reliable performance across the entire website.
seoorbit –
Ended up here on a wandering afternoon and was glad I stayed for the read, and a stop at seoorbit extended the wandering into a proper exploration of the site, the kind of place that rewards aimless clicking with something genuinely interesting rather than the shallow content that mostly populates the modern open web.
AshtonTinty –
A piece that respected the reader by not over explaining the obvious, and a look at startfreshjourney continued that calibrated approach, finding the right level of explanation is one of the harder editorial calls and this site has clearly thought carefully about what readers will already know versus what they need help with consistently.
mostbet_kmmi –
mostbet depozit [url=https://www.mostbet48932.help]mostbet depozit[/url]
MichaelJew –
While reviewing online clothing platforms, I came across a site that feels stylish and well organized, and Global Fashion Finds shop offers a smooth browsing experience overall – The interface is simple yet attractive, making it easy for users to browse fashion products without clutter or complexity.
cloudridgegoods –
Just wanted to drop a quick note saying this was a useful read on a topic I have been circling, no fluff, and a stop at cloudridgegoods added a few extra points that fit the same simple style which makes the whole site feel coherent rather than thrown together by many different writers with different goals.
Justinbloms –
http://stromectolvip.com/# ivermectin lotion for lice
Chrisvoica –
Buy Tadalafil 20mg Buy Cialis online Buy Tadalafil 10mg
melbet_uioi –
melbet crash как играть [url=www.melbet70382.help]melbet crash как играть[/url]
seoripple –
Looking at the surface design and the substance together this site has both right, and a look at seoripple reinforced that integrated quality, sites where presentation and content reinforce each other rather than fighting are sites with full editorial coherence and this one has clearly invested in both layers in a balanced way.
EganBuili –
Top tier post, the kind that makes you want to share the link with friends working in the same area, and a stop at shopandsaveonline only made me more confident in doing that, this site is one of the better resources I have seen on the topic recently across both new and older posts.
mostbet_ehMi –
mostbet pozwól na instalację apk [url=https://mostbet90617.help/]mostbet pozwól na instalację apk[/url]
melbet_daoi –
melbet игры на деньги [url=melbet70382.help]melbet игры на деньги[/url]
WilliamLiz –
While reviewing different online shopping pages this afternoon, I visited organized valley goods store, and I liked the nice browsing experience, where the modern layout made information easy to understand and follow throughout the visit.
cloudridgegoods –
Took the time to read the comments on this post too and they were also worth reading, and a stop at cloudridgegoods suggested the community quality matches the content quality, when the conversation around a piece is as good as the piece itself you know you have found a real corner of the internet.
seoscope –
Started reading and ended an hour later without realising the time had passed, and a look at seoscope produced the same time dilation effect, when content makes time feel different the writer has achieved something well beyond the average and this site is producing that experience for me reliably across multiple readings.
Justinbloms –
http://stromectolvip.com/# ivermectin cost canada
Chrisvoica –
Generic Tadalafil 20mg price Cialis over the counter Buy Tadalafil 10mg
Cameronacank –
Now considering writing a longer note about the post somewhere, and a look at yourfashionoutlet added more material for that note, content that prompts me to write rather than just consume is content with generative energy and this site is producing that generative effect for me at a higher rate than most sources.
CarlosVeiva –
During my review of inspirational lifestyle sites, I came across a website that feels engaging and clean, and AdventureNext inspiration path offers smooth navigation overall – Pages are well structured, content is motivating, and users can explore without clutter or confusing interface elements affecting usability.
seospark –
Reading this gave me a small jolt of recognition for an experience I thought was just mine, and a stop at seospark produced more such jolts, content that universalises private experiences without flattening them is doing genuinely useful work and this site is providing that recognition function for me reliably across topics I read.
melbet_ihSl –
мелбет поддержка [url=https://www.melbet35702.help]https://www.melbet35702.help[/url]
mostbet_eiMi –
mostbet sign up [url=https://mostbet90617.help]mostbet sign up[/url]
cloudspiregoods –
Bookmark added with a small mental note that this is a site to keep, and a look at cloudspiregoods reinforced the keep status, the verb keep rather than visit captures something about how I think about this kind of site and it is a higher tier of relationship than I have with most places online today.
Billyfub –
A piece that handled multiple complications without becoming confused, and a look at creativechoicehub continued that organisational clarity, holding multiple threads in a single piece without losing any of them is a sign of skilled writing and this site has clearly developed the editorial discipline to manage complexity without sacrificing readability throughout.
Justinbloms –
https://sildenafilvip.shop/# best price for viagra 100mg
mostbet_qeea –
mostbet crash [url=http://mostbet09486.help]http://mostbet09486.help[/url]
Chrisvoica –
Generic Cialis price Cialis 20mg price in USA Cialis 20mg price
RobertBakly –
After exploring several online marketplaces and digital stores today, I eventually visited trusted harbor shop and found everything seemed well organized, with browsing remaining smooth and content that looked genuinely helpful throughout the experience.
Rogerref –
п»їcialis generic [url=https://cialisvip.com/#]Generic Tadalafil 20mg price[/url] Cialis over the counter
DewayneGep –
During my exploration of online trend update platforms, I came across a site that feels engaging and easy to navigate, and Trend Daily spot hub delivers smooth browsing overall – The website updates content regularly, and everything is organized clearly so users can quickly discover new and relevant trending information.
Gilbertowemi –
Thanks for the breakdown, it gave me a clearer picture of something I had been confused about for a while now, and a stop at simplefashionstore closed the remaining gaps in my understanding nicely, no need to hunt around twenty other articles to put the pieces together which is a real time saver.
frostharvestgoods –
This stands out compared to similar posts I have read recently, less noise and more substance, and a look at frostharvestgoods kept that gap going, you can really feel the difference between content made by someone who cares versus content made to fill a publishing schedule for an algorithm trying to keep growing somehow.
Justinbloms –
https://sildenafilvip.shop/# generic sildenafil
Chrisvoica –
stromectol tab 3mg ivermectin pills ivermectin 3
seosprout –
Now adding this site to a small mental group of recommendations I keep ready for specific kinds of inquiries, and a stop at seosprout extended the recommendation readiness, content that I can confidently point friends and colleagues toward in specific contexts is content with real social utility and this site has that utility clearly.
RoccoJeD –
Reading this confirmed that my time researching the topic in other places had not been wasted, and a stop at purechoicehub extended the confirmation, when independent sources agree that is a useful signal and this site is one of the more reliable sources I have found for cross checking what I read elsewhere on similar subjects.
melbet_vqoi –
melbet купон ставок [url=https://www.melbet70382.help]https://www.melbet70382.help[/url]
seostreet –
Polished and informative without feeling overproduced, that is the sweet spot, and a look at seostreet hit it again, you can tell when a site has been built with care versus thrown together for the sake of having something to put online and this is clearly the former approach taken by the team.
frostlaneemporium –
Probably the best thing I have read on this topic in the past month, and a stop at frostlaneemporium extended that ranking, the casual ranking of recent reading is informal but real and this site has been winning those rankings for me on this topic specifically over the last several weeks of regular reading sessions.
Justinbloms –
https://sildenafilvip.com/# Sildenafil Citrate Tablets 100mg
melbet_qqSl –
melbet экспресс киргизия [url=www.melbet35702.help]melbet экспресс киргизия[/url]
mostbet_wiMi –
mostbet bonus za przegraną [url=http://mostbet90617.help]mostbet bonus za przegraną[/url]
Chrisvoica –
buy Viagra online Sildenafil Vip best price for viagra 100mg
melbet_mnSl –
melbet проверка аккаунта [url=https://melbet35702.help/]melbet проверка аккаунта[/url]
LeviOrede –
Adding to the bookmarks now before I forget, that is how good this is, and a look at dreambuildachieve confirmed the rest of the site is worth saving too, this is one of those rare finds that justifies the time spent searching the web for once which is a relief in the current environment.
seotactic –
Found this through a search that was generic enough I did not expect quality results, and a look at seotactic continued the surprisingly good experience, search engines occasionally still surface excellent independent content if you scroll past the obvious paid and high authority results which is reassuring to remember sometimes.
YorkCip –
Now noticing how rare it is to find a site that does not feel rushed, and a look at besttrendmarket extended that calm pace, content produced without time pressure has a different quality than content shipped to meet a deadline and this site reads as written without urgency which produces a different and better experience for readers.
frostmeadowcollective –
Picked this up while looking for something else and ended up reading every paragraph because it was actually informative, and after frostmeadowcollective I was sure I would come back, that does not happen often when most sites bury the useful parts under endless ads and pop ups today and across most categories online.
Justinbloms –
http://stromectolvip.com/# stromectol 3mg
yutingmgj –
2000 EUR + 225 Free Spins Wilfried Grasberger 18+. Responsible Gambling. Be Gamble Aware. | DMCA | Gambling Help Online Seven Seven Pots And Pearls Avalanche Reels Slot Aloha This can be particularly beneficial for beginners who are looking to enhance their gameplay and increase their chances of winning Many online casinos also feature live dealer games, where players can interact with real dealers in real time, adding an extra layer of excitement to the experience With just a few clicks, you can access a wide range of poker games at any time of day or night, without having to leave your home Casinos Macao Slot Aloha From welcome bonuses to loyalty rewards, players can enjoy extra cash to play with or even free tournament entries, increasing their chances of winning big To ensure a fair and secure gaming environment, reputable online poker sites implement strict security measures and use certified random number generators to guarantee the integrity of the games Online casino poker has become increasingly popular in recent years, providing players with a convenient way to enjoy their favorite card game from the comfort of their own homes Free Slot Machines Game
https://eci23.agrobiologie.cz/2026/04/27/discover-the-thrill-at-pokerpartyuk-trusted-casino-for-uk-players/
When playing high-stakes roulette variants online, high rollers get the chance to carefully consider their next bet and play the game at their own pace. The game can prove to be rather profitable, since it enables players to take all the time they need in order to choose and implement a suitable betting strategy. In fact, many roulette fans prefer to play online, as this way they are in control of every single aspect of the game, starting with the colour of the tablecloth and ending with the time allotted for each spin of the wheel. This documentation may be requested by the casino at any time, the bonus terms and conditions may not restrict you from playing table games. This currency can also be earned either through gameplay or by paying real money, this operator is also present online. Take what happened to Ukraine for example, as a desktop-only platform with a mobile app for iOS.
Chrisvoica –
sildenafil over the counter buy Viagra over the counter viagra canada
seothread –
Now recognising that this site has earned a place in the small group of resources I treat as authoritative, and a stop at seothread confirmed that placement, the difference between resources I trust and resources I just consume is real and this site has clearly moved into the trusted category through consistent quality over time.
Joshuafup –
rybelsus weight loss price [url=https://semaglutideglp1.com/#]glp-1 drugs for weight loss[/url] rybelsus coupon 2024
GeorgeChorm –
can you take rybelsus at night glp-1 drugs semaglutide clinic near me
Sylvesterboics –
Glad to find a site whose links lead somewhere worth going rather than back to itself for SEO juice, and a stop at finddealsnow kept that generous outbound feel, citing other peoples work with real respect rather than just for ranking signals is a sign of an honest operation worth supporting going forward.
mostbet_oumi –
mostbet kartdan depozit vaxtı [url=https://mostbet48932.help]mostbet kartdan depozit vaxtı[/url]
mostbet_jxea –
mostbet способы оплаты [url=www.mostbet09486.help]mostbet способы оплаты[/url]
mostbet_ynki –
aviator pe mostbet [url=www.mostbet80695.help]www.mostbet80695.help[/url]
rpgdvfidj –
The astronaut earning game is not your typical space game—it’s a thrilling crash-style betting game where you watch an astronaut’s rocket soar into space with a multiplier climbing every second. The catch? You have to decide when to cash out before the rocket crashes and you lose your bet. It’s like a high-stakes game of timing, combining luck and strategy for maximum adrenaline. From the astronaut game app to the astronaut game pc version, this game has taken Pakistan’s online gaming scene by storm. Auto-Betting Options: For convenience, you can set up auto-betting and auto-cash-out, allowing you to automatically place bets and cash out at a chosen multiplier. Astronaut is a video slot game created by the provider Red Tiger Gaming. In this Astronaut slot review you’ll learn about its core features (including RTP, max win, and volatility), the bonus mechanics, and what helps the game stand out — along with the areas where it may fall short.
https://turkeycreekbaptistchurch.org/2026/04/27/an-honest-bonusstrikecasino-review-for-uk-players-spin-rewards-and-more/
Slot Aloha With just a few clicks, you can access a wide range of poker games at any time of day or night, without having to leave your home From classic Texas Hold’em to Omaha and Stud poker variations, players can choose from a wide range of options to keep their gaming experience fresh and exciting In addition to games, software, and bonuses, the customer support provided by an online casino is another crucial aspect to consider Spartan Slot Game You may get free coins, spins, credits, power-ups, bonus, prizes, diamonds, rewards, golds, puzzle, cards, special bonus or any other gifts for your game: at hoffreespins. We are deliberately aiming to satisfy your gaming with House of Freebies website. We will be posting links of all legitimate freebies here everyday. We emphasized that only legitimate game freebies are posted because of so many bogus freebies or non-functional freebies are also circulating online. But we are also open to possibility that you may experience irregularities of our freebie & gift links.
Jessesaw –
http://victopharm.com/# new pharmacy online
tyr v spb_lapn –
культурно экскурсионная программа [url=https://tury-v-spb.com]https://tury-v-spb.com[/url]
mostbet_bvMi –
pobieranie mostbet apk [url=www.mostbet90617.help]www.mostbet90617.help[/url]
frostpetalemporium –
Useful read, especially because the writer did not assume too much background from the reader, and a quick look at frostpetalemporium continued in the same way, a thoughtful site that meets people where they are which is something the modern web could use a lot more of for both casual and serious readers.
melbet_fuSl –
melbet пополнение через карту [url=http://melbet35702.help]http://melbet35702.help[/url]
seotrail –
Solid stuff, the kind of post that I will probably refer back to later this month when the topic comes up again, and a look at seotrail only confirmed I should bookmark the site as a whole rather than just this single page for future reference and use across coming weeks.
mostbet_aoea –
mostbet восстановление аккаунта [url=http://mostbet09486.help]http://mostbet09486.help[/url]
RussellBum –
liraglutide online LiraglutideGlp1 liraglutide fast delivery
PhillipTeags –
However casually I came to this site I have ended up reading carefully, and a look at findnewdeals continued earning that careful reading, the conversion from casual visitor to careful reader is something content earns rather than demands and this site has accomplished that conversion for me over the course of just a few pieces.
mostbet_gsmi –
mostbet pul yatırma [url=https://mostbet48932.help]mostbet pul yatırma[/url]
mostbet_cvki –
mostbet fără verificare [url=https://mostbet80695.help/]https://mostbet80695.help/[/url]
mostbet_uhmi –
mostbet kart təsdiqi [url=www.mostbet48932.help]mostbet kart təsdiqi[/url]
Jessesaw –
https://semaglutideglp1.shop/# is semaglutide going away
seovista –
Reading this triggered a small but real correction in something I had assumed, and a stop at seovista extended that corrective effect, content that updates my beliefs through evidence rather than rhetoric is content with intellectual integrity and this site has earned that label consistently across the pieces I have read so far today.
Donaldkeete –
average weight loss on semaglutide glp-1 drugs semaglutide without prescription
frostpetalstore –
Picked this site to mention to a colleague who would benefit, and a look at frostpetalstore added more material I will pass along, recommending sites to colleagues is a higher bar than recommending to friends because the professional context demands more careful curation and this site cleared the professional bar without me having to think.
GeorgeChorm –
buy victoza online victoza generic liraglutide pharmacy
ChristianHax –
Honest reaction is that I want to send this to a friend who would benefit from it, and a look at yourdailydeals added more material I will pass along too, the impulse to share is the strongest signal I have for content quality and this site is generating that impulse cleanly across multiple posts.
RussellBum –
cheap liraglutide victoza generic liraglutide pharmacy
melbet_ffoi –
мелбет новая версия apk [url=http://melbet70382.help/]http://melbet70382.help/[/url]
otpgdiqzy –
Además, es fundamental comprender el funcionamiento de la ronda de bonificación y los multiplicadores. Observar las rondas de otros jugadores y analizar sus resultados puede proporcionar información valiosa sobre cómo funcionan los símbolos de multiplicadores y qué combinaciones generan mayores ganancias. La practica con la demo Gates Of Olympus permite comprender mejor estas estrategias. Subimos el nivel en mantenimiento de ascensores Ahora que ya conoces todas las características técnicas y las reglas del juego, es momento de explicarte de inicio a fin cómo jugar en esta tragamonedas. El proceso es bastante intuitivo y puedes usar la versión de Gates of Olympus demo para practicar cada uno de los siguientes pasos: Gates of Olympus presenta unos gráficos impactantes y un diseño sofisticado. Las animaciones son fluidas y atractivas, lo que convierte cada giro en una agradable visita.
https://sanmarcossierras.com/?p=134331
ITT Canarias es distribuidor oficial de maquinaria para la construcción y la industria. Damos servicio de primeras marcas como: Case CE, Bobcat, MB Crusher, Hamm, Putzmeister, Arden, Kleeman, Jenz, Tana, Lindner, Edge, Franzoi Sigue estos pasos para saber cu00f3mo jugar a Gates of Olympus y empieza a disfrutar el juego con dinero real. Una vez te encuentres registrado en un casino online que te guste, podru00e1s jugar a Gates of Olympus gratis o con dinero real, haciendo depu00f3sitos ru00e1pidos y muy seguros al instante. Gates of Olympus está cargado de funciones que pueden desatar premios monumentales: Fitur multiplier dalam slot demo pg soft wild bounty dimulai dengan pengali x1 di setiap putaran utama. Jika terdapat satu atau lebih simbol kemenangan selama putaran, setelah pembayaran dilakukan dan simbol-simbol baru jatuh, nilai pengali akan bertambah dua kali lipat. Pengali kemenangan dapat terus meningkat hingga mencapai maksimal x1.024, memberikan kesempatan untuk memenangkan hadiah yang lebih besar dalam permainan.
tyr v spb_rnpn –
за путевкой рф санкт петербург подбор тура [url=www.tury-v-spb.com]за путевкой рф санкт петербург подбор тура[/url]
shopmint –
Reading this confirmed a hunch I had been carrying about the topic without having articulated it, and a stop at shopmint extended the confirmation, content that gives shape to fuzzy intuitions is doing the rare work of making private thoughts public and this site is providing that articulating service consistently for me lately.
Jessesaw –
https://victopharm.com/# pharmacy online
Joshuafup –
sublingual semaglutide reviews [url=https://semaglutideglp1.com/#]semaglutide other names[/url] bmi for semaglutide
mostbet_myea –
мостбет лимит ставок [url=mostbet09486.help]мостбет лимит ставок[/url]
RussellBum –
glp-1 cheap liraglutide liraglutide online
Jessesaw –
https://victopharm.com/# best online pharmacy
mostbet_moki –
cum primesc pariu gratuit la mostbet [url=https://mostbet80695.help/]https://mostbet80695.help/[/url]
GeorgeChorm –
glp 1 generic liraglutide liraglutide online
mostbet_goki –
mostbet link de acces [url=https://www.mostbet80695.help]https://www.mostbet80695.help[/url]
RussellBum –
online drugs order Victo Pharm legitimate online pharmacy
tyr v spb_ompn –
туры в санкт петербурга [url=http://tury-v-spb.com]http://tury-v-spb.com[/url]
Jessesaw –
https://victopharm.com/# online pharmacy no prescription needed
RussellBum –
liraglutide online LiraglutideGlp1 liraglutide online
Joshuafup –
rybelsus india [url=https://semaglutideglp1.shop/#]glp-1[/url] when does semaglutide start working
GeorgeChorm –
liraglutide online LiraglutideGlp1 victoza weight loss
Jessesaw –
https://victopharm.shop/# best rx pharmacy online
RussellBum –
rybelsus tab 7mg glp-1 drugs over the counter semaglutide online prescription
tyr v spb_efpn –
пакетный тур в санкт петербург [url=www.tury-v-spb.com]пакетный тур в санкт петербург[/url]
Jessesaw –
https://semaglutideglp1.shop/# can you take wegovy and rybelsus together
Donaldkeete –
worldwide pharmacy international pharmacy no prescription pharmacy paypal
RussellBum –
how to pronounce semaglutide rybelsus prix how to get rybelsus
Jessesaw –
http://liraglutideglp1.com/# liraglutide
Joshuafup –
buy liraglutide online [url=https://liraglutideglp1.com/#]liraglutide price[/url] generic liraglutide
RussellBum –
glp-1 buy liraglutide online victoza delivery
Jessesaw –
https://semaglutideglp1.com/# rybelsus sglt2
Donaldkeete –
what is rybelsus glp-1 drugs for weight loss semaglutide make you tired
Jerri –
Nieuwe xxx sites bieden geavanceerde ibhoud voor volwassenen.
Kies oor gegarandeerde platforms voor veilig kijken.
Feel free to surf to my web-site: BUY VIAGRA ONLINE
GeorgeChorm –
victoza delivery LiraglutideGlp1 buy liraglutide online
frostpinecollective –
Now considering the post as evidence that careful blog writing is still possible, and a look at frostpinecollective extended that evidence, the broader question of whether the modern web can sustain quality writing has obvious empirical answers in sites like this one and seeing them is reassuring even when they remain a minority overall today.
melbet_ujst –
melbet тоталӣ [url=www.melbet74319.help]www.melbet74319.help[/url]
melbet_byPa –
joc lucky jet melbet [url=http://melbet52780.help]http://melbet52780.help[/url]
melbet_bmMa –
melbet metode de plata [url=melbet95431.help]melbet metode de plata[/url]
pinup_dden –
pin-up mantenimiento Chile [url=pinup2004.help]pinup2004.help[/url]
RussellBum –
online pharmacy buy online medicine foreign online pharmacy
mostbet_rcPl –
mostbet plinko turnir [url=www.mostbet48217.help]www.mostbet48217.help[/url]
melbet_fjPa –
contact melbet [url=https://melbet52780.help/]https://melbet52780.help/[/url]
melbet_imst –
melbet app барои ios [url=www.melbet74319.help]www.melbet74319.help[/url]
frostshoregoods –
Solid post, the structure is easy to follow and the language stays simple even when the topic gets a bit more involved, and a look at frostshoregoods kept that same standard going, so I left feeling like the time spent here was actually worth something for once which is rare lately.
MichaelInhap –
Viagra without a doctor prescription Canada [url=https://urohealthdaily.com/#]Buy generic 100mg Viagra online[/url] Cheap Viagra 100mg
melbet_bhPa –
melbet aplicatie [url=www.melbet52780.help]www.melbet52780.help[/url]
melbet_zrst –
мелбет сабти ном бе хато [url=http://melbet74319.help/]мелбет сабти ном бе хато[/url]
ClintShulp –
Cheap generic Viagra online UroHealth Daily – best price for viagra 100mg
RandallVials –
https://urohealthdaily.com/# buy viagra here
pinup_ypen –
pin-up rollover bono [url=https://pinup2004.help/]pin-up rollover bono[/url]
melbet_htMa –
login cont melbet [url=https://melbet95431.help]login cont melbet[/url]
pinup_qyen –
pin-up promo code [url=www.pinup2004.help]www.pinup2004.help[/url]
melbet_meMa –
melbet Republica Moldova pariuri [url=melbet95431.help]melbet95431.help[/url]
mostbet_biPl –
mostbet ordinar [url=https://mostbet48217.help/]https://mostbet48217.help/[/url]
mostbet_kiPl –
mostbet tez ochiladigan sayt [url=https://mostbet48217.help/]mostbet tez ochiladigan sayt[/url]
melbet_jtPa –
melbet aviator bonus [url=https://melbet52780.help/]https://melbet52780.help/[/url]
melbet_urst –
мелбет коди бонус 2026 [url=http://melbet74319.help/]http://melbet74319.help/[/url]
AndresSmeam –
Хочешь испытать азарт? покерок официальный сайт онлайн-покер с турнирами, кэш-столами и бонусами для игроков. Удобный интерфейс, мобильное приложение и регулярные покерные серии. Играйте в холдем, омаху и участвуйте в крупных турнирах.
Anthonyphict –
sildenafil over the counter UroHealth Daily – Generic Viagra online
glowforgeessentials –
Really like that there are no exclamation marks or all caps shouting throughout the post, and a quick visit to glowforgeessentials maintained the same calm voice, restraint in punctuation signals confidence in the content and this site clearly trusts its substance to do the persuading rather than relying on typographic emphasis.
pinup_pqen –
pinup apk [url=https://pinup2004.help/]https://pinup2004.help/[/url]
melbet_lnMa –
melbet pariuri pe cornere [url=melbet95431.help]melbet95431.help[/url]
mostbet_fdPl –
mostbet qollab-quvvatlash [url=http://mostbet48217.help/]http://mostbet48217.help/[/url]
ClintShulp –
best price for viagra 100mg UroHealth Daily – Cheap Sildenafil 100mg
RandallVials –
https://urohealthdaily.com/# buy viagra here
Anthonyphict –
buy Viagra over the counter Viagra generic over the counter – Order Viagra 50 mg online
maplecrestgoods –
Started smiling at one paragraph because the writing was just nice, and a look at maplecrestgoods produced a couple more such moments, prose that produces small spontaneous reactions in the reader is doing more than just transferring information and the writers here are clearly hitting that level fairly consistently throughout pieces.
MichaelInhap –
cheapest viagra [url=http://urohealthdaily.com/#]Viagra tablet online[/url] viagra canada
Anthonyphict –
Cheap generic Viagra online UroHealth Daily – Cheap Viagra 100mg
mysticbaygoods –
Now planning to share the link with a small group of readers I trust, and a look at mysticbaygoods suggested more material to share with the same group, recommending content into a curated circle requires confidence in the recommendation and this site is making me confident in those personal recommendations on multiple separate occasions now.
ClintShulp –
Cheap Viagra 100mg viagra canada – over the counter sildenafil
piter na teplohode_chOl –
экскурсионный тур в петербург [url=https://www.piter-na-teplohode.ru]https://www.piter-na-teplohode.ru[/url]
mostbet_szKl –
mostbet yechish uchun karta [url=https://mostbet56934.help/]https://mostbet56934.help/[/url]
mostbet_nwsa –
mostbet reklamace výběru [url=www.mostbet41862.help]www.mostbet41862.help[/url]
RandallVials –
https://urohealthdaily.shop/# generic sildenafil
mostbet_oxor –
mostbet акции [url=http://mostbet20581.help/]http://mostbet20581.help/[/url]
Anthonyphict –
Sildenafil 100mg price Viagra without a doctor prescription Canada – Cheap generic Viagra online
mysticbaystore –
Better signal to noise ratio than most places I check on this kind of topic, and a look at mysticbaystore kept that going, every paragraph here carries something worth reading rather than padding out the page to hit some arbitrary length target that search engines reward but readers ignore as soon as they notice it.
Deweyzox –
Продажа и установка камеры видеонаблюдения купить. Современные системы безопасности для квартир, домов, магазинов и складов. Настройка удалённого доступа, запись видео и круглосуточный контроль объекта.
Alfredozex –
Быстрая профессиональная монтаж видеонаблюдения для квартир, домов, офисов и коммерческих объектов. Проектирование, монтаж и настройка систем безопасности, удалённый доступ, запись видео и контроль в реальном времени. Надёжные решения для защиты имущества и контроля территории.
ClintShulp –
sildenafil online buy Viagra over the counter – Buy generic 100mg Viagra online
melbet_mzEn –
melbet kz email поддержки [url=https://www.melbet85713.help]https://www.melbet85713.help[/url]
mysticfieldmarket –
Considered alongside other sources I have been reading this one consistently rises to the top, and a stop at mysticfieldmarket maintained that top ranking, the informal ongoing comparison between sources is something I do whenever reading on a topic and this site keeps coming out near the top of those comparisons over many sessions.
MichaelInhap –
Cheap generic Viagra [url=http://urohealthdaily.com/#]UroHealth Daily[/url] Buy generic 100mg Viagra online
mostbet_kssa –
mostbet bitcoin [url=http://mostbet41862.help]http://mostbet41862.help[/url]
mostbet_ruea –
zakłady na żywo mostbet [url=www.mostbet82175.help]www.mostbet82175.help[/url]
mostbet_vnma –
mostbet çıxarış statusu [url=https://mostbet68324.help]mostbet çıxarış statusu[/url]
mostbet_dssa –
mostbet platby Česko [url=http://mostbet41862.help]http://mostbet41862.help[/url]
mostbet_zcor –
mostbet ставки приложение [url=http://mostbet20581.help]http://mostbet20581.help[/url]
mostbet_jxor –
мостбет мой аккаунт [url=http://mostbet20581.help/]мостбет мой аккаунт[/url]
Anthonyphict –
viagra without prescription cheap viagra – Cheap Viagra 100mg
mostbet_adsa –
lucky jet mostbet tipy [url=http://mostbet41862.help]lucky jet mostbet tipy[/url]
mysticoakmarket –
Halfway through I knew I would finish the post, and a stop at mysticoakmarket also held me through to the end, content that signals its quality early and then sustains it is content with real internal consistency and this site has clearly figured out how to maintain quality from opening sentence through to closing thought.
mostbet_qtor –
mostbet чат поддержки [url=mostbet20581.help]mostbet20581.help[/url]
Anthonyphict –
best price for viagra 100mg UroHealth Daily – Viagra online price
mostbet_pgma –
mostbet download olmur [url=https://www.mostbet68324.help]https://www.mostbet68324.help[/url]
mostbet_oiea –
mostbet oszustwo czy nie [url=https://www.mostbet82175.help]https://www.mostbet82175.help[/url]
mostbet_klKl –
mostbet karta boglash [url=https://mostbet56934.help]https://mostbet56934.help[/url]
mostbet_emma –
mostbet tətbiq [url=http://mostbet68324.help/]http://mostbet68324.help/[/url]
mostbet_omea –
mostbet zarejestruj [url=https://www.mostbet82175.help]https://www.mostbet82175.help[/url]
mostbet_vjKl –
mostbet aviator oynash [url=http://mostbet56934.help]http://mostbet56934.help[/url]
mysticpetalgoods –
Felt the writer was being honest with the reader which is rare enough that I want to acknowledge it, and a look at mysticpetalgoods continued that honest feel, content built on actual knowledge rather than aggregated summaries is something I value highly and rarely come across in regular searches on the open internet these days.
melbet_gbEn –
melbet app скачать [url=http://melbet85713.help]http://melbet85713.help[/url]
Anthonyphict –
Sildenafil 100mg price cheap viagra – viagra canada
mostbet_mbKl –
mostbet qoidabuzarlik [url=http://mostbet56934.help]http://mostbet56934.help[/url]
mostbet_arma –
mostbet tətbiq giriş problemi [url=http://mostbet68324.help]http://mostbet68324.help[/url]
mostbet_beea –
mostbet czas wypłaty [url=www.mostbet82175.help]mostbet czas wypłaty[/url]
melbet_vaEn –
melbet kz верификация карты [url=https://melbet85713.help/]melbet kz верификация карты[/url]
MichaelInhap –
Cheap generic Viagra [url=https://urohealthdaily.com/#]UroHealth Daily[/url] Cheap generic Viagra
melbet_lvEn –
crash игра melbet [url=https://melbet85713.help]crash игра melbet[/url]
mysticridgegoods –
The tone stayed consistent across the whole post which is harder than it looks for longer pieces, and a look at mysticridgegoods continued the same voice, this kind of editorial consistency is a sign of either a single careful writer or a tightly run team and either is impressive today across the broader media environment.
KennethGrows –
Tadalafil Tablet cialis for sale – Cialis without a doctor prescription
aviator_ccei –
aviator multiplier [url=http://aviator09317.help/]http://aviator09317.help/[/url]
aviator_ecki –
aviator slots apk [url=www.aviator68130.help]www.aviator68130.help[/url]
mysticshorecollective –
Now realising the post solved a small problem I had been carrying for weeks, and a look at mysticshorecollective extended that problem solving function, content that connects to specific unresolved questions in my own life rather than just providing general interest is content with real practical impact and this site is providing that practical value.
KennethGrows –
Tadalafil Tablet Tadalafil Tablet – Tadalafil price
ClaytonByday –
Tadalafil Tablet http://mensrxguide.org/# Cialis 20mg price
Timothydot –
Buy Tadalafil 5mg [url=https://mensrxguide.org/#]Buy Cialis online[/url] Cialis 20mg price
piter na teplohode_bxOl –
туры в питер [url=https://piter-na-teplohode.ru]туры в питер[/url]
mostbet_smmi –
mostbet промокод на сегодня Кыргызстан [url=http://mostbet47129.help/]mostbet промокод на сегодня Кыргызстан[/url]
melbet_thEt –
melbet купон ставок [url=http://melbet67043.help/]http://melbet67043.help/[/url]
aviator_waMr –
aviator novo link [url=https://aviator71803.help/]https://aviator71803.help/[/url]
mostbet_fwOl –
мостбет букмекер 2026 [url=https://www.mostbet36014.help]https://www.mostbet36014.help[/url]
aviator_nwei –
aviator saxta sayt [url=http://aviator09317.help/]http://aviator09317.help/[/url]
mostbet_gbmn –
mostbet сколько идет вывод [url=https://mostbet14967.help]mostbet сколько идет вывод[/url]
JudsonWed –
A nicely understated post that does not shout for attention, and a look at shoptheday maintained the same quiet quality, understatement is a stylistic choice that distinguishes serious writing from attention seeking writing and this site has clearly committed to the understated approach as a core editorial value rather than just a phase.
aviator_ytei –
aviator crash strategiya [url=https://www.aviator09317.help]https://www.aviator09317.help[/url]
ClaytonByday –
Buy Tadalafil 5mg http://mensrxguide.org/# buy cialis pill
KennethGrows –
cheapest cialis MensRxGuide – Generic Cialis price
mysticthreadstore –
A thoughtful read in a week that has been mostly noisy, and a look at mysticthreadstore carried that thoughtful quality across more pages, finding pockets of considered writing in a week of distractions is one of the small wins of careful curation and this site is providing those pockets at a sustainable rate.
aviator_waei –
aviator mines bonus [url=http://aviator09317.help]http://aviator09317.help[/url]
mostbet_akmi –
mostbet вход ошибка [url=www.mostbet47129.help]www.mostbet47129.help[/url]
dreamgrovehub –
Took a few notes from this post, the points are easy to remember without needing to come back and check, and a look at dreamgrovehub added a couple more, the kind of place that sticks in the memory long after the browser tab has been closed for the day which says a lot really.
mostbet_fvmi –
mostbet как пополнить MasterCard [url=http://mostbet47129.help]mostbet как пополнить MasterCard[/url]
aviator_jkMr –
aviator apostas esportivas [url=https://www.aviator71803.help]aviator apostas esportivas[/url]
melbet_jhEt –
melbet android официальное приложение [url=melbet67043.help]melbet67043.help[/url]
mostbet_icOl –
мостбет игровые автоматы [url=https://mostbet36014.help/]https://mostbet36014.help/[/url]
oakpetalemporium –
Reading this slowly and letting each paragraph land before moving on, and a stop at oakpetalemporium earned the same patient approach, content that rewards slow reading rather than speed is content with real density and the writers here are clearly producing work that benefits from the careful eye rather than the rushed scan.
KennethGrows –
Cialis 20mg price in USA MensRxGuide – Buy Tadalafil 20mg
mostbet_ywmn –
mostbet как пройти верификацию [url=mostbet14967.help]mostbet14967.help[/url]
aviator_giMr –
aviator como receber [url=https://aviator71803.help/]aviator como receber[/url]
melbet_yvEt –
мелбет лента событий [url=http://melbet67043.help]http://melbet67043.help[/url]
mostbet_ygOl –
aviator мостбет [url=mostbet36014.help]aviator мостбет[/url]
mostbet_wrmn –
мостбет скачать 2026 [url=https://mostbet14967.help]мостбет скачать 2026[/url]
discoverfashioncorner –
Picked this for my morning read because the topic seemed worth the time, and a look at discoverfashioncorner confirmed the choice was right, my morning reading slot is precious and giving it to this site felt like a good investment rather than a waste which is a higher endorsement than I usually offer for content.
melbet_wqol –
melbet bangladesh bypass blocking [url=www.melbet58273.help]www.melbet58273.help[/url]
aviator_vjMr –
aviator pagamento seguro [url=aviator71803.help]aviator71803.help[/url]
melbet_kaEt –
мелбет фора [url=https://melbet67043.help]мелбет фора[/url]
mostbet_qqOl –
mostbet скачать Кыргызстан [url=http://mostbet36014.help]http://mostbet36014.help[/url]
mostbet_hhmi –
мостбет лимит ставок [url=https://mostbet47129.help/]https://mostbet47129.help/[/url]
mostbet_clmn –
mostbet верификация [url=http://mostbet14967.help/]mostbet верификация[/url]
discoveramazingdeals –
Worth flagging that this approach to the topic is fresh without being contrarian, and a stop at discoveramazingdeals extended the same fresh angle, finding original perspective on familiar subjects is rare and this site has clearly developed its own way of seeing rather than echoing the dominant takes from elsewhere consistently.
KennethGrows –
Cialis over the counter Buy Tadalafil 5mg – Tadalafil Tablet
aviator_vuki –
aviator jackpot slots [url=http://aviator68130.help/]http://aviator68130.help/[/url]
dailyfashioncorner –
Halfway through reading I knew this would be one to bookmark, and a look at dailyfashioncorner confirmed that early intuition, when bookmark intent forms before finishing a post you know the writing has cleared a quality bar that most content fails to clear and this site has cleared it on multiple visits already.
KennethGrows –
Tadalafil Tablet MensRxGuide – Tadalafil price
plinko_ffpa –
plinko fast withdrawal [url=http://plinko62894.help/]http://plinko62894.help/[/url]
melbet_tbol –
melbet website customer support [url=melbet58273.help]melbet58273.help[/url]
creativegiftboutique –
A piece that handled a controversial angle without becoming heated, and a look at creativegiftboutique continued that calm engagement, content that can address contested topics without inflaming them is doing rare diplomatic work and this site has clearly developed the editorial maturity to handle sensitive material with the appropriate temperature of writing throughout.
melbet_jbol –
melbet bonus wagering [url=https://melbet58273.help]melbet bonus wagering[/url]
aviator_nmki –
aviator casino [url=www.aviator68130.help]www.aviator68130.help[/url]
aviator_utki –
aviator daily tournament [url=https://www.aviator68130.help]https://www.aviator68130.help[/url]
KennethGrows –
Generic Cialis without a doctor prescription Cialis without a doctor prescription – Cialis over the counter
melbet_xlol –
melbet mirror link [url=https://www.melbet58273.help]https://www.melbet58273.help[/url]
aviator_nqki –
aviator plinko game [url=https://www.aviator68130.help]https://www.aviator68130.help[/url]
mostbet_kxMl –
мостбет как пройти верификацию [url=https://www.mostbet81396.help]мостбет как пройти верификацию[/url]
mostbet_vjpi –
mostbet biztonságos tükör [url=mostbet50472.help]mostbet50472.help[/url]
mostbet_frea –
mostbet сом пополнение [url=https://mostbet23586.help]mostbet сом пополнение[/url]
plinko_hapa –
how to withdraw to Rocket from plinko [url=https://www.plinko62894.help]https://www.plinko62894.help[/url]
melbet_lpkn –
melbet сайт не работает [url=www.melbet87025.help]www.melbet87025.help[/url]
plinko_zlpa –
plinko Rocket payment [url=https://www.plinko62894.help]plinko Rocket payment[/url]
KennethGrows –
Cheap Cialis MensRxGuide – Cialis 20mg price
plinko_bapa –
plinko games [url=https://www.plinko62894.help]https://www.plinko62894.help[/url]
mostbet_sbMl –
мостбет приложение не работает [url=https://www.mostbet81396.help]мостбет приложение не работает[/url]
mostbet_hhMl –
mostbet скачать приложение с официального сайта [url=http://mostbet81396.help]mostbet скачать приложение с официального сайта[/url]
mostbet_ripi –
mostbet stream nézés [url=https://www.mostbet50472.help]https://www.mostbet50472.help[/url]
Brianliste –
semaglutide https://usobesityscience.org/liraglutide-studies/ how many units is 0.25 mg of semaglutide
mostbet_xdea –
mostbet вход по номеру [url=www.mostbet23586.help]www.mostbet23586.help[/url]
mostbet_tapi –
mostbet app helyett böngésző [url=http://mostbet50472.help]http://mostbet50472.help[/url]
melbet_xgkn –
как установить melbet apk [url=https://www.melbet87025.help]https://www.melbet87025.help[/url]
mostbet_omea –
мостбет ставки на теннис Кыргызстан [url=mostbet23586.help]mostbet23586.help[/url]
melbet_qskn –
мелбет support кыргызстан [url=https://melbet87025.help]мелбет support кыргызстан[/url]
mostbet_zmMl –
мостбет коэффициенты [url=www.mostbet81396.help]www.mostbet81396.help[/url]
Brianliste –
orlistat https://usobesityscience.org/glp-1-agonists/ victoza weight loss
mostbet_wfpi –
mostbet bónusz szabályok magyarul [url=www.mostbet50472.help]www.mostbet50472.help[/url]
mostbet_yhea –
мостбет не приходит код [url=www.mostbet23586.help]www.mostbet23586.help[/url]
melbet_xukn –
как вывести выигрыш мелбет [url=www.melbet87025.help]как вывести выигрыш мелбет[/url]
Brianliste –
liraglutide https://usobesityscience.org/glp-1-agonists/ where to get compounded semaglutide
pinup_zosa –
mines pin-up Chile [url=https://pinup84291.help]https://pinup84291.help[/url]
plinko_mkka –
plinko рабочий сайт [url=https://www.plinko83214.help]https://www.plinko83214.help[/url]
Brianliste –
semaglutide https://usobesityscience.org/glp-1-agonists/ semaglutide weight loss near me
Brianliste –
glp-1 agonists https://usobesityscience.org/semaglutide-research/ does semaglutide help with pcos
plinko_zmka –
plinko скачать с официального сайта [url=https://plinko83214.help]https://plinko83214.help[/url]
pinup_lwsa –
pin-up póker Chile [url=pinup84291.help]pinup84291.help[/url]
pinup_fpsa –
juego mines pinup [url=https://pinup84291.help]https://pinup84291.help[/url]
plinko_muka –
скачать plinko [url=https://plinko83214.help/]https://plinko83214.help/[/url]
Brianliste –
Advancing Clinical Research in Metabolic Health and Weight Management https://usobesityscience.org/glp-1-agonists/ what is semaglutide made of
pinup_wusa –
pin-up promociones [url=http://pinup84291.help]http://pinup84291.help[/url]
plinko_kvka –
плинко вывод без верификации [url=www.plinko83214.help]www.plinko83214.help[/url]
Brianliste –
liraglutide https://usobesityscience.org/tirzepatide-analysis/ zepbound vs semaglutide
pinup_hlSa –
pin up mines demo [url=http://pinup50413.help]pin up mines demo[/url]
pinup_anPn –
pin-up voleybol mərc [url=http://pinup56439.help]http://pinup56439.help[/url]
mostbet_etEi –
mostbet apelsin [url=https://mostbet20439.help]https://mostbet20439.help[/url]
Brianliste –
orlistat https://usobesityscience.org/orlistat-clinical-review/ liraglutide otc
pinup_kgSa –
pin-up kupon kod [url=https://pinup50413.help/]https://pinup50413.help/[/url]
pinup_fnSa –
pinup ios ilova ishlamayapti [url=https://pinup50413.help/]https://pinup50413.help/[/url]
Brianliste –
AMRI https://usobesityscience.org/glp-1-agonists/ cheap victoza
pinup_efSa –
pinup apk qanday o‘rnatish [url=pinup50413.help]pinup50413.help[/url]
mostbet_zqMi –
авиатор мостбет [url=https://mostbet43287.help]https://mostbet43287.help[/url]
pinup_vbPn –
pin-up plinko demo qeydiyyatsız [url=https://pinup56439.help]https://pinup56439.help[/url]
mostbet_qmEi –
mostbet joriy mirror [url=https://www.mostbet20439.help]https://www.mostbet20439.help[/url]
pinup_owPn –
pin-up oyun siyahısı [url=http://pinup56439.help/]http://pinup56439.help/[/url]
mostbet_gyEi –
mostbet Buxoro [url=https://mostbet20439.help]https://mostbet20439.help[/url]
Brianliste –
tirzepatide https://usobesityscience.org/ semaglutide near me
aviator_diEi –
aviator लॉस रिकवरी स्ट्रेटेजी [url=https://aviator50639.help]https://aviator50639.help[/url]
pinup_zuPn –
pin-up lucky jet minimum mərc [url=https://www.pinup56439.help]pin-up lucky jet minimum mərc[/url]
mostbet_njEi –
aviator oyini mostbet [url=www.mostbet20439.help]aviator oyini mostbet[/url]
Brianliste –
us obesity science https://usobesityscience.org/glp-1-agonists/ semaglutide thyroid cancer
mostbet_beMi –
mostbet mines [url=http://mostbet43287.help]mostbet mines[/url]
mostbet_urMi –
как активировать промокод мостбет [url=http://mostbet43287.help]http://mostbet43287.help[/url]
aviator_jjEi –
aviator से रोज कमाई [url=www.aviator50639.help]aviator से रोज कमाई[/url]
aviator_jaEi –
aviator रजिस्ट्रेशन कैसे करें [url=http://aviator50639.help/]http://aviator50639.help/[/url]
mostbet_koMi –
как зарегистрироваться в mostbet [url=mostbet43287.help]mostbet43287.help[/url]
Brianliste –
glp-1 agonists https://usobesityscience.org/orlistat-clinical-review/ rybelsus stock
aviator_ghEi –
aviator वैगरिंग कैसे पूरी करें [url=http://aviator50639.help]http://aviator50639.help[/url]
Brianliste –
Advancing Clinical Research in Metabolic Health and Weight Management https://usobesityscience.org/glp-1-agonists/ what happens if you take rybelsus with food
mostbet_yrpr –
mostbet регистрация аккаунта [url=https://mostbet97142.help]https://mostbet97142.help[/url]
RodneyTaria –
jardiance vs rybelsus glp-1 agonists
Brianliste –
American Metabolic Research Institute https://usobesityscience.org/semaglutide-research/ victoza generic
mostbet_evpr –
мостбет надежность [url=https://www.mostbet97142.help]мостбет надежность[/url]
mostbet_ykpr –
мостбет mines 2026 [url=http://mostbet97142.help/]http://mostbet97142.help/[/url]
mostbet_xdPa –
mostbet новый адрес [url=http://mostbet60398.help/]http://mostbet60398.help/[/url]
mostbet_yvsi –
mostbet скачать бесплатно [url=http://mostbet93268.help]mostbet скачать бесплатно[/url]
mostbet_bwpr –
мостбет скачать Кыргызстан [url=https://mostbet97142.help/]https://mostbet97142.help/[/url]
RodneyTaria –
semaglutide cost AMRI
Timothyduaft –
п»їbuy liraglutide glp-1 agonists
Brianliste –
tirzepatide https://usobesityscience.org/ liraglutide
Brianliste –
tirzepatide https://usobesityscience.org/glp-1-agonists/ how long can you take semaglutide
RodneyTaria –
liraglutide pharmacy us obesity science
Timothyduaft –
rybelsus side effect semaglutide
mostbet_xjPa –
mostbet новый адрес [url=https://mostbet60398.help/]https://mostbet60398.help/[/url]
mostbet_yisi –
mostbet кэшбэк на ставки [url=https://www.mostbet93268.help]mostbet кэшбэк на ставки[/url]
mostbet_wcsi –
aviator мостбет [url=https://mostbet93268.help]https://mostbet93268.help[/url]
mostbet_chPa –
мостбет зеркало Киргизия [url=www.mostbet60398.help]www.mostbet60398.help[/url]
Brianliste –
AMRI https://usobesityscience.org/glp-1-agonists/ rybelsus oral semaglutide
RodneyTaria –
liraglutide pharmacy Advancing Clinical Research in Metabolic Health and Weight Management
mostbet_qmPa –
мостбет сколько идет вывод [url=http://mostbet60398.help/]http://mostbet60398.help/[/url]
mostbet_lgsi –
mostbet ссылка на зеркало [url=https://mostbet93268.help/]https://mostbet93268.help/[/url]
Timothyduaft –
rybelsus for weight loss reviews Advancing Clinical Research in Metabolic Health and Weight Management
budgetfriendlystore –
Reading this triggered a small change in how I think about the topic going forward, and a stop at budgetfriendlystore reinforced that subtle shift, the rare content that actually moves my thinking rather than just confirming or filling it is the kind I most value and this site is providing that kind of impact today.
aviator_unSl –
aviator कैशबैक [url=www.aviator63791.help]www.aviator63791.help[/url]
mostbet_rwKn –
mostbet депозит намешавад [url=https://www.mostbet13748.help]https://www.mostbet13748.help[/url]
mostbet_lgoa –
mostbet limită retragere [url=http://mostbet63247.help]mostbet limită retragere[/url]
brightwatershoppe –
Following a few of the internal links revealed more posts of similar quality, and a stop at brightwatershoppe added more to that growing pile, sites where internal links lead to more good content rather than to more of the same recycled material are sites with depth and this one has clearly built that depth carefully.
Brianliste –
AMRI https://usobesityscience.org/ semaglutide with b12
Timothyduaft –
п»їbuy liraglutide Advancing Clinical Research in Metabolic Health and Weight Management
brighttrailfashion –
Quiet confidence runs through the whole post, no need to shout to make the points stick, and a stop at brighttrailfashion carried that same restrained voice forward, content that respects the reader by trusting its own substance rather than dressing it up in theatrical language is what I look for online and rarely actually find these days.
mostbet_acSa –
mostbet logout [url=www.mostbet63875.help]www.mostbet63875.help[/url]
Brianliste –
American Metabolic Research Institute https://usobesityscience.org/liraglutide-studies/ semaglutide drugs
brightrootcollection –
Once I trust a site this much I tend to read everything they publish and that is the trajectory I am on with this one, and a stop at brightrootcollection confirmed the trajectory, the rare progression from interested reader to comprehensive reader is something only certain sites earn and this one is earning that progression rapidly.
mostbet_joKn –
mostbet хуруҷ дер шуд [url=mostbet13748.help]mostbet13748.help[/url]
aviator_rcSl –
aviator ios पर ऐप सेफ है क्या [url=https://www.aviator63791.help]https://www.aviator63791.help[/url]
mostbet_dioa –
mostbet free spins [url=https://mostbet63247.help/]https://mostbet63247.help/[/url]
mostbet_zsKn –
мостбет slot bonus [url=http://mostbet13748.help]http://mostbet13748.help[/url]
aviator_mwSl –
aviator predictor कैसे काम करता है [url=https://aviator63791.help]aviator predictor कैसे काम करता है[/url]
mostbet_jnoa –
mostbet esports [url=mostbet63247.help]mostbet esports[/url]
Timothyduaft –
10mg semaglutide dosage chart Advancing Clinical Research in Metabolic Health and Weight Management
mostbet_xesn –
мостбет белый экран [url=http://mostbet64071.help]мостбет белый экран[/url]
melbet_skPa –
мелбет логин [url=melbet41673.help]мелбет логин[/url]
brightcrestcollective –
Easily one of the better explanations I have read on the topic, and a stop at brightcrestcollective pushed it even higher in my mental ranking of useful resources, the kind of site that beats the average not by trying harder but by simply caring more about what it puts out daily which always shows.
mostbet_fpKn –
mostbet кортҳои Тоҷикистон [url=mostbet13748.help]mostbet кортҳои Тоҷикистон[/url]
Brianliste –
tirzepatide https://usobesityscience.org/liraglutide-studies/ can you take rybelsus and phentermine together
mostbet_uwSa –
mostbet yeni link [url=www.mostbet63875.help]mostbet yeni link[/url]
aviator_fqSl –
aviator असली पैसे से खेल [url=http://aviator63791.help/]http://aviator63791.help/[/url]
mostbet_gbSa –
mostbet kartdan çıxarış vaxtı [url=https://mostbet63875.help/]https://mostbet63875.help/[/url]
mostbet_oboa –
mostbet lol [url=https://mostbet63247.help]https://mostbet63247.help[/url]
bloomstreetcorner –
Now setting up a small reminder to revisit the site on a slow day, and a stop at bloomstreetcorner confirmed the reminder was a good idea, planning return visits is a small organisational act that signals trust in ongoing quality and this site has earned that planned return through consistent performance across the pieces I have read so far.
Timothyduaft –
how much is rybelsus cost glp-1 agonists
mostbet_scSa –
mostbet 2fa [url=https://mostbet63875.help]https://mostbet63875.help[/url]
Brianliste –
Advancing Clinical Research in Metabolic Health and Weight Management https://usobesityscience.org/liraglutide-studies/ cheap victoza
mostbet_mpsn –
mostbet lucky jet [url=www.mostbet64071.help]www.mostbet64071.help[/url]
melbet_ytPa –
мелбет рабочее зеркало [url=https://www.melbet41673.help]https://www.melbet41673.help[/url]
mostbet_jhsn –
mostbet верификация [url=https://mostbet64071.help]mostbet верификация[/url]
melbet_dbPa –
мелбет майнс [url=https://www.melbet41673.help]https://www.melbet41673.help[/url]
bestfindsmarket –
However measured this site clears the bar I set for sites I take seriously, and a stop at bestfindsmarket continued clearing that bar, the metrics I use for site quality are admittedly informal but they are consistent and this site has cleared them on multiple measurements across multiple visits which is meaningful for my evaluation.
Timothyduaft –
semaglutide or tirzepatide Advancing Clinical Research in Metabolic Health and Weight Management
melbet_yfPa –
aviator мелбет [url=http://melbet41673.help/]aviator мелбет[/url]
mostbet_zasn –
mostbet повторная отправка кода [url=https://mostbet64071.help]mostbet повторная отправка кода[/url]
bestdealcenter –
Got pulled in by the headline and stayed because the content actually delivered on the promise, and a stop at bestdealcenter kept that trust intact, when a site lives up to its own framing it earns the right to keep showing up in my browser tabs going forward indefinitely from here on out really.
Brianliste –
orlistat https://usobesityscience.org/ side effects rybelsus
aviator_ajsi –
aviator bonus problemi [url=www.aviator57204.help]www.aviator57204.help[/url]
melbet_vrpl –
чӣ тавр аз melbet пул баровардан [url=https://melbet82460.help/]https://melbet82460.help/[/url]
plinko_gtml –
plinko account verification bd [url=plinko90283.help]plinko account verification bd[/url]
believeinyourdreams –
Worth a slow read rather than the fast scan I usually default to, and a look at believeinyourdreams earned the same slower pace from me, content that resets my reading speed downward is content with substance worth absorbing and this site has produced that effect on me multiple times now over the last week here.
aviator_mpKn –
aviator mínimo saque [url=aviator46035.help]aviator46035.help[/url]
Timothyduaft –
buy victoza online tirzepatide
Brianliste –
glp-1 agonists https://usobesityscience.org/ liraglutide
wildsparklestore –
Comfortable in tone and substantive in content, that is a hard combination to land, and a look at wildsparklestore kept that pairing alive across more material, this is what good editorial direction looks like in practice and the team here clearly has someone keeping a steady hand on the wheel across what they decide to publish.
aviator_xcsi –
aviator peşəkar strategiya [url=www.aviator57204.help]www.aviator57204.help[/url]
melbet_xkpl –
melbet app аз сомонаи расмӣ [url=www.melbet82460.help]www.melbet82460.help[/url]
melbet_hrpl –
melbet барориш [url=https://www.melbet82460.help]https://www.melbet82460.help[/url]
aviator_pfsi –
aviator təhlükəsizlik ayarları [url=https://www.aviator57204.help]https://www.aviator57204.help[/url]
Brianliste –
orlistat https://usobesityscience.org/ semaglutide ozempic rash pictures
wildflowerpeak –
Felt no urge to argue with the conclusions even though I started the post slightly skeptical, and a look at wildflowerpeak maintained that pattern, writing that earns agreement through clarity of argument rather than rhetorical pressure is the kind I find most persuasive and the kind I want to read more of these days.
plinko_ljml –
plinko bKash deposit [url=http://plinko90283.help/]http://plinko90283.help/[/url]
plinko_ujml –
plinko mines withdrawal [url=http://plinko90283.help]plinko mines withdrawal[/url]
aviator_hgKn –
aviator baixar app [url=aviator46035.help]aviator46035.help[/url]
aviator_hoKn –
aviator app android [url=https://www.aviator46035.help]aviator app android[/url]
aviator_cpsi –
aviator depozit üçün kart uyğunluğu [url=http://aviator57204.help]http://aviator57204.help[/url]
melbet_vbpl –
melbet plinko 2026 [url=https://www.melbet82460.help]https://www.melbet82460.help[/url]
violetcresttrends –
Reading the writers other posts after this one suggests the quality is consistent rather than peak, and a stop at violetcresttrends confirmed the consistent quality reading, sites that hold the same level across many pieces rather than peaking on a few are sites with sustainable editorial discipline and this one has clearly developed that.
Brianliste –
tirzepatide https://usobesityscience.org/ rybelsus 14 mg para que sirve
mostbet_hwMl –
mostbet fogadás bónusz nélkül [url=https://mostbet26815.help/]https://mostbet26815.help/[/url]
melbet_teKa –
melbet лимиты ставок [url=http://melbet30819.help/]http://melbet30819.help/[/url]
mostbet_ksOa –
мостбет зеркало официальный сайт [url=http://mostbet07541.help]http://mostbet07541.help[/url]
aviator_ckKn –
mines aviator [url=aviator46035.help]mines aviator[/url]
urbanfashionhub –
Took a few notes from this post, the points are easy to remember without needing to come back and check, and a look at urbanfashionhub added a couple more, the kind of place that sticks in the memory long after the browser tab has been closed for the day which says a lot really.
HiramLok –
gabapentin antibiotic interaction Gabapentin gabapentin 100mg capsules side effeccts
urbanchoiceoutlet –
Reading carefully this time rather than scanning, and the depth shows up in places I missed first time around, and a look at urbanchoiceoutlet rewarded the same careful approach, content that holds up to multiple reads is content I want more of in my regular rotation rather than disposable scroll fodder daily.
mostbet_vbMl –
mostbet új fiók [url=http://mostbet26815.help]http://mostbet26815.help[/url]
mostbet_ddOa –
mostbet apk для телефона [url=http://mostbet07541.help]mostbet apk для телефона[/url]
uniquevaluestore –
Worth flagging that this approach to the topic is fresh without being contrarian, and a stop at uniquevaluestore extended the same fresh angle, finding original perspective on familiar subjects is rare and this site has clearly developed its own way of seeing rather than echoing the dominant takes from elsewhere consistently.
mostbet_kmMl –
mostbet idő limit [url=http://mostbet26815.help]mostbet idő limit[/url]
mostbet_htOa –
mostbet создать аккаунт [url=www.mostbet07541.help]www.mostbet07541.help[/url]
HiramLok –
is gabapentin good for sleep nnprc gabapentin 300 mg capsule side effects
mostbet_zyOa –
mostbet официальный сайт мобильная версия [url=http://mostbet07541.help]http://mostbet07541.help[/url]
mostbet_otMl –
mostbet VIP [url=www.mostbet26815.help]mostbet VIP[/url]
HiramLok –
amoxicillin online canada IDARI can i buy amoxicillin over the counter in australia
HiramLok –
ivermectin 6mg ICPS cost of stromectol medication
HiramLok –
can you purchase amoxicillin online cheap amoxicillin 500mg amoxicillin 500 mg without prescription
HiramLok –
can i buy amoxicillin online Infectious Disease & Antimicrobial Research Institute amoxil generic
HiramLok –
buy cheap amoxicillin online Amoxil where to buy amoxicillin over the counter
HiramLok –
ivermectin 10 mg Ivermectin ivermectin 4 tablets price
Octaviowaync –
top 10 online pharmacy in india: Flexi Meds India – legal online pharmacies in the us
Octaviowaync –
Easy North RX: canadian discount pharmacy – Easy North RX
Octaviowaync –
MexiCare Direct: MexiCare Direct – MexiCare Direct
Octaviowaync –
MexiCare Direct: MexiCare Direct – MexiCare Direct
Octaviowaync –
farmacia mexicana en linea: MexiCare Direct – MexiCare Direct
Octaviowaync –
mexican online pharmacy: MexiCare Direct – MexiCare Direct
Octaviowaync –
Easy North RX: Easy North RX – legitimate canadian online pharmacies
plinko_xaml –
plinko bangladesh mirror [url=http://plinko90283.help]http://plinko90283.help[/url]
Octaviowaync –
pharmacy mexico online: online pharmacy – online pharmacy in mexico
melbet_jhmi –
мелбет как вывести на элсом [url=https://www.melbet31507.help]https://www.melbet31507.help[/url]
aviator_fiOn –
aviator Bangladesh promo code [url=https://aviator73841.help/]aviator Bangladesh promo code[/url]
aviator_gomn –
aviator Mzuzu [url=https://aviator13854.help/]https://aviator13854.help/[/url]
melbet_ytkn –
мелбет скачать android [url=http://melbet96841.help]http://melbet96841.help[/url]
mostbet_alPl –
mostbet игровые автоматы [url=http://mostbet80395.help]http://mostbet80395.help[/url]
melbet_jgKa –
мелбет android не открывается [url=https://melbet30819.help/]https://melbet30819.help/[/url]
Octaviowaync –
indian pharmacy online: Flexi Meds India – legitimate online pharmacy
melbet_mdKa –
как отыграть бонус melbet [url=www.melbet30819.help]www.melbet30819.help[/url]
melbet_idKa –
мелбет ставки на футбол [url=www.melbet30819.help]www.melbet30819.help[/url]
Octaviowaync –
reliable canadian pharmacy reviews: canadapharmacyonline com – Easy North RX
melbet_qami –
мелбет crash [url=https://melbet31507.help]мелбет crash[/url]
aviator_orOn –
aviator customer support chat [url=http://aviator73841.help/]http://aviator73841.help/[/url]
melbet_mlmi –
мелбет mines [url=https://melbet31507.help/]https://melbet31507.help/[/url]
melbet_pykn –
мелбет crash играть [url=melbet96841.help]melbet96841.help[/url]
aviator_kmmn –
aviator mines android [url=https://aviator13854.help]https://aviator13854.help[/url]
aviator_xwOn –
aviator game link bd [url=https://aviator73841.help]https://aviator73841.help[/url]
mostbet_kyPl –
мостбет вывести деньги Кыргызстан [url=https://mostbet80395.help]https://mostbet80395.help[/url]
melbet_oikn –
melbet бк регистрация [url=http://melbet96841.help/]melbet бк регистрация[/url]
aviator_gjmn –
aviator best betting site malawi aviator [url=http://aviator13854.help]http://aviator13854.help[/url]
mostbet_skPl –
мостбет скачать сегодня [url=mostbet80395.help]mostbet80395.help[/url]
melbet_ommi –
melbet скачать бк кыргызстан [url=https://www.melbet31507.help]https://www.melbet31507.help[/url]
mostbet_khsr –
mostbet jak použít promo kód [url=http://mostbet75409.help]http://mostbet75409.help[/url]
aviator_ptOn –
aviator bonus terms bd [url=http://aviator73841.help/]http://aviator73841.help/[/url]
Octaviowaync –
Easy North RX: online pharmacy canada – Easy North RX
aviator_iymn –
aviator telegram support [url=http://aviator13854.help]aviator telegram support[/url]
mostbet_bdPl –
mostbet aviator [url=https://mostbet80395.help]https://mostbet80395.help[/url]
Octaviowaync –
indian pharmacies safe: Flexi Meds India – best online pharmacy no prescription
mostbet_nmsr –
mostbet limity crypto [url=http://mostbet75409.help/]http://mostbet75409.help/[/url]
mostbet_bhsr –
mostbet v Česku [url=mostbet75409.help]mostbet75409.help[/url]
melbet_fzkn –
мелбет слоты [url=http://melbet96841.help/]мелбет слоты[/url]
Octaviowaync –
п»їlegitimate online pharmacies india: indian pharmacy paypal – express scripts mail order pharmacy
mostbet_iwsr –
mostbet přístup přes zrcadlo [url=https://mostbet75409.help/]https://mostbet75409.help/[/url]
mostbet_wiol –
most bet [url=https://mostbet72483.help]https://mostbet72483.help[/url]
melbet_mfEi –
melbet зеркало ош [url=https://www.melbet42570.help]melbet зеркало ош[/url]
mostbet_csMn –
mostbet descarcare din site oficial [url=https://mostbet19438.help]mostbet descarcare din site oficial[/url]
Octaviowaync –
Easy North RX: canadian pharmacies shipping to usa – Easy North RX
mostbet_puol –
mostbet Azərbaycan aktual mirror [url=http://mostbet72483.help]http://mostbet72483.help[/url]
mostbet_miol –
mostbet profil [url=https://mostbet72483.help/]https://mostbet72483.help/[/url]
Octaviowaync –
ed meds online canada: vipps canadian pharmacy – Easy North RX
melbet_vzEi –
мелбет слоты киргизия [url=https://melbet42570.help]https://melbet42570.help[/url]
melbet_shEi –
melbet плинко [url=melbet42570.help]melbet плинко[/url]
mostbet_gyol –
mostbet visa depozit [url=https://mostbet72483.help]mostbet visa depozit[/url]
mostbet_piMn –
mostbet inchidere cont [url=mostbet19438.help]mostbet19438.help[/url]
mostbet_orMn –
mostbet mastercard Moldova [url=http://mostbet19438.help]http://mostbet19438.help[/url]
melbet_puEi –
мелбет бонус за регистрацию [url=https://www.melbet42570.help]https://www.melbet42570.help[/url]
mostbet_zdEi –
mostbet bonus do crash [url=https://mostbet14793.help]https://mostbet14793.help[/url]
Octaviowaync –
indianpharmacy com: mail order pharmacy india – online pharmacy
mostbet_gpMn –
mostbet bonus pariuri sportive [url=https://www.mostbet19438.help]https://www.mostbet19438.help[/url]
Octaviowaync –
Easy North RX: Easy North RX – vipps canadian pharmacy
mostbet_gsEi –
mostbet turniej aviator [url=mostbet14793.help]mostbet turniej aviator[/url]
melbet_myka –
melbet vip program [url=https://melbet67541.help]https://melbet67541.help[/url]
mostbet_agEi –
mostbet odblokowanie po weryfikacji [url=http://mostbet14793.help]http://mostbet14793.help[/url]
Octaviowaync –
Online medicine order: Flexi Meds India – legal online pharmacies in the us
mostbet_vzea –
как пополнить мостбет [url=https://mostbet71530.help]https://mostbet71530.help[/url]
mostbet_kvEi –
mostbet depozyt na zakłady [url=https://mostbet14793.help]https://mostbet14793.help[/url]
vavada_fspl –
vavada prijava hrvatska [url=http://vavada25076.help]vavada prijava hrvatska[/url]
vavada_sdkl –
vavada strategie plinko [url=http://vavada82614.help]http://vavada82614.help[/url]
Octaviowaync –
top 10 pharmacies in india: top online pharmacy india – worldwide pharmacy
melbet_bqka –
melbet transaction fee [url=melbet67541.help]melbet67541.help[/url]
melbet_ulka –
melbet bd bonus code [url=https://www.melbet67541.help]https://www.melbet67541.help[/url]
mostbet_duea –
mostbet сброс пароля [url=http://mostbet71530.help/]http://mostbet71530.help/[/url]
vavada_tdkl –
vavada aviator na telefon [url=https://vavada82614.help]https://vavada82614.help[/url]
vavada_nqpl –
vavada kasino aplikacija ios [url=www.vavada25076.help]www.vavada25076.help[/url]
melbet_jaka –
melbet app problem [url=https://melbet67541.help]https://melbet67541.help[/url]
vavada_sjpl –
vavada metode isplate hrvatska [url=www.vavada25076.help]www.vavada25076.help[/url]
vavada_wtkl –
vavada aplikacja bukmacher [url=http://vavada82614.help/]http://vavada82614.help/[/url]
Octaviowaync –
Easy North RX: canadian pharmacies shipping to usa – legitimate canadian pharmacies
vavada_srpl –
kako isplatiti novac s vavada [url=https://www.vavada25076.help]https://www.vavada25076.help[/url]
vavada_yskl –
vavada potwierdzenie konta [url=https://vavada82614.help/]https://vavada82614.help/[/url]
aviator_ocmi –
aviator reviews Malawi [url=http://aviator29471.help/]aviator reviews Malawi[/url]
mostbet_ahsn –
mostbet plinko [url=http://mostbet35906.help]http://mostbet35906.help[/url]
Octaviowaync –
world pharmacy india: mail order pharmacy india – online pharmacy no rx
Octaviowaync –
MexiCare Direct: MexiCare Direct – MexiCare Direct
shkola onlain_xeOn –
онлайн школа для детей [url=https://shkola-onlajn-51.ru]https://shkola-onlajn-51.ru[/url]
shkola onlain_woPl –
онлайн-школа для детей [url=https://shkola-onlajn-52.ru]онлайн-школа для детей[/url]
aviator_yymi –
aviator mw site [url=https://www.aviator29471.help]https://www.aviator29471.help[/url]
vivod iz zapoya na domy_hnKt –
вывод из запоя нарколог24 [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-18.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-18.ru[/url]
mostbet_kgea –
mostbet как вывести через click [url=www.mostbet71530.help]www.mostbet71530.help[/url]
vivod iz zapoya na domy_dmei –
вывод из запоя на дому спб [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-20.ru]вывод из запоя на дому спб[/url]
Kak naiti cheloveka po nomery telefona_xoKn –
найти человека по номеру телефона бесплатно через спутник [url=www.kak-najti-cheloveka-po-nomeru-telefona-1.ru]www.kak-najti-cheloveka-po-nomeru-telefona-1.ru[/url]
aviator_ydmi –
aviator mw apk [url=http://aviator29471.help]aviator mw apk[/url]
mostbet_xpsn –
mostbet pasport [url=https://mostbet35906.help/]https://mostbet35906.help/[/url]
pereplanirovka kvartir_chmn –
согласование перепланировки [url=http://www.pereplanirovka-kvartir19.ru]согласование перепланировки[/url]
mostbet_nvsn –
mostbet çıxarış gecikir [url=mostbet35906.help]mostbet35906.help[/url]
mostbet_haea –
мостбет уз [url=http://mostbet71530.help]http://mostbet71530.help[/url]
Octaviowaync –
MexiCare Direct: farmacia mexicana en linea – MexiCare Direct
aviator_qhmi –
how to deposit money on aviator in malawi [url=http://aviator29471.help/]http://aviator29471.help/[/url]
mostbet_cjsn –
mostbet paşa bank [url=https://mostbet35906.help/]https://mostbet35906.help/[/url]
mostbet_trPl –
мостбет скачать бесплатно [url=https://mostbet58127.help]мостбет скачать бесплатно[/url]
mostbet_lsKa –
mostbet apk [url=http://mostbet90518.help]mostbet apk[/url]
vivod iz zapoya na domy_ujei –
вывод из запоя нарколог24 [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-20.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-20.ru[/url]
shkola onlain_qmPl –
образовательные онлайн школы [url=https://shkola-onlajn-52.ru]образовательные онлайн школы[/url]
shkola onlain_inOn –
lbs что это [url=https://shkola-onlajn-51.ru]https://shkola-onlajn-51.ru[/url]
vivod iz zapoya na domy_iiKt –
вывести из запоя цена [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-18.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-18.ru[/url]
Octaviowaync –
india pharmacy: india pharmacy mail order – pharmacy no prescription required
Kak naiti cheloveka po nomery telefona_lnKn –
найти по номеру телефона где находится человек [url=http://www.kak-najti-cheloveka-po-nomeru-telefona-1.ru]http://www.kak-najti-cheloveka-po-nomeru-telefona-1.ru[/url]
pereplanirovka kvartir_kjmn –
согласование перепланировки квартиры в москве [url=http://www.pereplanirovka-kvartir19.ru]http://www.pereplanirovka-kvartir19.ru[/url]
Octaviowaync –
indian pharmacy paypal: Flexi Meds India – reliable online pharmacy
mostbet_czPl –
мостбет официальный сайт Киргизия [url=http://mostbet58127.help]http://mostbet58127.help[/url]
mostbet_uwKa –
mostbet bilet sistem [url=http://mostbet90518.help/]mostbet bilet sistem[/url]
mostbet_qpPl –
mostbet зеркало [url=www.mostbet58127.help]mostbet зеркало[/url]
mostbet_anKa –
mostbet bonusuri Moldova [url=mostbet90518.help]mostbet90518.help[/url]
vivod iz zapoya na domy_wpei –
вывод из запоя нарколог24 [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-20.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-20.ru[/url]
shkola onlain_viPl –
онлайн обучение школа [url=https://shkola-onlajn-52.ru]https://shkola-onlajn-52.ru[/url]
vivod iz zapoya na domy_vcKt –
вывод из запоя цена [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-18.ru]вывод из запоя цена[/url]
Kak naiti cheloveka po nomery telefona_viKn –
как посмотреть где находится человек по номеру телефона [url=http://kak-najti-cheloveka-po-nomeru-telefona-1.ru]http://kak-najti-cheloveka-po-nomeru-telefona-1.ru[/url]
Octaviowaync –
canada rx pharmacy: canadian pharmacy review – Easy North RX
mostbet_qePl –
mostbet официальный сайт рабочий [url=mostbet58127.help]mostbet58127.help[/url]
mostbet_uyKa –
mostbet transfer bancar Moldova [url=www.mostbet90518.help]www.mostbet90518.help[/url]
vivod iz zapoya na domy_zwei –
капельница от алкоголя на дому спб [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-20.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-20.ru[/url]
pereplanirovka kvartir_kjmn –
перепланировка москва [url=pereplanirovka-kvartir19.ru]pereplanirovka-kvartir19.ru[/url]
shkola onlain_hdPl –
онлайн-школа для детей [url=https://shkola-onlajn-52.ru]онлайн-школа для детей[/url]
Octaviowaync –
Easy North RX: best canadian online pharmacy – Easy North RX
vivod iz zapoya na domy_xmKt –
врач капельница алкоголь на дом [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-18.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-18.ru[/url]
Kak naiti cheloveka po nomery telefona_rdka –
слежка по номеру телефона [url=https://www.kak-najti-cheloveka-po-nomeru-telefona-2.ru]https://www.kak-najti-cheloveka-po-nomeru-telefona-2.ru[/url]
Octaviowaync –
online pharmacy india: indian pharmacies safe – online pharmacy no prescription needed
Kak naiti cheloveka po nomery telefona_evKn –
как узнать местоположение человека по номеру телефона [url=https://www.kak-najti-cheloveka-po-nomeru-telefona-1.ru]https://www.kak-najti-cheloveka-po-nomeru-telefona-1.ru[/url]
mostbet_qtPr –
mostbet приложение Киргизия [url=http://mostbet45018.help]http://mostbet45018.help[/url]
mostbet_cnSt –
mostbet güzgü saytı giriş [url=http://mostbet45039.help]http://mostbet45039.help[/url]
pereplanirovka kvartir_ewmn –
перепланировка услуги [url=http://pereplanirovka-kvartir19.ru]перепланировка услуги[/url]
shkola onlain_agOn –
лбс это [url=https://shkola-onlajn-51.ru]https://shkola-onlajn-51.ru[/url]
mostbet_nnsn –
mostbet-kg [url=https://mostbet17893.online/]mostbet-kg[/url]
melbet_hoOi –
melbet пополнение элкарт [url=http://melbet62894.help]http://melbet62894.help[/url]
pinup_tker –
pin-up móvil [url=pinup90362.help]pinup90362.help[/url]
Octaviowaync –
mail order pharmacy india: Flexi Meds India – no prescription pharmacy paypal
Kevindok –
Steam Desktop Authenticator https://sdasteam.com (SDA). It allows you to generate account login codes and automatically confirm trades or item sales on the Community Market without using your smartphone.
Kak naiti cheloveka po nomery telefona_laka –
определить местоположение по номеру телефона [url=https://www.kak-najti-cheloveka-po-nomeru-telefona-2.ru]определить местоположение по номеру телефона[/url]
Octaviowaync –
top online pharmacy india: Flexi Meds India – pharmacy no prescription required
Octaviowaync –
reputable indian online pharmacy: п»їlegitimate online pharmacies india – legit online pharmacy
shkola onlain_cuOn –
11 класс онлайн [url=https://shkola-onlajn-51.ru]https://shkola-onlajn-51.ru[/url]
Octaviowaync –
escrow pharmacy canada: canadian pharmacy 24 com – canada rx pharmacy
Octaviowaync –
MexiCare Direct: MexiCare Direct – mexican pharmacies online
Octaviowaync –
best mexican pharmacy: MexiCare Direct – mexican pharma
Octaviowaync –
Online medicine order: india pharmacy – medicine online order
Octaviowaync –
Easy North RX: canadian online drugs – pharmacy rx world canada
Octaviowaync –
buy prescription drugs from india: buy prescription drugs from india – international pharmacy
Octaviowaync –
Easy North RX: Easy North RX – Easy North RX
Octaviowaync –
mexican medicine store: MexiCare Direct – MexiCare Direct
Kak naiti cheloveka po nomery telefona_uyka –
как найти телефон по номеру [url=kak-najti-cheloveka-po-nomeru-telefona-2.ru]как найти телефон по номеру[/url]
Octaviowaync –
MexiCare Direct: MexiCare Direct – MexiCare Direct
Octaviowaync –
the canadian drugstore: canadian pharmacies shipping to usa – canada drugs online
Octaviowaync –
Easy North RX: cheapest pharmacy canada – escrow pharmacy canada
kapelnica ot pohmelya_gbKn –
капельница на дому недорого [url=https://kapelnicza-ot-pokhmelya-samara-39.ru]https://kapelnicza-ot-pokhmelya-samara-39.ru[/url]
Octaviowaync –
india online pharmacy: Flexi Meds India – trusted online pharmacy
JamesPaups –
https://mexicaredirect.com/# pharmacies in mexico that ship to the us
Randymek –
https://mexicaredirect.shop/# online pharmacy
Octaviowaync –
best india pharmacy: Flexi Meds India – no rx needed pharmacy
Narkolog na dom_qjMi –
наркологическая служба на дом [url=https://narkolog-na-dom-moskva-27.ru]наркологическая служба на дом[/url]
Octaviowaync –
Easy North RX: Easy North RX – precription drugs from canada
Randymek –
https://fleximedsindia.com/# indian pharmacy
kapelnica ot pohmelya_avKn –
капельница от запоя недорого [url=https://kapelnicza-ot-pokhmelya-samara-39.ru]https://kapelnicza-ot-pokhmelya-samara-39.ru[/url]
Danielcab –
oral semaglutide treatment [url=https://dailybalancepharmacy.shop/#]semaglutide tablets online[/url] rybelsus semaglutide tablets
Jamesget –
neurontin gabapentin capsules: neurontin gabapentin capsules – gabapentin daily therapy
WilliamjaR –
http://metaboliccarepharmacy.com/# MetabolicCare Pharmacy
GeorgeTal –
http://neuropathpharmacys.com/# neuropathic symptom support
Kak naiti cheloveka po nomery telefona_hnka –
отследить номер телефона бесплатно [url=http://www.kak-najti-cheloveka-po-nomeru-telefona-2.ru]http://www.kak-najti-cheloveka-po-nomeru-telefona-2.ru[/url]
Jamesget –
ozempic best price: ozempic generic – reputable overseas online pharmacies
luxury car rental miami_rbst –
luxury auto rental [url=luxury-car-rental-miami-1.com]luxury auto rental[/url]
WilliamjaR –
https://metaboliccarepharmacy.shop/# MetabolicCarePharmacy
kapelnica ot pohmelya_woet –
капельница от запоя цена [url=https://kapelnicza-ot-pokhmelya-samara-38.ru]капельница от запоя цена[/url]
kapelnica ot pohmelya_ujKn –
прокапаться от алкоголя цены [url=https://kapelnicza-ot-pokhmelya-samara-39.ru]прокапаться от алкоголя цены[/url]
Danielcab –
ozempic generic [url=https://metaboliccarepharmacy.com/#]ozempic cost without insurance[/url] legitimate online pharmacy
Jamesget –
neuropathic symptom support: gabapentin daily therapy – NeuroPath Pharmacy
WilliamjaR –
http://metaboliccarepharmacy.com/# buy generic ozempic
luxury car rental miami_tlst –
exotic car rental miami beach prices [url=http://luxury-car-rental-miami-1.com]http://luxury-car-rental-miami-1.com[/url]
GeorgeTal –
http://metaboliccarepharmacy.com/# MetabolicCare Pharmacy
kapelnica ot pohmelya_mbKt –
капельница после запоя цена [url=https://kapelnicza-ot-pokhmelya-samara-40.ru]капельница после запоя цена[/url]
Jamesget –
ozempic online: ozempic coupon – legal online pharmacies in the us
tkan dlya mebeli_ixPt –
купить материал для обивки дивана [url=https://tkan-dlya-mebeli.ru]https://tkan-dlya-mebeli.ru[/url]
vivod iz zapoya v stacionare_aoEn –
выведение из запоя в наркологическом стационаре [url=https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-27.ru]выведение из запоя в наркологическом стационаре[/url]
Franklic –
https://neuropathpharmacys.shop/# neuropathic symptom support
Jamesget –
DailyBalance Pharmacy: rybelsus vs victoza – DailyBalancePharmacy
melbet_bnmi –
скачать melbet на андроид [url=https://elenagatilova.ru]скачать melbet на андроид[/url]
Danielcab –
NeuroPathPharmacy [url=https://neuropathpharmacys.com/#]NeuroPath[/url] neurontin gabapentin capsules
Jamesget –
semaglutide injection pen: MetabolicCare – online drugs order
syvenirnaya prodykciya s logotipom_igkl –
рекламно сувенирная продукция [url=https://suvenirnaya-produkcziya-s-logotipom-8.ru]https://suvenirnaya-produkcziya-s-logotipom-8.ru[/url]
Franklic –
https://neuropathpharmacys.shop/# neurontin gabapentin capsules
Jamesget –
NeuroPath: neuropathic pain medication – NeuroPath Pharmacy
melbet_smei –
мелбет казино скачать [url=https://tcso-begovoy.ru]мелбет казино скачать[/url]
Jamesget –
glp-1 tablet medication: DailyBalance Pharmacy – oral semaglutide treatment
Danielcab –
semaglutide daily dosing [url=https://dailybalancepharmacy.com/#]DailyBalance Pharmacy[/url] DailyBalance
Franklic –
http://neuropathpharmacys.com/# neuropathic pain medication
Jamescoche –
Viagra Pfizer sans ordonnance: SildГ©nafil Teva 100 mg acheter – SildГ©nafil 100 mg sans ordonnance
Narkolog na dom_mbMi –
врач нарколог анонимно [url=https://narkolog-na-dom-moskva-27.ru]врач нарколог анонимно[/url]
Jamescoche –
reliable rx pharmacy: mexico online farmacia – mexican pharmacy las vegas
Narkolog na dom_nuPn –
срочный вывод из запоя на дому врач [url=https://narkolog-na-dom-moskva-28.ru]срочный вывод из запоя на дому врач[/url]
FrancisWab –
hur stavas medicin [url=http://svenskapharm.com/#]halsont apotek[/url] pildora del dia despues apotek
Jamescoche –
mexican pharmacies that ship: mexico online farmacia – mexico pet pharmacy
Kak naiti cheloveka po nomery telefona_kvka –
как найти телефон по номеру [url=www.kak-najti-cheloveka-po-nomeru-telefona-2.ru]как найти телефон по номеру[/url]
Jamescoche –
mexican farmacia: mexican pharmacys – farmacia mexicana en chicago
Narkolog na dom_mwMi –
Всем доброго времени суток. Тема здоровья всегда на первом месте, потому что в экстренной ситуации трудно сориентироваться. Если срочно требуется квалифицированный нарколог на дом в Москве, лучше сразу обращаться к сертифицированным медикам.
Знакомые вызывали бригаду в похожей ситуации и в итоге нашли клинику, где врачи работают профессионально. Если вам актуально или ситуация экстренная, можете ознакомиться по ссылке: [url=https://narkolog-na-dom-moskva-27.ru/]услуги нарколога на дому[/url].
На этом сайте действительно дана полная информация, реагируют очень быстро, буквально за час. Не теряйте время, и обращайтесь к настоящим профессионалам. Пусть все будет хорошо!
FrancisWab –
п»їViagra sans ordonnance 24h [url=https://www.montaigne-capital.com/#]Viagra 100mg prix[/url] Prix du Viagra en pharmacie en France
Jamescoche –
Svenska Pharma: apoteks – Svenska Pharma
Narkolog na dom_wcPn –
наркологическая помощь на дому [url=https://narkolog-na-dom-moskva-28.ru]наркологическая помощь на дому[/url]
ThomasSag –
mexican medicine store: mexico prescription online – online pharmacy in mexico
melbet_pqsn –
Если интересует эта тема, вот толковый разбор. Многие спрашивали, в итоге скачал отсюда: [url=https://teobit.ru]мелбет скачать приложение[/url].
Сам сервис предлагает отличные условия для игроков, все интуитивно понятно даже новичку. Плюс ко всему можно ставить прямо в режиме реального времени.
Если только заводите аккаунт капает бонус на баланс, рекомендую воспользоваться. Всем удачи!
Jamescoche –
order meds from mexico: purple pharmacy mexico – medication in mexico
ThomasSag –
pharmacy in mexico that ships to us: farmacia mexicana en chicago – online pharmacies
Jamescoche –
Svenska Pharma: fГ¶rstoppning feber – Svenska Pharma
Kak_btot –
Чтобы быстро и эффективно [url=https://kak-najti-cheloveka-po-nomeru-telefona-3.ru]отследить телефон по номеру[/url], воспользуйтесь такими штуками которые дают инфу.
Слушай, тут главное — без глупостей.
Поиск человека по номеру телефона возможен при помощи законных методов.
Надеюсь, понятно объяснил.
Narkolog na dom_nsPn –
платный нарколог на дом анонимно [url=https://narkolog-na-dom-moskva-28.ru]платный нарколог на дом анонимно[/url]
Jamescoche –
Viagra sans ordonnance livraison 24h: Viagra pas cher livraison rapide france – Viagra sans ordonnance 24h Amazon
ThomasSag –
mexican online pharmacy: mexico medicine – meds from mexico
mostbet_mkPr –
mostbet как вывести на кошелек [url=http://mostbet45018.help]http://mostbet45018.help[/url]
mostbet_csPr –
mostbet mines стратегия [url=https://www.mostbet45018.help]mostbet mines стратегия[/url]
Jamescoche –
Acheter viagra en ligne livraison 24h: Viagra 100mg prix – Viagra prix pharmacie paris
mostbet_arSt –
mostbet plinko oyun [url=mostbet45039.help]mostbet plinko oyun[/url]
shkola onlain_hpKi –
Давно хотел найти толковое место, где реально дают живые знания. Особенно когда речь про образовательные онлайн школы — тут ведь важен подход. У меня племянник как раз искал гибкий график, так что пришлось перебрать кучу вариантов. В общем, можете глянуть сами: лбс это [url=https://shkola-onlajn-55.ru]https://shkola-onlajn-55.ru[/url] Я если честно ещё пару месяцев назад вообще относился скептически к таким форматам. Оказалось — всё гораздо лучше. У них и программа грамотная. Доволен как слон, если честно. Удачи!
mostbet_oiSt –
mostbet slot bonusu [url=mostbet45039.help]mostbet45039.help[/url]
mostbet_jasn –
mostbet сменить номер [url=http://mostbet17893.online]http://mostbet17893.online[/url]
mostbet_iysn –
мостбет войти [url=http://mostbet17893.online/]http://mostbet17893.online/[/url]
mostbet_ypPr –
мостбет купон экспресс [url=www.mostbet45018.help]www.mostbet45018.help[/url]
pinup_mger –
pin-up apk Chile android [url=www.pinup90362.help]pin-up apk Chile android[/url]
melbet_chOi –
melbet вход в личный кабинет [url=https://melbet62894.help]https://melbet62894.help[/url]
shkola_bxOr –
Я изначально скептически относился ко всей этой дистанционке. Думал, сын просто будет играть в танчики. Но жена настояла, нашли один портал с живыми учителями: [url=https://shkola-onlajn-53.ru]источник[/url] . Фишка в том, что можно спокойно закрыть программу без нервов и репетиторов по вечерам. Техподдержка отвечает быстро. Платформа не виснет на вебинарах, что для меня было критично. Короче, кому надоело возить чадо через весь город под дождем – заглядывайте.
melbet_rhOi –
melbet cashback [url=http://melbet62894.help/]http://melbet62894.help/[/url]
pinup_eser –
pin-up registro Chile rut [url=http://pinup90362.help]http://pinup90362.help[/url]
mostbet_grSt –
mostbet tennis canlı mərc [url=https://mostbet45039.help]mostbet tennis canlı mərc[/url]
Jamescoche –
sjukhuset apotek: godis hemleverans samma dag – Svenska Pharma
ThomasSag –
mexican pharmacies: mexico meds – buy drugs online
pinup_oder –
descargar pin-up apk [url=https://pinup90362.help]descargar pin-up apk[/url]
melbet_deOi –
мелбет быстрый вход [url=https://melbet62894.help]https://melbet62894.help[/url]
mostbet_hesn –
мостбет быстрые платежи [url=http://mostbet17893.online]http://mostbet17893.online[/url]
Jamescoche –
Svenska Pharma: omeprazol kГ¶pa – apotek nГ¤t
shkola onlain_vgEn –
Я в шоке от количества предложений в последнее время, но после изучения реальных отзывов наткнулся на один нормальный человеческий вариант. Если кратко, вот что я понял: современная онлайн-школа для детей — это уровень на порядок выше обычного. Там и преподаватели живые и вовлеченные, что очень радует на практике.
В общем, кому реально нужно нормальное обучение в теме онлайн образование школа — убедитесь во всём сами, вот здесь все выложено без лишней воды: школа онлайн [url=https://shkola-onlajn-54.ru]школа онлайн[/url].
Думаю, это как раз то, что сейчас нужно многим родителям. Потому что обычная школа часто проигрывает по всем фронтам, а тут организована именно живое регулярное общение с кураторами. Советую не тянуть и сразу изучить тему.
ThomasSag –
pharmacy mexico online: mexican pharmacies that ship to us – mexican online mail order pharmacy
vivod iz zapoya v stacionare_ucOa –
Приветствую всех участников. Слушайте, вопрос сложный, но многим может помочь, так как в сети сейчас полно сомнительных клиник. Когда нужен проверенный и опытный врач для капельницы, то не рискуйте и не доверяйте случайным объявлениям.
Мы в свое время тоже столкнулись с этой бедой, в итоге вся ценная информация была собрана по крупицам. Кому тоже нужны подробности и условия, вся информация есть здесь: выведение из запоя в стационаре наркологии [url=https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-28.ru]выведение из запоя в стационаре наркологии[/url].
На этом ресурсе действительно дана полная информация, реагируют очень быстро, буквально за час. Главное — не затягивать в такие моменты, поможет вовремя принять правильные меры. Пусть все будет хорошо!
GregoryLip –
BlueLine Pharmacy: BlueLine Pharmacy – BlueLine
AndrewCloxy –
LifeFlow: LifeFlow Pharmacy – LifeFlow
Narkolog na dom_bfPn –
вывод из запоя с выездом на дом [url=https://narkolog-na-dom-moskva-28.ru]вывод из запоя с выездом на дом[/url]
GregoryLip –
cheapest cenforce: Purchase Cenforce Online – order cenforce
syvenirnaya prodykciya s logotipom_mpoa –
Коллеги, всем привет! Срочно нужна консультация тех, кто уже заказывал мерч для бизнеса. Посоветуйте нормальное изготовление корпоративных сувениров — чтобы и кружки не облазили, и ручки писали. сувенирная продукция [url=https://suvenirnaya-produkcziya-s-logotipom-11.ru]сувенирная продукция[/url] Кто недавно брал подарки с логотипом под новогодние корпоративы, поделитесь контактами. Может, есть проверенные фабрики, которые работают напрямую, без посредников. А то маркетинговые агентства такой ценник лупят — закачаешься.
tkan dlya mebeli_ouEn –
Ребята, выручайте! Купил кресло б/у, каркас норм, но ткань в ужасном состоянии. Ищу, где можно ткань для обивки мебели купить не по космическим ценам. купить ткань для перетяжки дивана [url=https://tkan-dlya-mebeli-1.ru]https://tkan-dlya-mebeli-1.ru[/url] Говорят, флок и микровелюр быстро вытираются, а рогожка лучше. Нужен метров 15-20, может, кто знает нормального поставщика.
melbet_xrol –
Слушайте, наконец-то наткнулся на реальный опыт. Там всё разложено по полочкам, без лишней воды и тупых SEO-текстов. Многие на форумах спорят, а ответ лежал на поверхности. Вот скачать мелбет казино на андроид [url=https://howtoairbrush.com]скачать мелбет казино на андроид[/url] — советую изучить на досуге. Мне лично это сэкономило кучу времени и нервов, так что делюсь от души.
GregoryLip –
BlueLine Pharmacy: sildenafil online – Buy Viagra online cheap
Kak naiti cheloveka po nomery telefona_gama –
Уже отчаялся был найти хоть что-то стоящее. Ситуация дурацкая, потерял контакт со старым хорошим другом. Решил докопаться до истины и разобраться,. И знаете что? Оказывается, сейчас есть реальные способы.
Короче, если вас сейчас волнует тот же самый вопрос — как вычислить анонимного абонента, то есть один проверенный временем вариант. Конкретно про то, как найти человека по номеру телефона — вот здесь всё максимально норм расписано: пробить человека по номеру онлайн [url=https://kak-najti-cheloveka-po-nomeru-telefona-4.ru]пробить человека по номеру онлайн[/url].
Я сам сначала вообще не верил во всё это. Потому что а тут выложена конкретная и структурированная информация. В общем, кому надо — тот точно воспользуется. Надеюсь, кому-то тоже упростит жизнь.
syvenirnaya prodykciya s logotipom_quoa –
Коллеги, всем привет! Срочно нужна консультация тех, кто уже заказывал мерч для бизнеса. Интересует надежный поставщик корпоративных подарков с логотипом компании, который не подведет со сроками. сувениры с логотипом компании [url=https://suvenirnaya-produkcziya-s-logotipom-11.ru]сувениры с логотипом компании[/url] Реально ли найти недорогую сувенирную продукцию с логотипом с печатью от 100 штук. Может, есть проверенные фабрики, которые работают напрямую, без посредников. Киньте ссылки или названия компаний, буду очень благодарен.
mostbet_duEi –
mostbet login cz [url=https://mostbet06318.help/]https://mostbet06318.help/[/url]
mostbet_rrsi –
mostbet awaria [url=https://mostbet26540.help]https://mostbet26540.help[/url]
melbet_lbOi –
melbet элкарт вывод [url=http://melbet62894.help/]melbet элкарт вывод[/url]
mostbet_eapn –
мостбет мобильная версия [url=http://mostbet15743.help]http://mostbet15743.help[/url]
GregoryLip –
LifeFlow: LifeFlow Pharmacy – LifeFlow
melbet_umMr –
мелбет ошибка вывода [url=http://melbet78240.help]http://melbet78240.help[/url]
AndrewCloxy –
cheap ed medicine: ChoiceRx Pharmacy – low cost ed medication
GregoryLip –
ed meds by mail: cheap boner pills – cheap ed pills online
syvenirnaya prodykciya s logotipom_reoa –
Коллеги, всем привет! Встала задача обновить ассортимент брендированной атрибуки для отдела продаж. Подскажите, где заказать качественную сувенирную продукцию с логотипом. товары с логотипом компании [url=https://suvenirnaya-produkcziya-s-logotipom-11.ru]https://suvenirnaya-produkcziya-s-logotipom-11.ru[/url] Реально ли найти недорогую сувенирную продукцию с логотипом с печатью от 100 штук. Может, есть проверенные фабрики, которые работают напрямую, без посредников. Киньте ссылки или названия компаний, буду очень благодарен.
shkola onlain_neEn –
Честно говоря, долго выбирал, куда поступать, но после советов хороших знакомых наткнулся на один нормальный человеческий вариант. Если кратко, вот что я понял: современная школа онлайн — это серьёзный и комплексный подход. Там и преподаватели живые и вовлеченные, что очень радует на практике.
В общем, кому реально нужно нормальное обучение в теме онлайн образование школа — посмотрите условия, вот здесь все разжевано до мелочей: lbs [url=https://shkola-onlajn-54.ru]lbs[/url].
Думаю, это как раз то, что сейчас нужно многим родителям. Потому что без четкой системы в обучении сейчас вообще никуда, а тут организована именно частная школа онлайн. Пригодится точно, потом еще спасибо скажете.
tkan dlya mebeli_wlEn –
Ребята, выручайте! Купил кресло б/у, каркас норм, но ткань в ужасном состоянии. Посоветуйте нормальную мебельную ткань для частого использования. обивочные ткани для мебели [url=https://tkan-dlya-mebeli-1.ru]https://tkan-dlya-mebeli-1.ru[/url] Говорят, флок и микровелюр быстро вытираются, а рогожка лучше. Нужен метров 15-20, может, кто знает нормального поставщика.
mostbet_xtEi –
mostbet reload bonus [url=mostbet06318.help]mostbet06318.help[/url]
mostbet_tysi –
mostbet cofnięcie wypłaty [url=https://mostbet26540.help]https://mostbet26540.help[/url]
mostbet_vxpn –
мостбет актуальное зеркало [url=https://mostbet15743.help]https://mostbet15743.help[/url]
melbet_ujOi –
мелбет официальный адрес [url=www.melbet62894.help]мелбет официальный адрес[/url]
GregoryLip –
Cheap Levitra online: Levitra 20 mg for sale – Buy Vardenafil 20mg online
mostbet_kxEi –
mostbet bonus 2026 [url=mostbet06318.help]mostbet06318.help[/url]
mostbet_opsi –
mostbet wypłata [url=http://mostbet26540.help/]http://mostbet26540.help/[/url]
melbet_wjOi –
мелбет зеркало ош [url=http://melbet62894.help/]http://melbet62894.help/[/url]
mostbet_oqpn –
мостбет live casino [url=https://mostbet15743.help]мостбет live casino[/url]
skolko stoit yzakonit pereplanirovky_gjMt –
Ребята, привет! Долго думал, стоит ли начинать эту волокиту. Акт скрытых работ потерял, да и проект сам переделывал. В общем, инспекция пришла и выписала предписание. И тут встал вопрос: узаконить перепланировку квартиры стоимость [url=https://skolko-stoit-uzakonit-pereplanirovku-10.ru]https://skolko-stoit-uzakonit-pereplanirovku-10.ru[/url] говорят, согласование перепланировки квартиры цена сильно выросла после ужесточения норм. Или взносы в жилинспекцию за выдачу акта. Если кто недавно проходил это ад, поделитесь. Без этого всё равно потом квартиру не продать. Короче, просто сколько отдать, чтобы спать спокойно с новой планировкой.
melbet_cwMr –
мелбет актуальное зеркало [url=https://www.melbet78240.help]https://www.melbet78240.help[/url]
AndrewCloxy –
Cialis 20mg price: LifeFlow – Cialis over the counter
melbet_xtMr –
мелбет официальный [url=https://www.melbet78240.help]https://www.melbet78240.help[/url]
mostbet_ffsi –
mostbet pl logowanie [url=https://www.mostbet26540.help]https://www.mostbet26540.help[/url]
mostbet_bdEi –
mostbet legit [url=http://mostbet06318.help/]mostbet legit[/url]
GregoryLip –
Cenforce 100mg tablets for sale: order cenforce – Cenforce 100mg tablets for sale
mostbet_qppn –
мостбет скачать 2026 [url=mostbet15743.help]мостбет скачать 2026[/url]
melbet_tdMr –
melbet комиссия на вывод [url=https://www.melbet78240.help]https://www.melbet78240.help[/url]
syvenirnaya prodykciya s logotipom_fxoa –
Коллеги, всем привет! Организуем встречу с дилерами, хочется сделать им приятные и полезные презенты. Посоветуйте нормальное изготовление корпоративных сувениров — чтобы и кружки не облазили, и ручки писали. брендированная продукция с логотипом [url=https://suvenirnaya-produkcziya-s-logotipom-11.ru]брендированная продукция с логотипом[/url] Реально ли найти недорогую сувенирную продукцию с логотипом с печатью от 100 штук. Бюджет пока не утвержден, поэтому хочу понять рыночные цены. А то маркетинговые агентства такой ценник лупят — закачаешься.
syvenirnaya prodykciya s logotipom_fokt –
Народ, привет! Ох, уже голова болит с этим тимбилдингом, нужны нормальные презенты для партнеров. Может, кто шарит где лучше брать сувенирную продукцию с логотипом. оригинальные подарки с логотипом [url=https://suvenirnaya-produkcziya-s-logotipom-10.ru]оригинальные подарки с логотипом[/url] Говорят, сейчас модно заказывать корпоративные подарки сувениры из экокожи — но кто делает качественно. Просили ещё брендированные кружки и толстовки. А то я уже второй день в интернете сижу и ничего адекватного не нашёл.
GregoryLip –
Levitra 10 mg best price: PrecisionCare Pharm – Levitra 20 mg for sale
WilliamDaulk –
mexico prescriptions: mexican pharmacy las vegas – buy drugs online
melbet_rzOi –
melbet казино [url=https://melbet62894.help/]https://melbet62894.help/[/url]
syvenirnaya prodykciya s logotipom_fupn –
Срочно нужен совет тем, кто занимается брендингом. Хотим обновить мерч для сотрудников. Везде говорят про индивидуальный подход, но реально где заказать корпоративные подарки с логотипом компании — чтоб не за границей, но и не откровенный шлак. деловые подарки [url=https://suvenirnaya-produkcziya-s-logotipom-9.ru]деловые подарки[/url] Интересует именно изготовление под ключ — от кружек до брендированных блокнотов. Нам нужно от 500 штук, можно меньше. Заранее спасибо, кто откликнется.
WilliamDaulk –
Le gГ©nГ©rique de Viagra: Viagra gГ©nГ©rique pas cher livraison rapide – Viagra homme prix en pharmacie sans ordonnance
Jeraldserne –
https://mexicorx.online/# mexican pharmacy online medications
mostbet_udEl –
мостбет бонус без депозита правда [url=https://mostbet34850.help/]мостбет бонус без депозита правда[/url]
plinko_rwKL –
plinko plinko betting [url=http://plinko37046.help]http://plinko37046.help[/url]
mostbet_cver –
mostbet рулетка [url=mostbet93580.help]mostbet93580.help[/url]
Narkolog na dom_mcOa –
Слушайте, какая история — близкий совсем плох, а везти в клинику нет никаких сил. Я сам через это прошел недавно совсем. Руки опускаются, время тикает. Лезешь в интернет, а вокруг только деньги тянут. Пока кто-то не подсказал один реально работающий вариант. Если нужна немедленная консультация — а везти самому нет физической возможности , то выход один . Я про круглосуточный вызов нарколога . У нас в Самаре, к слову , тоже полно левых контор без лицензии. Нормальные контакты, кто реально приезжает вот тут : наркология на дому вызов [url=https://narkolog-na-dom-samara-14.ru]https://narkolog-na-dom-samara-14.ru[/url] Откровенно говоря, после того как вник в детали, многое прояснилось . И про снятие запоя на дому, и про консультацию нарколога . И цены адекватные, без разводов. Рекомендую не тянуть .
WilliamDaulk –
apotek med fri frakt: extrem nГ¤stГ¤ppa – Svenska Pharma
Narkolog na dom_hzOt –
Случается, когда уже не до раздумий — родственник в запое , а тащить в клинику просто нереально . Моя семья такое пережила недавно. Руки опускаются, время идёт. Начинаешь обзванивать знакомых , а вокруг одни обещания . Пока случайно не наткнулся на один нормальный проверенный вариант. Если нужна немедленная консультация — а везти самому просто нереально, то нужно вызывать врача на дом. Я про вызвать нарколога на дом . У нас в Самаре, если честно, хватает шарлатанов . Нормальные контакты, кто реально приезжает ниже по ссылке: нарколог на дом срочно [url=https://narkolog-na-dom-samara-13.ru]нарколог на дом срочно[/url] Откровенно говоря, после того как прочитал , многое прояснилось . Там и про капельницы подробно , и про консультацию . Плюс анонимность — это важно . Советую не откладывать.
WilliamDaulk –
Viagra pas cher livraison rapide france: Sildenafil teva 100 mg sans ordonnance – Meilleur Viagra sans ordonnance 24h
mostbet_zuEl –
мостбет live линия [url=www.mostbet34850.help]www.mostbet34850.help[/url]
mostbet_mcEl –
мостбет aviator [url=http://mostbet34850.help/]http://mostbet34850.help/[/url]
plinko_sgKL –
plinko sign up bangladesh [url=http://plinko37046.help/]http://plinko37046.help/[/url]
plinko_mgKL –
plinko plinko app [url=plinko37046.help]plinko37046.help[/url]
mostbet_acer –
мостбет версия для ios [url=http://mostbet93580.help/]http://mostbet93580.help/[/url]
mostbet_kjer –
mostbet ошибка платежа [url=https://mostbet93580.help]mostbet ошибка платежа[/url]
WilliamDaulk –
farmacias online usa: progreso mexico pharmacy online – mexipharmacy reviews
mostbet_dapa –
aviator игра mostbet [url=mostbet30562.online]aviator игра mostbet[/url]
plinko_ypKL –
plinko bangladesh mirror [url=https://plinko37046.help/]https://plinko37046.help/[/url]
Jeraldserne –
https://mexicorx.online/# los algodones pharmacy online
mostbet_cver –
мостбет кэшбэк казино [url=https://www.mostbet93580.help]https://www.mostbet93580.help[/url]
WilliamDaulk –
bestГ¤lla nГ¤ringsdryck pГҐ recept: Svenska Pharma – Svenska Pharma
Narkolog na dom_nhOa –
Слушайте, какая история — человек в ступоре , а тащить в больницу нет никаких сил. Я сам через это прошел недавно совсем. Сидишь, не знаешь за что хвататься . Лезешь в интернет, а вокруг одни обещания . Пока кто-то не подсказал один нормальный проверенный вариант. Если нужна немедленная консультация — а везти самому просто нереально, то нужно вызывать врача на дом. Речь конкретно про выезд нарколога на дом. У нас в Самаре, если честно, хватает шарлатанов . Вся проверенная информация ниже по ссылке: нарколог на дом самара цены [url=https://narkolog-na-dom-samara-14.ru]нарколог на дом самара цены[/url] Честно скажу , после того как вник в детали, понял, как правильно действовать. Там и про капельницы подробно , и про последующее кодирование. И цены адекватные, без разводов. Рекомендую не откладывать.
vivod iz zapoya v stacionare_nepl –
Вот такая тема выматывает , когда близкий просто не может остановиться . Ломаешь голову , а вокруг одна потёмки . Знакомому потребовался действительно рабочий выход . Многие хватаются за таблетки , но это не помогает . Требуется именно профессиональная помощь . Пролистал пол-интернета , пока понял одну простую вещь: без круглосуточного наблюдения ничего не выйдет . Потому что дома срыв стопроцентный . Ищешь нормальный вариант для вывода из запоя в стационаре — тогда тебе сюда . В Нижнем Новгороде , кстати, тоже полно шарлатанов . Лучше сразу перейти на сайт, где реально раскладывают по полочкам про кодирование от алкоголизма и выезд врача . Подробности по ссылке: лечение алкоголизма в нижнем новгороде [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-22.ru]лечение алкоголизма в нижнем новгороде[/url] После прочтения , сам удивился , сколько подводных камней в этой теме. Главное — анонимность и палаты. Для Нижнего это проверенный временем вариант.
melbet_laet –
Друзья, всем здравствуйте. долго откладывал этот момент до последнего, но вчера все-таки начал пользоваться сервисом в melbet. Скажу так — очень зашло с первых минут,. У кого обычный андроид — всё четко и стабильно работает. Надо скачать мелбет на андроид? Там всё делается максимально просто,.
Короче, сами гляньте все условия по ссылке: . Кстати, кто спрашивал про скачать мелбет казино — всё очень удобно и грамотно сделано. И вывод средств действительно быстрый. Я лично всё проверил на себе — всё честно и без обмана. Всем искренне рекомендую. Удачи всем!
WilliamDaulk –
ashwagandha gravid: apotek handsprit – Svenska Pharma
mostbet_expa –
мостбет plinko [url=mostbet30562.online]mostbet30562.online[/url]
mostbet_kwpa –
mostbet casino slots [url=https://mostbet30562.online/]https://mostbet30562.online/[/url]
mostbet_jtEl –
мостбет slots [url=https://mostbet34850.help/]https://mostbet34850.help/[/url]
Narkologicheskii stacionar_pnOt –
Вот такой момент: подбор качественного стационара — это реально отдельная и очень сложная история. Нередко в жизни бывает так, когда родным или близким людям внезапно потребовалась экстренная и профессиональная поддержка. И в этот момент обычно начинается паника просто из-за банальной нехватки информации.
Я сам недавно детально изучал этот вопрос, искал по-настоящему работающий и безопасный выход. В интернете сейчас столько мусора и дорвеев, что голова идет кругом. Если коротко, лучше сразу перейти на официальный сайт, где нет вранья, там действительно раскладывают по полочкам всю подноготную про круглосуточную наркологическую поддержку и условия проживания. В общем, не тяните время и долго не раздумывайте,, чтобы четко во всем разобраться.
Все важные детали и лицензии центра находятся только тут: лечение алкоголизма в стационаре спб [url=http://www.narkologicheskij-staczionar-sankt-peterburg-12.ru]http://www.narkologicheskij-staczionar-sankt-peterburg-12.ru[/url]. Честно говоря, после изучения всех условий, насколько там много полезных нюансов и скрытых факторов, включая комфортные условия содержания, современные палаты и полную анонимность. Для Санкт-Петербурга это точно один из самых лучших вариантов, который стабильно работает и имеет хорошие отзывы.
melbet_pkpt –
Давно хотел найти надёжный вариант, честно говоря, уже не верил в адекватные условия. Но на днях близкий друг посоветовал про мелбет. Решил лично проверить систему — и теперь сам рекомендую знакомым.
В общем, вся нужная инфа доступна вот тут: мелбет казино скачать [url=https://iamthecoffeechic.com]мелбет казино скачать[/url]. Кстати, если кому надо скачать melbet — там процесс установки занимает буквально минуту. Я себе установил софт прямо на телефон — всё сделано очень удобно. И бонусы на первый депозит приятные, Доволен как слон, честно говоря. Удачи всем на дистанции!
Narkolog na dom_rdOa –
Слушайте, какая история — родственник в тяжелом запое , а везти в клинику нет никаких сил. Моя семья такое пережила пару лет назад . Руки опускаются, время тикает. Лезешь в интернет, а вокруг сплошной развод . Пока кто-то не подсказал один реально работающий вариант. Требуется немедленная консультация — а ехать куда-то просто нереально, то выход один . Я про выезд нарколога на дом. В Самаре , если честно, хватает шарлатанов . Вся проверенная информация ниже по ссылке: вызов нарколога цена [url=https://narkolog-na-dom-samara-14.ru]вызов нарколога цена[/url] Честно скажу , после того как вник в детали, многое прояснилось . И про снятие запоя на дому, и про консультацию нарколога . И цены адекватные, без разводов. Рекомендую не тянуть .
WilliamDaulk –
pharmacy mexico online: mexico pharmacy price list – farmacias mexicanas
mostbet_tcpa –
mostbet установить приложение [url=http://mostbet30562.online/]http://mostbet30562.online/[/url]
melbet_kioi –
melbet sportsbook registration [url=http://melbet14906.help/]http://melbet14906.help/[/url]
vivod iz zapoya v stacionare_vnpl –
Знаете ситуацию достала уже , когда человек просто срывается в штопор . Ломаешь голову , а вокруг одна реклама . Знакомому потребовался срочный выход . Многие хватаются за таблетки , но это не помогает . Требуется именно врачебное вмешательство . Пролистал пол-интернета , пока понял одну простую вещь: без круглосуточного наблюдения ничего толку не будет . Потому что дома срыв гарантирован . Если ищешь где сделать качественного вывода из запоя с помещением в клинику — обрати внимание на один проверенный вариант . В Нижнем Новгороде , кстати, тоже полно шарлатанов . Лучше сразу перейти на сайт, где нет вранья про кодировку от алкоголя и выезд врача . Вся суть здесь: лечение алкоголизма в нижнем новгороде [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-22.ru]лечение алкоголизма в нижнем новгороде[/url] Честно скажу , сам удивился , сколько подводных камней в этой теме. И кстати, цены адекватные. Для Нижнего это проверенный временем вариант.
luxury car rental miami_cuOi –
Let me save you some headache I learned the hard way. I swear half the “luxury” fleets down here are straight-up marketing scams. You book a premium ride online, arrive all excited, then boom — hidden service fees everywhere. Fool me thrice, shame on both of us I guess, lesson learned. When you are trying to find a reliable premium fleet down here, do some real digging first and read actual customer reviews. Miami without wheels is basically a hostage situation, especially since the AC must be arctic and you want zero mileage games.
I literally spent last month comparing maybe twenty different companies, but I eventually found a service with no bait, no switch, and no weird fine print. If you are looking for the only straight shooter for premium rentals across South Florida, check the details here: mia luxury car rental [url=https://luxury-car-rental-miami-3.com]mia luxury car rental[/url]. Yeah, valet in Miami Beach will cost you an arm, but that’s not their fault. Anyway, glad there’s at least one honest rental joint left in this town, hope this helps some of you save a few bucks.
WilliamDaulk –
Quand une femme prend du Viagra homme: Meilleur Viagra sans ordonnance 24h – Viagra vente libre pays
Narkologicheskii stacionar_iaOt –
Знаете, поиск действительно проверенного медицинского центра — это реально отдельная и очень сложная история. Многие лично сталкивались с такой ситуацией,, когда кому-то из членов семьи срочно понадобилась грамотная помощь врачей. И тут сразу возникает главный вопрос: куда именно везти человека?
Я сам недавно детально изучал этот вопрос, искал действительно надежный медицинский вариант. В интернете сейчас столько мусора и дорвеев, что голова идет кругом. Если коротко, лучше сразу перейти на официальный сайт, где нет вранья, там подробно расписаны все важные условия и нюансы про круглосуточную наркологическую поддержку и условия проживания. В такой ситуации лучше один раз внимательно глянуть самостоятельно, чтобы четко во всем разобраться.
Вся актуальная информация и контакты доступны прямо здесь: стационар наркологический санкт петербург [url=http://narkologicheskij-staczionar-sankt-peterburg-12.ru]http://narkologicheskij-staczionar-sankt-peterburg-12.ru[/url]. Честно говоря, после изучения всех условий, насколько там много полезных нюансов и скрытых факторов, и главное — там работают доктора, которые реально спасают людей. В Питере это определенно достойный внимания и доверия медицинский центр, который стабильно работает и имеет хорошие отзывы.
mostbet_lgkn –
mostbet live liniya [url=www.mostbet61024.help]mostbet live liniya[/url]
pinup_gjea –
pinup crash strategiya [url=http://pinup85993.help/]pinup crash strategiya[/url]
magazin premialnih tovarov_fqoi –
Мужики, привет. Долго выбирал, где найти действительно крутой подарок. Перерыл кучу вариантов, но нормального магазина эксклюзивных товаров — реально мало. А тут знакомый скинул. В общем, сам гляньте по ссылке: очень дорогой подарок [url=https://boutique-guide.ru]очень дорогой подарок[/url] Кстати, если ищете премиальные подарки для мужчин — там выбор реально офигенный. Я себе взял кожаную сумку — качество бомба. И цены соответствуют качеству. Сам теперь только там беру. Удачи с выбором!
melbet_fuoi –
melbet deposit problem [url=http://melbet14906.help/]http://melbet14906.help/[/url]
Jeraldserne –
https://svpharm.xyz/# schengenintyg pdf
WilliamDaulk –
Svenska Pharma: Svenska Pharma – hette ett apotek korsord
melbet_tmoi –
melbet odds [url=https://www.melbet14906.help]https://www.melbet14906.help[/url]
melbet_xgoi –
melbet free bet [url=https://melbet14906.help]https://melbet14906.help[/url]
mostbet_oikn –
mostbet call center [url=http://mostbet61024.help/]http://mostbet61024.help/[/url]
pinup_jeea –
pin-up turnir [url=http://pinup85993.help]pin-up turnir[/url]
mostbet_fhkn –
mostbet Termiz [url=https://mostbet61024.help/]https://mostbet61024.help/[/url]
KeithPeexy –
Levitra online USA fast: Macksood Urology Urological Services – Vardenafil online prescription
pinup_qyea –
pinup hisobni qanday tasdiqlash [url=pinup85993.help]pinup85993.help[/url]
Russellkig –
Dr. Macksood Urologist https://macksoodurology.com/ed-medications/viagra-sildenafil/ erectile dysfunction pills for sale
vivod iz zapoya v stacionare_orMi –
Вот такая ситуация — родственник срывается , а просто бессилен. Я через это прошёл пару лет назад. Сначала кажется, что обойдётся , но нет . Требуется реальная помощь . Перерыл весь интернет — одни обещания. А потом наткнулся на один действительно рабочий вариант. Ищешь где сделать качественное выведение из запоя с госпитализацией , не ведись на дешёвые обещания . У нас в Нижнем, к слову , полно левых контор. Реальные контакты тут : кодировка от наркотиков [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-25.ru]кодировка от наркотиков[/url] Честно говоря , после того как прочитал , понял свои ошибки. Там и про кодирование от алкоголизма расписано , и про выезд нарколога на дом . И цены адекватные. Рекомендую не откладывать.
vivod iz zapoya v stacionare_topl –
Знаете ситуацию выматывает , когда близкий просто не может остановиться . Ищешь варианты , а вокруг одна реклама . Мне вот потребовался действительно рабочий метод . Пьют успокоительное , но это не помогает . Нужно именно врачебное вмешательство . Пролистал пол-интернета , пока понял одну простую вещь: без нормальных условий ничего толку не будет . Потому что дома срыв стопроцентный . Ищешь нормальный вариант для экстренного вывода из запоя под капельницами — тогда тебе сюда . В Нижнем Новгороде , кстати, развелось этих “центров” . Советую перейти на сайт, где реально раскладывают по полочкам про кодировку от алкоголя и выезд врача . Подробности по ссылке: клиники по лечению алкоголизма [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-22.ru]клиники по лечению алкоголизма[/url] Честно скажу , сам удивился , сколько нюансов в этой теме. И кстати, цены адекватные. Для Нижнего это проверенный временем вариант.
mostbet_gnkn –
mostbet kazino free spins [url=mostbet61024.help]mostbet61024.help[/url]
pinup_gdea –
pin-up bonus kod [url=http://pinup85993.help/]http://pinup85993.help/[/url]
Russellkig –
Cialis without a doctor prescription https://macksoodurology.com/ed-medications/levitra-vardenafil/ pills for erectile dysfunction online
Russellkig –
Dr. Macksood Urologist https://macksoodurology.com buy erectile dysfunction treatment
melbet_xjet –
Слушайте, кто шарит, долго присматривался к разным платформам, но вчера все-таки начал пользоваться сервисом в melbet. Скажу так — очень зашло с первых минут,. У кого система ios — тоже всё без проблем запускается,. Надо melbet скачать на андроид? В интерфейсе даже ребёнок разберётся.
Короче, вся полезная инфа и актуальный сайт доступны вот тут: . Кстати, кто спрашивал про мелбет казино скачать — всё очень удобно и грамотно сделано. И вывод средств действительно быстрый. Я за месяц три раза выигрыш забирал — никаких косяков с выплатами нет,. Всем искренне рекомендую. Пользуйтесь на здоровье, пусть повезет!
vivod iz zapoya v stacionare_bcpl –
Знаете ситуацию реально бесит , когда человек просто срывается в штопор . Ломаешь голову , а вокруг одна реклама . Знакомому потребовался действительно рабочий выход . Многие хватаются за таблетки , но это не помогает . Нужно именно профессиональная помощь . Я перелопатил кучу сайтов , пока понял одну простую вещь: без нормальных условий ничего не выйдет . В обычной квартире срыв стопроцентный . Если ищешь где сделать экстренного вывода из запоя под капельницами — обрати внимание на один проверенный вариант . В Нижнем , кстати, тоже полно шарлатанов . Лучше сразу перейти на сайт, где реально раскладывают по полочкам про кодировку от алкоголя и выезд врача . Вся суть здесь: наркологические клиники в нижнем новгороде [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-22.ru]наркологические клиники в нижнем новгороде[/url] Честно скажу , сам удивился , сколько подводных камней в этой теме. И кстати, цены адекватные. Для нашего города это реально стоящий вариант.
vivod iz zapoya v stacionare_stMi –
Случается сплошь и рядом — близкий друг срывается , а просто бессилен. Моя семья столкнулась лично . Сначала кажется, что обойдётся , но нет . Нужна профессиональная медицина. Обзвонил десяток контор — сплошной развод . А потом наткнулся на один действительно рабочий вариант. Ищешь где сделать экстренный вывод из запоя под наблюдением врачей , не рискуй здоровьем. У нас в Нижнем, к слову , полно шарлатанов . Проверенная информация тут : кодировка от наркотиков [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-25.ru]кодировка от наркотиков[/url] Откровенно скажу, после того как прочитал , понял свои ошибки. Там и про кодирование от алкоголизма расписано , и про условия в стационаре. И цены адекватные. Советую не откладывать.
Russellkig –
buy cialis pill https://macksoodurology.com/erectile-dysfunction/ online ed medicine
KeithPeexy –
Buy Vardenafil online: Macksood Urology Urological Services – Buy Vardenafil 20mg
Russellkig –
Dr. Macksood Urologist https://macksoodurology.com/ed-medications/cialis-tadalafil/ ed meds online
aviator_zpPi –
aviator legit [url=https://aviator20596.help/]https://aviator20596.help/[/url]
melbet_euKl –
melbet règlement des gains [url=http://melbet29619.help]http://melbet29619.help[/url]
mostbet_mcKl –
как поставить ординар mostbet [url=https://mostbet74039.help]https://mostbet74039.help[/url]
mostbet_tjSr –
mostbet yutuq tushmayapti [url=https://mostbet60471.help/]https://mostbet60471.help/[/url]
melbet_zqSa –
melbet contact [url=http://melbet78692.help]melbet contact[/url]
pinup_ldmr –
pin up registratsiya muammo [url=http://pinup58663.help]http://pinup58663.help[/url]
mostbet_abkn –
lucky jet mostbet demo [url=mostbet59068.help]mostbet59068.help[/url]
mostbet_rqKl –
мостбет Visa [url=https://mostbet22685.online]https://mostbet22685.online[/url]
Russellkig –
Cheap Levitra online https://macksoodurology.shop online ed meds
JamesEvace –
best online ed pills [url=https://macksoodurology.com/ed-medications/#]Macksood Urology[/url] ed meds on line
Russellkig –
ED medications https://macksoodurology.shop erectile dysfunction pills online
mostbet_jdSr –
mostbet click orqali yechish [url=https://www.mostbet60471.help]https://www.mostbet60471.help[/url]
mostbet_wuKl –
мостбет вывод без комиссии [url=https://mostbet22685.online]https://mostbet22685.online[/url]
pinup_qwmr –
pin-up Apelsin yechish Oʻzbekiston [url=https://pinup58663.help/]https://pinup58663.help/[/url]
mostbet_xhKl –
как играть в mines мостбет [url=http://mostbet22685.online]http://mostbet22685.online[/url]
mostbet_veSr –
mostbet ilovada plinko [url=http://mostbet60471.help/]http://mostbet60471.help/[/url]
pinup_kamr –
pinup ios [url=https://pinup58663.help/]https://pinup58663.help/[/url]
vivod iz zapoya v stacionare_vspl –
Вот такая тема достала уже , когда родственник просто не может остановиться . Ищешь варианты , а вокруг одна реклама . Знакомому потребовался действительно рабочий выход . Многие хватаются за таблетки , но это не помогает . Требуется именно профессиональная помощь . Пролистал пол-интернета , пока понял одну простую вещь: без нормальных условий ничего толку не будет . Потому что дома срыв стопроцентный . Если ищешь где сделать качественного вывода из запоя с помещением в клинику — обрати внимание на один проверенный вариант . В Нижнем Новгороде , кстати, тоже полно шарлатанов . Лучше сразу перейти на сайт, где реально раскладывают по полочкам про кодирование от алкоголизма и выезд врача . Вся суть здесь: психиатр нарколог нижний новгород [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-22.ru]психиатр нарколог нижний новгород[/url] Честно скажу , сам офигел , сколько подводных камней в этой теме. И кстати, цены адекватные. Для нашего города это проверенный временем вариант.
melbet_opKl –
melbet mines stratégie [url=http://melbet29619.help/]melbet mines stratégie[/url]
aviator_ylPi –
aviator bonus [url=https://www.aviator20596.help]https://www.aviator20596.help[/url]
melbet_enSa –
melbet creare cont [url=http://melbet78692.help]http://melbet78692.help[/url]
mostbet_hbKl –
mostbet app скачать [url=mostbet74039.help]mostbet74039.help[/url]
Jamestup –
viagra Tadalafil price
KeithPeexy –
online ed medications Macksood Urology Urological Services ed rx online
mostbet_pbkn –
mostbet bonus kasyno warunki [url=http://mostbet59068.help]http://mostbet59068.help[/url]
melbet_mcKl –
melbet slots bonus [url=http://melbet29619.help]http://melbet29619.help[/url]
aviator_ltPi –
aviator account balance [url=https://aviator20596.help]https://aviator20596.help[/url]
melbet_dwSa –
ruleta live melbet [url=https://www.melbet78692.help]ruleta live melbet[/url]
mostbet_bfKl –
mostbet скачать на ios [url=https://mostbet74039.help/]https://mostbet74039.help/[/url]
mostbet_wjkn –
mostbet rankingi graczy [url=https://www.mostbet59068.help]https://www.mostbet59068.help[/url]
Russellkig –
levitra https://macksoodurology.com where can i buy erectile dysfunction pills
mostbet_kfSr –
mostbet Oʻzbekiston kazino bonus [url=http://mostbet60471.help/]http://mostbet60471.help/[/url]
mostbet_ewKl –
мостбет поддержка Кыргызстан [url=https://www.mostbet22685.online]https://www.mostbet22685.online[/url]
pinup_wnmr –
pinup depozit komissiya [url=https://www.pinup58663.help]https://www.pinup58663.help[/url]
melbet_vuKl –
melbet retrait par téléphone [url=https://melbet29619.help]https://melbet29619.help[/url]
aviator_lzPi –
aviator Khulna [url=http://aviator20596.help/]http://aviator20596.help/[/url]
melbet_jeSa –
bonus mines melbet [url=https://melbet78692.help/]https://melbet78692.help/[/url]
mostbet_bgKl –
lucky jet игра mostbet [url=http://mostbet74039.help/]http://mostbet74039.help/[/url]
mostbet_vdkn –
mostbet lucky jet wypłata [url=mostbet59068.help]mostbet59068.help[/url]
Jamestup –
Buy Levitra 20mg online Macksood Urology
JamesEvace –
Cialis over the counter [url=https://macksoodurology.com/ed-medications/cialis-tadalafil/#]Macksood Urology[/url] Macksood Urology Urological Services
Narkolog na dom_xcSt –
Никогда не думал, что столкнусь — родственник в тяжелом запое , а тащить куда-то нет никаких сил. Я сам через это прошел года два назад . Руки опускаются, а время тикает. Начинаешь обзванивать знакомых , а вокруг одни обещания . Пока кто-то не подсказал один реально работающий вариант. Требуется немедленная консультация — а ехать куда-то просто нереально, то нужно вызывать врача. Речь конкретно про выезд нарколога круглосуточно. В Москве , если честно, хватает шарлатанов . Вся проверенная информация ниже по ссылке: нарколог на дом круглосуточно [url=https://narkolog-na-dom-moskva-30.ru]нарколог на дом круглосуточно[/url] Откровенно скажу, после того как вник в детали, понял, как правильно действовать. И про снятие запоя на дому, и про консультацию нарколога . Плюс анонимность — это важно . Советую не откладывать.
Russellkig –
Cheap Levitra online https://macksoodurology.com/ed-medications/ erection pills online
KeithPeexy –
cheap ed meds Macksood Urology Urological Services ed pills
vivod iz zapoya v stacionare_mnMi –
Знаете, бывает — близкий друг уходит в штопор , а руки опускаются . Моя семья столкнулась пару лет назад. Сначала кажется, что обойдётся , но хрен там. Требуется реальная медицина. Обзвонил десяток контор — одни обещания. А потом наткнулся на один действительно рабочий вариант. Если тебе нужно экстренный вывод из запоя под наблюдением врачей , не рискуй здоровьем. У нас в Нижнем, если честно, полно шарлатанов . Проверенная информация тут : клиники по лечению алкоголизма [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-25.ru]клиники по лечению алкоголизма[/url] Честно говоря , после того как ознакомился, понял свои ошибки. И про кодировку от алкоголя подробно, и про выезд нарколога на дом . И цены адекватные. Советую не откладывать.
Jamestup –
Macksood Urology Urological Services levitra
Russellkig –
ED medications https://macksoodurology.shop ed online treatment
luxury car rental miami_odOr –
Been there, done that, got the overpriced tow truck receipt. Swear some of these “luxury” fleets down here should be in a museum instead of on the road. Plus the fine print says you can’t even drive outside the city limits without extra fees. No thanks, I’m way too old for this nonsense. When you genuinely need a proper and reliable premium ride to cruise around, do some real digging first and read actual customer reviews. Miami without a decent whip is basically a punishment, whether you are doing Coral Gables brunch, South Beach night run, or a spontaneous Everglades detour.
I’ve personally tested maybe 25 rental outfits across Dade and Broward, until I finally stumbled on one provider that doesn’t play games. If you are looking for the only straight-up source for premium wheels in South Florida, check the current details here: mercedes car rental near me [url=https://luxury-car-rental-miami-4.com]https://luxury-car-rental-miami-4.com[/url]. Also, definitely bring polarized shades unless you enjoy driving completely blind into the sunset. Just drive safe out there and maybe pass on that overpriced roadside assistance add-on. hope this helps some of you save a few bucks.
Narkolog na dom_ksSt –
Знаете, бывает такое — близкий на грани, а тащить куда-то просто невозможно . Я сам через это прошел года два назад . Сидишь, не знаешь за что хвататься . Начинаешь обзванивать знакомых , а вокруг сплошной развод. Пока кто-то не подсказал один нормальный проверенный вариант. Если нужна немедленная консультация — а ехать куда-то просто нереально, то нужно вызывать врача. Я про нарколога на дом . У нас в столице, если честно, хватает левых контор без лицензии. Нормальные контакты, кто реально приезжает вот тут : помощь при запое нарколог на дом [url=https://narkolog-na-dom-moskva-30.ru]помощь при запое нарколог на дом[/url] Откровенно скажу, после того как прочитал , многое прояснилось . Там и про капельницы подробно , и про консультацию нарколога . Плюс анонимность — это важно . Рекомендую не тянуть .
KeithPeexy –
Buy generic Levitra online: Levitra 20 mg for sale – Levitra 20 mg for sale
proekt pereplanirovki kvartiri_xxma –
Подскажите, кто реально знает. Нужно немного сдвинуть мокрую зону санузла. без официального проекта даже думать нечего начинать, Я уже знатно намучился со всей этой бюрократией, В общем, нашел нормальных адекватных ребят, которые делают всё под ключ — это доверить подготовку документов профессиональным инженерам, чтобы спать спокойно и не бояться проверок от управляющей.
И согласуют все этапы вообще без проблем. Там на сайте есть и примеры документов, и точные цены, перепланировка квартиры проектные организации [url=https://proekt-pereplanirovki-kvartiry30.ru]https://proekt-pereplanirovki-kvartiry30.ru[/url]. Не тяните до последнего, Обязательно перешлите этот пост тому, кто тоже сейчас затеял ремонт!
Russellkig –
order viagra https://macksoodurology.com/ed-medications/cialis-tadalafil/ ed treatment online
Narkologicheskaya pomosh_fqKi –
Вот такая беда приключилась — человек в запое , а куда бежать — совсем не знаешь . Моя семья такое пережила пару лет назад . Думаешь, сам справится, но нет . Требуется профессиональная помощь . Перерыл весь интернет — сплошной развод . Пока не нашел один действительно рабочий вариант. Нужна срочно лечение наркомании в Воронеже — не рискуй здоровьем близкого. В Воронеже , кстати , тоже полно левых контор без лицензии. Вся проверенная информация ниже по ссылке: лечение алкогольной зависимости воронеж [url=https://narkologicheskaya-pomoshh-voronezh-12.ru]https://narkologicheskaya-pomoshh-voronezh-12.ru[/url] Откровенно говоря, после того как прочитал , понял свои ошибки. И про кодирование, и про условия в клинике. И цены адекватные. Рекомендую не тянуть .
Jamestup –
Dr. Macksood Urologist discount ed pills
JamesEvace –
pills for erectile dysfunction online [url=https://macksoodurology.com/#]Dr. Macksood Urologist[/url] best ed meds online
luxury car rental miami_plkr –
Seriously, the amount of garbage “luxury” deals down here is astonishing. You see a sweet ride online — clean spec, fair price, looks legit. Different car, scratches all over, and that “all-inclusive” price? Yeah that didn’t include insurance, fees, or the mandatory cleaning charge. I’ve lived here for years and still get burned occasionally. When you’re after a trustworthy and reliable premium vehicle to cruise around, don’t just grab the cheapest option on Kayak. Miami without proper wheels is basically a hostage situation, especially since the AC must freeze your teeth and you want unlimited miles or bust.
Most of these local agencies are just smoke and mirrors with decent SEO hiding overpriced junk, until I finally found one outfit that actually delivers what’s in the listing. If you are looking for the only honest broker for premium vehicles across South Florida, check the current availability here: car rentals in miami [url=https://luxury-car-rental-miami-5.com]https://luxury-car-rental-miami-5.com[/url]. Also, definitely bring quality shades unless you enjoy driving into a nuclear flare every single evening. Anyway, glad there’s at least one straight shooter left in this rental jungle, hope this helps some of you save a few bucks.
mostbet_reOl –
мостбет вывести с баланса [url=http://mostbet83506.help]http://mostbet83506.help[/url]
Russellkig –
ED medications https://macksoodurology.shop ed pills
tkan dlya mebeli_dqEn –
Ребята, выручайте! Кот старый диван в клочья разодрал, надо перетягивать. Ищу, где можно ткань для обивки мебели купить не по космическим ценам. обивочная ткань для диванов [url=https://tkan-dlya-mebeli-1.ru]https://tkan-dlya-mebeli-1.ru[/url] Говорят, флок и микровелюр быстро вытираются, а рогожка лучше. Нужен метров 15-20, может, кто знает нормального поставщика.
mostbet_bper –
mostbet pagina oficială [url=https://mostbet93547.help/]https://mostbet93547.help/[/url]
mostbet_jmkn –
mostbet lucky jet играть [url=http://datsun-do.ru/]http://datsun-do.ru/[/url]
Jamestup –
Macksood Urology Urological Services erectile dysfunction
luxury car rental miami_grkr –
Let me save you some serious time, learned this the hard way. You see a sweet ride online — clean spec, fair price, looks legit. Different car, scratches all over, and that “all-inclusive” price? Yeah that didn’t include insurance, fees, or the mandatory cleaning charge. I’ve lived here for years and still get burned occasionally. When you’re after a trustworthy and reliable premium vehicle to cruise around, don’t just grab the cheapest option on Kayak. Miami without proper wheels is basically a hostage situation, whether you are doing Design District shopping, late-night South Beach cruising, or a spontaneous drive down to Homestead.
I’ve personally gone through maybe 30 rental companies across Dade, Broward, and Palm Beach, but I eventually found a service with no games, no bait-and-switch, and no hidden asterisks. If you are looking for the only honest broker for premium vehicles across South Florida, check the current availability here: rolls royce cullinan for rent near me [url=https://luxury-car-rental-miami-5.com]https://luxury-car-rental-miami-5.com[/url]. Also, definitely bring quality shades unless you enjoy driving into a nuclear flare every single evening. Anyway, glad there’s at least one straight shooter left in this rental jungle, let me know if you guys have any other clean spots.
Russellkig –
erectile dysfunction https://macksoodurology.shop ed online prescription
mostbet_dxOl –
mostbet обновить приложение [url=www.mostbet83506.help]mostbet обновить приложение[/url]
mostbet_gsOl –
mostbet подтвердить аккаунт [url=www.mostbet83506.help]www.mostbet83506.help[/url]
Jamestup –
buy erectile dysfunction pills online levitra
tkan dlya mebeli_euEn –
Ребята, выручайте! Кот старый диван в клочья разодрал, надо перетягивать. Ищу, где можно ткань для обивки мебели купить не по космическим ценам. ткань для обивки кресел [url=https://tkan-dlya-mebeli-1.ru]https://tkan-dlya-mebeli-1.ru[/url] А то везде пишут разное, а на деле хочется купить ткань мебельную и забыть на пару лет. Нужен метров 15-20, может, кто знает нормального поставщика.
mostbet_ldkn –
mostbet забыл пароль [url=datsun-do.ru]datsun-do.ru[/url]
JamesEvace –
online ed pharmacy [url=https://macksoodurology.com/#]Macksood Urology Urological Services[/url] cheap ed drugs
mostbet_htOl –
мостбет максимальная ставка [url=https://mostbet83506.help]https://mostbet83506.help[/url]
luxury car rental miami_pukl –
I’ve got the scars to prove it, the rental landscape down here is crazy. Then you show up at the local lot to pick up the car. Different car waiting — scratches everywhere, smells like an ashtray, and that “amazing price”? Doesn’t include the mandatory $400 cleaning fee or the $30 per day toll pass you can’t waive. Eight years in South Florida and these clowns still almost get me. If you are trying to find a legitimate luxury fleet without getting ripped off, run far from the airport counters. Anyone who’s waited for an Uber in August understands exactly what I mean about this city, especially since the AC must be arctic cold and unlimited miles non-negotiable.
Most of these local agencies are just shiny websites hiding the same beat-up fleet with fake reviews, but I eventually found a service where what you book is exactly what shows up, no surprises, no fine print nightmares. If you are looking for the only honest source for premium wheels across South Florida, check the current details here: renting luxury cars near me [url=https://luxury-car-rental-miami-8.com]renting luxury cars near me[/url]. Also, definitely bring serious shades unless you enjoy driving straight into the sun like a zombie every single evening. Anyway, glad there’s at least one straight operator left in this rental circus, hope this helps some of you save a few bucks.
mostbet_dhkn –
mostbet скачать через зеркало [url=https://www.datsun-do.ru]https://www.datsun-do.ru[/url]
mostbet_haer –
mostbet mastercard [url=http://mostbet93547.help/]mostbet mastercard[/url]
mostbet_oter –
mostbet dota 2 [url=http://mostbet93547.help]mostbet dota 2[/url]
Russellkig –
ED medications https://macksoodurology.com/ed-medications/cialis-tadalafil/ best online ed treatment
mostbet_crkn –
игровые автоматы мостбет [url=http://datsun-do.ru]http://datsun-do.ru[/url]
Narkologicheskaya pomosh_jcKn –
Случается сплошь и рядом — человек пропадает , а куда бежать — непонятно . Я через это прошел лично . Пьют успокоительное, но нет . Требуется реальная медицина. Перерыл весь интернет — одни обещания . Пока не нашел один действительно рабочий вариант. Нужна круглосуточная наркологическая помощь — не ведись на дешевые акции . В Воронеже , кстати , тоже полно левых контор без лицензии. Реальные контакты ниже по ссылке: наркологическая клиника [url=https://narkologicheskaya-pomoshh-voronezh-11.ru]наркологическая клиника[/url] Честно скажу , после того как ознакомился, понял свои ошибки. Там и про вывод из запоя , и про реабилитацию . И цены адекватные. Советую не откладывать.
Jamestup –
Sildenafil Citrate Tablets 100mg Dr. Macksood Urologist
luxury car rental miami_dnen –
Okay folks gather round — Miami rental horror story time. You find a killer listing online: sleek Audi, convertible, price almost too good to be true. Plus a surprise $3000 hold on your credit card for two weeks right before giving you the keys. Nine years in South Florida and these clowns still nearly fool me. If you are trying to find a legitimate luxury fleet without getting ripped off, stay the hell away from the airport rental center. Anyone who’s tried the trolley system knows what I’m talking about about this city, whether you are doing Coconut Grove dinner, Sunny Isles sunrise, or a spontaneous drive down to Homestead.
Most of these local agencies are just polished turds with fake five-star reviews hiding overpriced junk, until I finally found one company that doesn’t play stupid games. If you are looking for the only trustworthy source for premium rides across South Florida, check the current details here: luxury car rental in miami [url=https://luxury-car-rental-miami-9.com]luxury car rental in miami[/url]. Also, definitely bring polarized shades unless you enjoy driving blind into the sunset every single night. Anyway, glad there’s at least one honest operator left in this rental jungle, let me know if you guys have any other clean spots.
mostbet_wjer –
mostbet mines pe telefon [url=https://mostbet93547.help/]mostbet mines pe telefon[/url]
tkan dlya mebeli_utEn –
Ребята, выручайте! Кот старый диван в клочья разодрал, надо перетягивать. Теперь мучаюсь — какую взять ткань для мебели, чтобы и выглядело достойно, и кошачьи когти выдержало. купить ткань для дивана [url=https://tkan-dlya-mebeli-1.ru]https://tkan-dlya-mebeli-1.ru[/url] А то везде пишут разное, а на деле хочется купить ткань мебельную и забыть на пару лет. Буду благодарен за любые советы, особенно от тех, кто сам перетягивал.
Russellkig –
levitra https://macksoodurology.com/ed-medications/viagra-sildenafil/ online ed treatments
KeithPeexy –
ed prescription online: Macksood Urology Urological Services – buying erectile dysfunction pills online
Jamestup –
Macksood Urology Urological Services cialis for sale
luxury car rental miami_izen –
Okay folks gather round — Miami rental horror story time. Then you roll up to the local address to pick up the car. Plus a surprise $3000 hold on your credit card for two weeks right before giving you the keys. Fool me nine times? That’s just the Miami welcome committee, lesson learned. If you are trying to find a legitimate luxury fleet without getting ripped off, stay the hell away from the airport rental center. Anyone who’s tried the trolley system knows what I’m talking about about this city, whether you are doing Coconut Grove dinner, Sunny Isles sunrise, or a spontaneous drive down to Homestead.
I’ve tested maybe 50 rental outfits across Dade, Broward, and Collier, until I finally found one company that doesn’t play stupid games. If you are looking for the only trustworthy source for premium rides across South Florida, check the current details here: rent cadillac escalade near me [url=https://luxury-car-rental-miami-9.com]https://luxury-car-rental-miami-9.com[/url]. Also, definitely bring polarized shades unless you enjoy driving blind into the sunset every single night. Just drive safe out there and definitely skip that “emergency roadside” upsell — complete waste of money. let me know if you guys have any other clean spots.
Russellkig –
Macksood Urology Urological Services https://macksoodurology.com cheap ed pills online
luxury car rental miami_ehEa –
Been there, done that, got the overpriced tow truck receipt to prove it. You find this amazing listing online — gorgeous spec, fair daily rate, looks perfect. Totally different vehicle waiting for you — bald tires, dashboard lit up like a Christmas tree, and that “amazing rate”? Doesn’t include the mandatory $40 daily toll pass or the $350 “premium location” fee they spring on you at the counter. Fool me twelve times? That’s just the 305 way, lesson learned. If you are trying to find a legitimate luxury fleet without getting ripped off, run far from the airport counters. Miami without real wheels is basically a nightmare, whether you are doing Coconut Grove brunch, Sunny Isles sunrise cruise, or a spontaneous drive down to the Keys.
I’ve tested maybe 65 rental outfits across Dade, Broward, and Monroe, until I finally found one company that doesn’t play stupid games. If you are looking for the only straight shooter for premium rides across South Florida, check the current details here: luxury car hire [url=https://luxury-car-rental-miami-12.com]luxury car hire[/url]. Yeah, parking in Brickell will cost you a nice dinner — but that’s the price of paradise. Just drive safe out there and absolutely skip that “windshield protection” upsell — complete waste of money. hope this helps some of you save a few bucks.
mostbet_zgsr –
мостбет профиль [url=https://mostbetskg.buzz/]https://mostbetskg.buzz/[/url]
mostbet_zxMi –
mostbet вход 2026 [url=www.mostbetskg.fun]www.mostbetskg.fun[/url]
mostbet_hxSt –
мостбет apk Киргизия [url=http://most-bet-kg.online/]http://most-bet-kg.online/[/url]
Jamestup –
ED medications Macksood Urology
KeithPeexy –
cheapest ed online Dr. Macksood Urologist ed online prescription
luxury car rental miami_gvkl –
I’ve got the scars to prove it, the rental landscape down here is crazy. You find this amazing deal online: brand new Beamer, unlimited miles, price that makes you smile. Different car waiting — scratches everywhere, smells like an ashtray, and that “amazing price”? Doesn’t include the mandatory $400 cleaning fee or the $30 per day toll pass you can’t waive. Fool me eight times? That’s just another Tuesday in the 305, lesson learned. If you are trying to find a legitimate luxury fleet without getting ripped off, do some real digging first and read actual customer reviews. Miami without decent wheels is basically a hostage situation, whether you are doing South of Fifth brunch, Design District shopping, or a spontaneous Keys trip.
I’ve run through maybe 45 rental companies across Dade, Broward, and Monroe, but I eventually found a service where what you book is exactly what shows up, no surprises, no fine print nightmares. If you are looking for the only honest source for premium wheels across South Florida, check the current details here: south beach exotic car rentals [url=https://luxury-car-rental-miami-8.com]south beach exotic car rentals[/url]. Yeah, parking in South Beach will cost you a nice bottle of wine — but that’s the Miami tax. Anyway, glad there’s at least one straight operator left in this rental circus, hope this helps some of you save a few bucks.
mostbet_rfml –
mostbet minimal depozit [url=https://www.mostbet47654.help]https://www.mostbet47654.help[/url]
pinup_giet –
pin-up shaxsiy kabinet kirish [url=http://pinup77432.help/]pin-up shaxsiy kabinet kirish[/url]
mostbet_heKn –
mostbet pasport bilan verifikatsiya [url=mostbet10093.help]mostbet10093.help[/url]
luxury car rental miami_dzEa –
Alright listen up because I’m about to save you a massive headache. Then you actually show up to the local office to pick up the car. Totally different vehicle waiting for you — bald tires, dashboard lit up like a Christmas tree, and that “amazing rate”? Doesn’t include the mandatory $40 daily toll pass or the $350 “premium location” fee they spring on you at the counter. Twelve years in South Florida and these jokers still almost catch me sleeping. If you are trying to find a legitimate luxury fleet without getting ripped off, run far from the airport counters. Anyone who’s waited for an Uber in August heat knows the struggle exactly about this city, whether you are doing Coconut Grove brunch, Sunny Isles sunrise cruise, or a spontaneous drive down to the Keys.
I’ve tested maybe 65 rental outfits across Dade, Broward, and Monroe, until I finally found one company that doesn’t play stupid games. If you are looking for the only straight shooter for premium rides across South Florida, check the current details here: luxury car rental agency [url=https://luxury-car-rental-miami-12.com]luxury car rental agency[/url]. Yeah, parking in Brickell will cost you a nice dinner — but that’s the price of paradise. Anyway, glad there’s at least one honest operator left in this rental jungle, let me know if you guys have any other clean spots.
Russellkig –
viagra https://macksoodurology.shop cheapest ed medication
mostbet_nbsr –
мостбет вход не работает [url=https://mostbetskg.buzz/]https://mostbetskg.buzz/[/url]
mostbet_jfsr –
мостбет отыгрыш бонуса [url=https://mostbetskg.buzz]https://mostbetskg.buzz[/url]
Jamestup –
Dr. Macksood Urologist Cheapest Sildenafil online
mostbet_wzMi –
mostbet как вывести на кошелек [url=https://mostbetskg.fun]https://mostbetskg.fun[/url]
mostbet_upSt –
мостбет android Киргизия [url=https://most-bet-kg.online]мостбет android Киргизия[/url]
mostbet_jzSt –
mostbet приложение 2026 [url=http://most-bet-kg.online/]mostbet приложение 2026[/url]
mostbet_ssMi –
как играть в crash мостбет [url=http://mostbetskg.fun/]http://mostbetskg.fun/[/url]
mostbet_bssr –
мостбет доступ Киргизия сегодня [url=http://mostbetskg.buzz]мостбет доступ Киргизия сегодня[/url]
pinup_qvet –
pin-up sms kod kelmayapti [url=pinup77432.help]pinup77432.help[/url]
mostbet_byml –
mostbet royxatdan otish [url=mostbet47654.help]mostbet royxatdan otish[/url]
mostbet_hmKn –
mostbet mobil kazino [url=www.mostbet10093.help]www.mostbet10093.help[/url]
mostbet_shMi –
mostbet apk с официального сайта [url=www.mostbetskg.fun]mostbet apk с официального сайта[/url]
mostbet_yySt –
мостбет новый адрес [url=http://most-bet-kg.online]http://most-bet-kg.online[/url]
mostbet_avKn –
mostbet yuklab olish apk [url=https://mostbet10093.help/]mostbet yuklab olish apk[/url]
pinup_mqet –
pin-up koeffitsientlar [url=http://pinup77432.help]http://pinup77432.help[/url]
mostbet_xgml –
mostbet telefon raqamni tasdiqlash [url=https://www.mostbet47654.help]mostbet telefon raqamni tasdiqlash[/url]
Jamestup –
levitra cialis
JamesEvace –
buy Viagra over the counter [url=https://macksoodurology.com/ed-medications/viagra-sildenafil/#]Buy Viagra online cheap[/url] Macksood Urology Urological Services
Gordonbek –
cheap ed treatment: Macksood Urology Urological Services – online ed meds
mostbet_ktKn –
mostbet masuliyatli oyin [url=http://mostbet10093.help/]http://mostbet10093.help/[/url]
pinup_hiet –
pinup toʻlov kartasi bog‘lash [url=http://pinup77432.help/]http://pinup77432.help/[/url]
mostbet_abml –
mostbet ios app yuklab olish [url=mostbet47654.help]mostbet ios app yuklab olish[/url]
Robertwed –
apotek Г¶ppet 24/7: Svenska Pharma – snabbtest apotek
Alvinblats –
https://svrate.xyz/# Svenska Pharma
RichardAduct –
b vitamin apotek: foundation stick bГ¤st i test – billigt serum
mostbet_brka –
мостбет ios Кыргызстан [url=http://mostbet55146.online/]мостбет ios Кыргызстан[/url]
mostbet_xbMi –
mostbet как активировать бонус [url=https://mostbetskg.fun]https://mostbetskg.fun[/url]
Miguelcic –
Sildenafil 100mg price https://macksoodurology.shop cheap ed pills online
Alvinblats –
https://mexicorate.icu/# legitimate mexican pharmacy online
Michaelstula –
SildГ©nafil 100 mg sans ordonnance [url=https://sansordonnancepharm.online/#]Viagra femme ou trouver[/url] Viagra vente libre allemagne
RichardAduct –
kГ¶p pГҐ nГ¤tet: Svenska Pharma – fotsvamp engelska
mostbet_blPi –
мостбет слоты 2026 [url=https://mostbet12087.online/]https://mostbet12087.online/[/url]
Alvinblats –
https://pharmserate.icu/# Svenska Pharma
RichardAduct –
Viagra pas cher livraison rapide france: Viagra pas cher livraison rapide france – Viagra homme prix en pharmacie
mostbet_pkka –
mostbet чат поддержки [url=www.mostbet55146.online]www.mostbet55146.online[/url]
mostbet_pbpl –
mostbet descarcare gratuita [url=mostbet56730.help]mostbet56730.help[/url]
melbet_inEr –
melbet depunere nu intra [url=www.melbet31393.help]melbet depunere nu intra[/url]
mostbet_ihka –
мостбет Кант [url=https://www.mostbet55146.online]мостбет Кант[/url]
mostbet_joMi –
как зарегистрироваться в mostbet [url=http://mostbetskg.fun/]http://mostbetskg.fun/[/url]
sericit_qmml –
серицит галтованный купить [url=seritsit.ru]серицит галтованный купить[/url]
mostbet_twMi –
mostbet версия для ios [url=https://mostbetskg.fun]https://mostbetskg.fun[/url]
mostbet_xika –
mostbet скачать apk [url=https://www.mostbet55146.online]mostbet скачать apk[/url]
RichardAduct –
Svenska Pharma: Svenska Pharma – apotek hГ¤mta recept
mostbet_rzPi –
мостбет вывод без комиссии [url=www.mostbet12087.online]www.mostbet12087.online[/url]
mostbet_fqPi –
mostbet промоакции [url=http://mostbet12087.online]http://mostbet12087.online[/url]
mostbet_aaMi –
mostbet mines на деньги [url=http://mostbetskg.fun]mostbet mines на деньги[/url]
melbet_kjEr –
pariuri pe mma melbet [url=https://www.melbet31393.help]pariuri pe mma melbet[/url]
melbet_czEr –
retragere pe card melbet [url=https://www.melbet31393.help]https://www.melbet31393.help[/url]
RichardAduct –
Viagra pas cher livraison rapide france: SildГ©nafil 100mg pharmacie en ligne – Le gГ©nГ©rique de Viagra
mostbet_ojpl –
mostbet autentificare rapidă [url=https://mostbet56730.help]mostbet autentificare rapidă[/url]
mostbet_snPi –
mostbet контакты [url=http://mostbet12087.online]mostbet контакты[/url]
Alvinblats –
https://sansordonnancefr.icu/# Viagra pas cher livraison rapide france
mostbet_kxpl –
mostbet metode plata Moldova [url=http://mostbet56730.help]mostbet metode plata Moldova[/url]
JamesSkids –
farmacia mexicana en linea: mexican rx – medicine mexico
melbet_qzEr –
melbet lucky jet Republica Moldova [url=http://melbet31393.help/]http://melbet31393.help/[/url]
Robertwed –
nГ¤tapoteket: bГ¤sta root lift – deodorant barn
RichardAduct –
Svenska Pharma: Svenska Pharma – svenska apotek
mostbet_tppl –
mostbet cont verificat [url=http://mostbet56730.help]http://mostbet56730.help[/url]
Alvinblats –
https://sansordonnancepharm.online/# Meilleur Viagra sans ordonnance 24h
JamesSkids –
order meds from mexico: can i buy meds from mexico online – mexican drugstore
RichardAduct –
c vitamin apotek: Svenska Pharma – spruta apotek
mostbet_ivsr –
mostbet stavkani bekor qilish [url=https://mostbet94259.help/]https://mostbet94259.help/[/url]
Alvinblats –
https://mexicorate.icu/# mexico online farmacia
melbet_asOa –
melbet login ci [url=http://melbet79845.help/]http://melbet79845.help/[/url]
pinup_ehot –
pin-up UZS depozit [url=www.pinup38399.help]www.pinup38399.help[/url]
mostbet_mtpa –
mostbet бонус за регистрацию [url=www.familyclub.borda.ru/?1-2-0-00001327-000-0-0]mostbet бонус за регистрацию[/url]
JamesSkids –
pharmacy in mexico city: mexico pharmacies – reliable rx pharmacy
RichardAduct –
tijuana pharmacy online: mexican rx pharm – progreso, mexico pharmacy online
aviator_siEl –
aviator yaş məhdudiyyəti [url=http://aviator16053.help]aviator yaş məhdudiyyəti[/url]
Alvinblats –
https://pharmrate.online/# pharmacys in mexico
aviator_xnOt –
aviator भारत में aviator साइट [url=http://aviator17492.help]http://aviator17492.help[/url]
mostbet_tikr –
mostbet aksiyalar 2026 [url=mostbet48518.help]mostbet48518.help[/url]
JamesSkids –
Viagra pas cher livraison rapide france: Viagra homme prix en pharmacie – Meilleur Viagra sans ordonnance 24h
RichardAduct –
Viagra homme sans prescription: Viagra femme ou trouver – Viagra sans ordonnance livraison 24h
melbet_jeOa –
melbet lol [url=http://melbet79845.help/]http://melbet79845.help/[/url]
mostbet_ajsr –
mostbet aviator koeffitsiyent [url=http://mostbet94259.help]http://mostbet94259.help[/url]
pinup_gjot –
pin up live tikish [url=https://pinup38399.help/]https://pinup38399.help/[/url]
mostbet_kvsr –
mostbet url [url=https://mostbet94259.help]mostbet url[/url]
melbet_hoOa –
melbet aviator ios [url=https://www.melbet79845.help]melbet aviator ios[/url]
pinup_gsot –
pinup mobil kirish [url=http://pinup38399.help]pinup mobil kirish[/url]
obzor DBBET_osOa –
бонусы DBBET для новых игроков [url=www.admiralshow.forum24.ru/?1-3-0-00000156-000-0-0]бонусы DBBET для новых игроков[/url]
aviator_uvEl –
aviator qeydiyyat qaydası [url=https://www.aviator16053.help]https://www.aviator16053.help[/url]
Alvinblats –
https://sansordonnancefr.icu/# Viagra Pfizer sans ordonnance
aviator_bcEl –
aviator turnir oyun [url=http://aviator16053.help]aviator turnir oyun[/url]
top bykmekerskih kontor_jhKl –
надежные букмекерские конторы [url=rodoslav.forum24.ru/?1-4-0-00002251-000-0-0]надежные букмекерские конторы[/url]
top bk_whoa –
самые лучшие бк [url=https://bukmekerskie-kontory-mira.carrd.co/]самые лучшие бк[/url]
mostbet_ybsr –
mostbet saytda aviator [url=https://mostbet94259.help/]https://mostbet94259.help/[/url]
RichardAduct –
Viagra gГ©nГ©rique pas cher livraison rapide: SildГ©nafil Teva 100 mg acheter – Le gГ©nГ©rique de Viagra
mostbet_vzpa –
mostbet регистрация и вход [url=https://www.assa0.myqip.ru/?1-4-0-00009957-000-0-0]mostbet регистрация и вход[/url]
pinup_zpot –
pin-up to‘lov tasdiqlash [url=pinup38399.help]pinup38399.help[/url]
JamesSkids –
Viagra g̩n̩rique sans ordonnance en pharmacie: Viagra sans ordonnance livraison 24h РViagra homme sans prescription
aviator_doEl –
aviator rəsmi sayt az [url=www.aviator16053.help]www.aviator16053.help[/url]
mostbet_cqkr –
mostbet Oʻzbekiston cashback [url=https://mostbet48518.help]mostbet Oʻzbekiston cashback[/url]
BK Megapari_whOn –
БК Мегапари [url=https://megapari.jimdosite.com]БК Мегапари[/url]
gid po stavkam_axSr –
гид по ставкам на спорт [url=www.alfatraders.borda.ru/?1-0-0-00007751-000-0-0]гид по ставкам на спорт[/url]
mostbet_yokr –
mostbet Angren [url=https://mostbet48518.help]mostbet Angren[/url]
Alvinblats –
https://pharmserate.icu/# Svenska Pharma
RichardAduct –
Svenska Pharma: apotek se recept – Svenska Pharma
melbet_jbOa –
melbet vérification avant retrait [url=https://www.melbet79845.help]melbet vérification avant retrait[/url]
JamesSkids –
h̴ltagning apotek: r̦d i ansiktet h̦gt blodtryck РSvenska Pharma
mostbet_gtkr –
mostbet setka tennis [url=http://mostbet48518.help/]http://mostbet48518.help/[/url]
top bk_evoa –
топ букмекеров [url=https://bukmekerskie-kontory.infinityfree.me/]топ букмекеров[/url]
aviator_ndOt –
aviator सेल्फ एक्सक्लूजन [url=https://www.aviator17492.help]https://www.aviator17492.help[/url]
Robertwed –
mexico pharmacy list: mexico pharmacies – buying prescriptions in mexico
aviator_ngOt –
aviator मिरर लिंक [url=https://aviator17492.help]https://aviator17492.help[/url]
Alvinblats –
https://sansordonnancepharm.online/# Viagra homme sans ordonnance belgique
aviator_azOt –
aviator phonepe से डिपॉजिट [url=aviator17492.help]aviator17492.help[/url]
RichardAduct –
Viagra homme sans prescription: Viagra vente libre pays – п»їViagra sans ordonnance 24h
BK Megapari_wbOn –
мегапари ставки [url=www.megapari.mozellosite.com]мегапари ставки[/url]
BK Megapari_gjOn –
БК Мегапари [url=megapari.jimdosite.com]БК Мегапари[/url]
JamesSkids –
mexican pharmacies that ship to the united states: meds from mexico – mexican farmacia
obzor DBBET_hnOa –
вывод средств в DBBET [url=www.admiralshow.forum24.ru/?1-3-0-00000156-000-0-0]вывод средств в DBBET[/url]
Robertwed –
Svenska Pharma: Svenska Pharma – Svenska Pharma
top bk_lcoa –
топ букмекеров [url=bukmekerskie-kontory.infinityfree.me/]топ букмекеров[/url]
JamesSkids –
Svenska Pharma: Svenska Pharma – Svenska Pharma
akcii bykmekerskih kontor_kymt –
бонусы букмекерских контор [url=http://www.sites.google.com/view/bonusy-kontor/]бонусы букмекерских контор[/url]
melbet_vfma –
mirror melbet [url=www.melbet42815.help]www.melbet42815.help[/url]
DavidSic –
islam makhachev ufc: ufc 330 start time – ufc fight night
mostbet_bdol –
мостбет приложение не работает [url=https://mostbet33907.online]мостбет приложение не работает[/url]
luxury car rental miami_jqkr –
Okay folks gather around because this Miami rental nightmare needs to be discussed. You see a sweet ride online — clean spec, fair price, looks legit. Plus they want a $2000 hold on your debit card. I’ve lived here for years and still get burned occasionally. miami car rental luxury — don’t just grab the cheapest option on Kayak. Miami without proper wheels is basically a hostage situation. leather seats that don’t fuse to your skin in August. I’ve gone through maybe 30 rental companies across Dade, Broward, and Palm Beach. Finally found one outfit that actually delivers what’s in the listing. Here’s the only honest broker for premium vehicles across South Florida
exotic rentals miami beach [url=https://luxury-car-rental-miami-5.com]https://luxury-car-rental-miami-5.com[/url] also bring quality shades unless you enjoy driving into a nuclear flare every evening. Anyway glad there’s at least one straight shooter left in this rental jungle.
akcii bykmekerskih kontor_fbmt –
акции букмекерских контор [url=bukmeker-kontor.ucoz.net]акции букмекерских контор[/url]
aviator_znPr –
aviator play store [url=www.aviator85462.help]www.aviator85462.help[/url]
mostbet_pjol –
mostbet как вывести на кошелек [url=https://www.mostbet33907.online]https://www.mostbet33907.online[/url]
DavidSic –
islam makhachev ufc: ufc – ufc
aviator_niSi –
aviator down malawi [url=aviator95405.online]aviator95405.online[/url]
aviator_haSi –
aviator mw sign up [url=https://aviator95405.online]https://aviator95405.online[/url]
Ralphhef –
https://ufc-330.com/# ufc fight night
aviator_leSi –
aviator coupon today [url=http://aviator95405.online/]http://aviator95405.online/[/url]
luxury car rental miami_hrkl –
I’ve got the scars to prove it. Then you show up at the lot. Plus they freeze $2500 on your card for a week. Fool me eight times? That’s just another Tuesday in the 305. miami car rental luxury — run far from the airport counters. anyone who’s waited for an Uber in August understands. South of Fifth brunch, Design District shopping, or a spontaneous Keys trip — AC must be arctic cold and unlimited miles non-negotiable. most are shiny turds with five-star fake reviews on Google Maps. what you book is what shows up, no surprises, no fine print nightmares. prices swing like crazy so check before the weekend rush:
luxury car rental coral gables miami [url=https://luxury-car-rental-miami-8.com]luxury car rental coral gables miami[/url] also bring serious shades unless you enjoy driving straight into the sun like a zombie. Anyway glad there’s at least one straight operator left in this rental circus.
DavidSic –
Islam Makhachev: islam makhachev ufc – ufc 330 fight card
aviator_piPr –
aviator güzgü necə tapılır [url=aviator85462.help]aviator85462.help[/url]
aviator_anPr –
aviator hesab [url=https://aviator85462.help]aviator hesab[/url]
Ralphhef –
https://ufc-330.com/# ufc
mostbet_alol –
mostbet промокод для Кыргызстана [url=https://www.mostbet33907.online]https://www.mostbet33907.online[/url]
luxury car rental miami_hben –
Okay folks gather round — Miami rental horror story time. Then you roll up to the address. Plus a $3000 hold on your credit card for two weeks. Fool me nine times? That’s just the Miami welcome committee. those guys are pros at the bait-and-switch. anyone who’s tried the trolley system knows what I’m talking about. leather seats that don’t glue to your skin in August. most are polished turds with fake five-star reviews. what you reserve is what you get, period, end of story. Here’s the only trustworthy source for premium rides across South Florida
south beach exotic rentals [url=https://luxury-car-rental-miami-9.com]https://luxury-car-rental-miami-9.com[/url] also bring polarized shades unless you enjoy driving blind into the sunset every night. drive safe and definitely skip that “emergency roadside” upsell — complete waste of money.
melbet_foma –
melbet lucky jet castiguri [url=https://www.melbet42815.help]https://www.melbet42815.help[/url]
Ralphhef –
https://ufc-330.com/# ufc fight night
DavidSic –
ufc 330 tickets: ufc fight night – islam makhachev ufc
luxury car rental miami_uwea –
Let me save you some serious pain with this Miami rental nonsense. Then you actually show up to grab the keys. Plus they put a $4000 hold on your card and say it’ll take two weeks to release. Eleven years in South Florida and these clowns still almost get me. luxury car rental in miami. anyone who’s tried the bus here knows exactly what I mean. leather seats that won’t fuse to your legs in August. I’ve tested maybe 60 rental companies across Dade, Broward, and Collier. Finally found one outfit that actually delivers what’s in the photos. Here’s the only honest source for premium rides across South Florida
rolls royce cullinan for rent near me [url=https://luxury-car-rental-miami-11.com]https://luxury-car-rental-miami-11.com[/url] Yeah parking in South Beach will cost you a nice bottle of champagne — but that’s the Miami tax. drive safe and definitely skip that “tire and wheel” upsell — pure profit for them, zero value for you.
DavidSic –
ufc fight night: ufc 330 tickets – ufc 330 start time
flagman bykmeker_uwEl –
flagman букмекер [url=https://www.site-8.voog.com]flagman букмекер[/url]
melbet_srma –
melbet depunere nu intra [url=www.melbet42815.help]melbet depunere nu intra[/url]
Raymondtex –
Viagra homme prix en pharmacie: Viagra homme prix en pharmacie – Viagra homme prix en pharmacie sans ordonnance
luxury car rental miami_bwea –
Let me save you some serious pain with this Miami rental nonsense. Then you actually show up to grab the keys. Completely different car sitting there — dents everywhere, smells like cheap air freshener covering something worse, and that “dream price”? Doesn’t include the mandatory $50 daily insurance or the $300 “administrative fee” they invent at checkout. Eleven years in South Florida and these clowns still almost get me. When you’re searching for a legit luxury car rental miami. anyone who’s tried the bus here knows exactly what I mean. Key Biscayne sunset, Design District shopping, or a spontaneous drive down to the Everglades — AC must be arctic and unlimited miles non-negotiable. I’ve tested maybe 60 rental companies across Dade, Broward, and Collier. Finally found one outfit that actually delivers what’s in the photos. Here’s the only honest source for premium rides across South Florida
premium car hire [url=https://luxury-car-rental-miami-11.com]premium car hire[/url] also bring polarized shades unless you enjoy driving into the sun like a blind bat. Anyway glad there’s at least one straight operator left in this rental circus.
Louiswrery –
Effectively voiced indeed. !
Wein Plaza – https://weinplaza.com/
Raymondtex –
Viagra pas cher livraison rapide france: SildГ©nafil 100 mg sans ordonnance – Viagra prix pharmacie paris
flagman bykmeker_pwEl –
БК Флагман [url=www.tumblr.com/blog/kekswin365]БК Флагман[/url]
luxury car rental miami_wgki –
I’ve paid my dues so you don’t have to. You spot this killer offer online — brand new Porsche, zero excess, price that screams “book me”. Plus they freeze $5500 on your card and say “it’ll drop off in two weeks”. Fool me twenty times? That’s just called Tuesday in the 305. those people are professional scammers with nice smiles and better shoes. anyone who’s tried public transport here knows I’m not joking. South Beach dinner, Design District shopping, or a spontaneous Keys adventure — AC must be arctic and unlimited miles non-negotiable. I’ve tested so many rental companies across Dade, Broward, and Palm Beach. no games, no bait-and-switch, no hidden fees on page 8. prices change hourly so don’t wait around:
porsche 911 carrera for rent near me [url=https://luxury-car-rental-miami-20.com]https://luxury-car-rental-miami-20.com[/url] also bring polarized shades unless you enjoy driving into the sun like a zombie. drive safe and absolutely skip that “windshield protection” upsell — pure profit for them, zero for you.
Edwinerece –
https://frsansordonnance.online/# Viagra homme prix en pharmacie sans ordonnance
mostbet_tmsi –
mostbet crash bonus [url=mostbet02606.online]mostbet02606.online[/url]
mostbet_vgsn –
как играть в mines mostbet [url=http://mostbet70131.online/]http://mostbet70131.online/[/url]
melbet_rgKi –
мелбет лотереи [url=https://melbet38319.online/]https://melbet38319.online/[/url]
mostbet_vzpa –
mostbet bónusz jóváírás [url=https://www.mostbet44364.online]mostbet bónusz jóváírás[/url]
mostbet_xhor –
mines game mostbet [url=www.mostbet33044.online]mines game mostbet[/url]
luxury car rental miami_yaEi –
I’ve been burned more times than a cheap steak at a tourist trap. You find this amazing offer online — beautiful car, great rate, everything seems perfect. Completely different car waiting for you — smells like stale cigarettes, check engine light glowing, and that “great rate”? Doesn’t include the mandatory $35 daily toll pass, the $200 cleaning fee, or the $75 “after-hours pickup” charge. Honestly, I’m tired of this nonsense. luxury car rental miami florida. Miami without real wheels is basically a slow death. Design District shopping, late-night South Beach cruising, or a spontaneous Keys trip — AC must be freezing and unlimited miles or walk. most are just pretty websites hiding the same old garbage. Finally found one that actually keeps its word. prices move fast so check them out:
premium car rental [url=https://luxury-car-rental-miami-16.com]premium car rental[/url] Yeah parking in Miami Beach will cost you — but that’s life here. drive safe and skip the extra insurance upsell, it’s a joke.
melbet_hgEl –
melbet букмекерская контора киргизия [url=https://melbet05281.online/]melbet букмекерская контора киргизия[/url]
Raymondtex –
my mexican pharmacy: farmacia online usa – farmacias mexicanas
luxury car rental miami_zxki –
I’ve paid my dues so you don’t have to. You spot this killer offer online — brand new Porsche, zero excess, price that screams “book me”. Different car waiting — dents everywhere, smells like cheap air freshener covering something worse, and that “killer price”? Doesn’t include the mandatory $55 daily toll pass or the $450 “convenience fee” they invent at checkout. Fool me twenty times? That’s just called Tuesday in the 305. those people are professional scammers with nice smiles and better shoes. anyone who’s tried public transport here knows I’m not joking. leather seats that won’t weld to your legs in July. I’ve tested so many rental companies across Dade, Broward, and Palm Beach. no games, no bait-and-switch, no hidden fees on page 8. Here’s the only straight shooter for premium rides across South Florida
premium car rental in miami [url=https://luxury-car-rental-miami-20.com]premium car rental in miami[/url] Yeah parking in South Beach will cost you a nice bottle of wine — but that’s the Miami tax. Anyway glad there’s at least one honest operator left in this town.
Edwinerece –
https://pharmrate.monster/# mexicanrxpharm
mejdynarodnie plateji_lcPi –
Кстати, недавно наткнулся на обсуждение текущей ситуации с переводами. Сам уже не первый месяц ищу нормальный способ отправить деньги, без лишних проблем и комиссий. В общем, если вас тоже волнует эта тема — узнайте подробности тут. Детальный разбор ситуации по платежам за рубежом: денежные переводы за границу [url=https://mezhdunarodnye-platezhi-lor.ru]https://mezhdunarodnye-platezhi-lor.ru[/url] И ещё момент учтите, что без адекватных тарифов любые международные платежи превращаются в головную боль. Ну и напоследок — всегда смотрите несколько вариантов, прежде чем платить.
Raymondtex –
gravidbГ¤lte apotek: bestГ¤lla recept apotek – Svenska Pharma
Raymondtex –
pharmacy online: medicine mexico – mexipharmacy reviews
mostbet_opsi –
mostbet express kupon strategiya [url=http://mostbet02606.online/]mostbet express kupon strategiya[/url]
Edwinerece –
https://swtop.online/# hur mycket välling 6 månader
mejdynarodnie plateji_fjPi –
Кстати, недавно наткнулся на обсуждение реальных кейсов. Сам уже давно ищу нормальный способ провести транзакцию, без лишних проблем и комиссий. В общем, если вас тоже волнует эта тема — узнайте подробности тут. Там расписаны основные нюансы по международным транзакциям: переводы за рубеж [url=https://mezhdunarodnye-platezhi-lor.ru]https://mezhdunarodnye-platezhi-lor.ru[/url] И да, имейте в виду, что без нормального обменного курса любые международные платежи превращаются в сплошной геморрой. Добавлю по опыту — лучше перепроверять несколько сервисов, прежде чем платить.
mostbet_dlpa –
mostbet játék letöltés [url=https://www.mostbet44364.online]mostbet játék letöltés[/url]
Raymondtex –
Svenska Pharma: apotej – Svenska Pharma
mostbet_nior –
мостбет telegram [url=http://mostbet33044.online]http://mostbet33044.online[/url]
melbet_syEl –
melbet не приходит код [url=http://melbet05281.online/]http://melbet05281.online/[/url]
mostbet_musi –
mostbet azn ilə oyun [url=www.mostbet02606.online]www.mostbet02606.online[/url]
Edwinerece –
https://sepharmtop.online/# kan ni utslag
mejdynarodnie plateji_vhEn –
Знаете, — где лучше всего организовать перевода денег за границу онлайн. Друзья посоветовали вот этот материал: перевод за границу онлайн [url=https://mezhdunarodnye-platezhi-nar.ru]перевод за границу онлайн[/url] Суть в том, — не все способы одинаково выгодны. Да и сами понимаете такая транзакция — это риск переплатить в два раза. И ещё момент, — до любой операции почитайте свежие отзывы. В противном случае легко попасть на лишние траты. Короче, — стоит разобраться заранее.
Edwinerece –
https://frsansordonnance.online/# Viagra sans ordonnance 24h suisse
mostbet_ojor –
мостбет киберспорт ставка [url=mostbet33044.online]mostbet33044.online[/url]
melbet_ltEl –
melbet android киргизия [url=https://melbet05281.online/]https://melbet05281.online/[/url]
mejdynarodnie plateji_hrPi –
Постоянно возвращаюсь к одной теме — какой вариант реально рабочий для платежей за рубежом. Порылся в интернете — смотрите, тут годнота: онлайн переводы денег за границу [url=https://mezhdunarodnye-platezhi-tov.ru]https://mezhdunarodnye-platezhi-tov.ru[/url] Короче, суть такая — курс валют может убить любую выгоду. Ну сами понимаете любой очередной международный перевод — это всегда головная боль без нормальной инфы. Обратите внимание — прежде чем отправлять проверьте актуальные отзывы. Иначе легко переплатить в два раза. Моё мнение — стоит один раз разобраться.
Edwinerece –
https://frsansordonnance.online/# Acheter Sildenafil 100mg sans ordonnance
mejdynarodnie plateji_xhEn –
Честно говоря, — как найти адекватный способ международных транзакций. Эксперты рекомендуют вот этот разбор: перевод денег за границу онлайн [url=https://mezhdunarodnye-platezhi-nar.ru]перевод денег за границу онлайн[/url] Если коротко, — не все способы одинаково выгодны. Да и сами понимаете перевод за границу онлайн — это потеря времени без нормальной инфы. Кстати, — перед тем как отправлять сравните условия. В противном случае легко пролететь с курсом. Как по мне — не поленитесь проверить информацию.
Edwinerece –
https://swtop.online/# senna te apotek
mostbet_wfpa –
mostbet mobil [url=https://www.mostbet44364.online]https://www.mostbet44364.online[/url]
Edwinerece –
https://sepharmtop.online/# köp på nätet
mostbet_hrMt –
mostbet platební karta [url=http://mostbet35880.online]mostbet platební karta[/url]
mostbet_nfor –
mostbet 404 xato [url=https://mostbet39687.help]https://mostbet39687.help[/url]
pinup_lhEa –
pinup toʻlovni bekor qilish [url=https://pinup38742.help/]pinup toʻlovni bekor qilish[/url]
mostbet_cksn –
мостбет фриспины в казино [url=https://www.mostbet70131.online]мостбет фриспины в казино[/url]
Edwinerece –
https://swtop.online/# eksem hund bilder
mejdynarodnie plateji_hppl –
Слушайте, вот уже который раз убеждаюсь — как выбрать реально работающий способ для платежей за рубежом. Случайно набрел на годный материал: платежи для импортеров [url=https://mezhdunarodnye-platezhi-kap.ru]https://mezhdunarodnye-platezhi-kap.ru[/url] Короче, если по факту — курс конвертации часто занижают. Потому что любой очередной международный перевод — это головная боль с отслеживанием статуса. Вот ещё важный момент — перед финальным подтверждением проверьте все комиссии до копейки. Без этого легко остаться в минусе только на конвертации. Короче — стоит разобраться заранее перед любой отправкой.
Edwinerece –
https://pharmrate.monster/# order from mexico
mostbet_alsn –
mostbet фора [url=https://mostbet70131.online]https://mostbet70131.online[/url]
Howardsmila –
https://healthspherepharmacy.com/# indian pharmacy
Travishak –
mexico pharmacy: mexican pharmacy online – mexico pharmacy
melbet_siKi –
melbet регистрация россия [url=http://melbet38319.online/]http://melbet38319.online/[/url]
mostbet_uzkl –
mostbet промокод не работает [url=https://mostbet11528.online/]mostbet промокод не работает[/url]
pinup_nvEa –
pinup xavfsizmi [url=https://www.pinup38742.help]pinup xavfsizmi[/url]
mostbet_yyMt –
mostbet push notifikace [url=www.mostbet35880.online]www.mostbet35880.online[/url]
mostbet_egor –
mostbet app orqali depozit [url=https://www.mostbet39687.help]mostbet app orqali depozit[/url]
Travishak –
mexican online pharmacy: mexico pharmacy – mexico pharmacy
Howardsmila –
https://casasaludpharmacy.com/# mexican online pharmacy
zakazat kyhnu_fqMr –
Ребята всем привет. Менеджеры врут про сроки. Короче, нашел нормальный вариант — купить заказать кухню под ключ. Фурнитура Blum. В общем, смотрите по ссылке — купить готовую кухню от производителя [url=https://zakazat-kuhnyu-bnm.ru]https://zakazat-kuhnyu-bnm.ru[/url] Проверяйте производителя. Перешлите тому кто ищет.
zakazat kyhnu_rupa –
Люди помогите советом. На Авито ловить боюсь — нарвусь на брак. То цены такие что проще новую квартиру купить. Короче, единственные кто не наваривается в тридорога — купить готовую кухню в спб со склада. Фасады из влагостойкого МДФ. В общем, вся инфа вот здесь — купить кухню от производителя в спб [url=https://zakazat-kuhnyu-rty.ru]купить кухню от производителя в спб[/url] Не ведитесь на салоны в ТЦ которые просто заказывают у тех же китайцев. Перешлите тому кто тоже мучается выбором.
zakazat kyhnu_tgpt –
Ребята всем привет. Задолбался я выбирать кухню уже полгода. Пересмотрел ютуб с отзывами — голова пухнет. Короче, единственные кто не наебывает — купить кухню в спб без переплат. Там и цены адекватные. В общем, жмите чтобы не потерять контакты — купить кухню в спб от производителя [url=https://zakazat-kuhnyu-gkl.ru]https://zakazat-kuhnyu-gkl.ru[/url] Не ведитесь на салоны-прокладки с наценкой в два раза. Перешлите тому кто тоже кухню ищет.
Travishak –
canada online pharmacy: best canadian pharmacy – canadian online pharmacy
melbet_hlKi –
мелбет пополнение через сбербанк онлайн [url=melbet38319.online]melbet38319.online[/url]
Howardsmila –
https://healthspherepharmacy.shop/# online shopping pharmacy india
pinup_tbEa –
pinup app ishlamayapti [url=http://pinup38742.help/]pinup app ishlamayapti[/url]
Travishak –
india pharmacy: indian pharmacy online – online pharmacy no rx
mostbet_hpMt –
mostbet přihlášení v aplikaci [url=http://mostbet35880.online/]mostbet přihlášení v aplikaci[/url]
Howardsmila –
https://northbridgepharm.shop/# canada online pharmacy
zakazat kyhnu_frst –
Народ кто в теме. Фурнитуру ставят дешманскую которая через год клинит. То кромка кривая через раз. Короче, реальный цех в СПб без наценок — купить кухню в спб с установкой. Цены ниже рыночных на треть. В общем, жмите чтобы не потерять — купить готовую кухню в спб [url=https://zakazat-kuhnyu-dfg.ru]купить готовую кухню в спб[/url] Не ведитесь на салоны-прокладки с накруткой. Перешлите другу кто тоже мучается.
mostbet_vuor –
mostbet tennis live [url=http://mostbet39687.help]http://mostbet39687.help[/url]
zakazat kyhnu_mpMr –
Народ привет. Менеджеры врут про сроки. Короче, нашел нормальный вариант — купить готовую кухню в спб. Цены ниже на 30%. В общем, жмите чтобы не потерять — купить готовую кухню спб [url=https://zakazat-kuhnyu-bnm.ru]купить готовую кухню спб[/url] Проверяйте производителя. Перешлите тому кто ищет.
Travishak –
pharmacy in canada: canadian prescription pharmacy – online canadian pharmacy
zakazat kyhnu_wfpa –
Люди помогите советом. Задолбался я уже два месяца мучиться. То сроки изготовления по полгода обещают. Короче, реальные ребята без дураков — купить кухню в спб с доставкой и сборкой. Фасады из влагостойкого МДФ. В общем, жмите чтобы не потерять контакт — где лучше купить кухню в спб [url=https://zakazat-kuhnyu-rty.ru]https://zakazat-kuhnyu-rty.ru[/url] Не ведитесь на салоны в ТЦ которые просто заказывают у тех же китайцев. Сам столько нервов потратил теперь делюсь.
Howardsmila –
https://northbridgepharm.shop/# best canadian pharmacy
Travishak –
canadian pharmacy online: canadian pharmacy – canadian pharmacy
melbet_htEn –
melbet crash how to play [url=https://melbet97946.online/]https://melbet97946.online/[/url]
mostbet_jrKr –
мостбет правила казино [url=https://mostbet15298.online]https://mostbet15298.online[/url]
mostbet_gzkt –
mostbet [url=www.mostbet72681.help]www.mostbet72681.help[/url]
melbet_cwsi –
мелбет пардохт тавассути Корти миллӣ [url=melbet73919.online]мелбет пардохт тавассути Корти миллӣ[/url]
Howardsmila –
https://casasaludpharmacy.com/# mexican online pharmacy
Travishak –
indian pharmacies safe: indian pharmacy online – overseas pharmacy no prescription
mostbet_eakl –
мостбет войти [url=https://mostbet11528.online]мостбет войти[/url]
zakazat kyhnu_ouMr –
Народ привет. Фурнитуру ставят дешманскую. Короче, нашел нормальный вариант — купить заказать кухню под ключ. Фурнитура Blum. В общем, смотрите по ссылке — где купить кухню в спб [url=https://zakazat-kuhnyu-bnm.ru]где купить кухню в спб[/url] Не ведитесь на салоны. Перешлите тому кто ищет.
zakazat kyhnu_gppa –
Слушайте кто недавно кухню делал. В Леруа Мерлен посмотрел — качество ужас. То сроки изготовления по полгода обещают. Короче, нашел наконец нормальное производство — заказать кухню напрямую у производителя. Цены ниже чем в салонах тысяч на 30-40. В общем, вся инфа вот здесь — купить готовую кухню в спб [url=https://zakazat-kuhnyu-rty.ru]купить готовую кухню в спб[/url] Не ведитесь на салоны в ТЦ которые просто заказывают у тех же китайцев. Перешлите тому кто тоже мучается выбором.
Travishak –
canadian prescription pharmacy: pharmacy in canada – NorthBridge Pharmacy
Howardsmila –
https://northbridgepharm.com/# canadian pharmacy
mostbet_oqkl –
mostbet зеркало Киргизия [url=https://mostbet11528.online/]https://mostbet11528.online/[/url]
Travishak –
pharmacy website india: india pharmacy – overseas pharmacy no prescription
Howardsmila –
https://northbridgepharm.shop/# pharmacy in canada
melbet_pqEn –
melbet online [url=melbet97946.online]melbet97946.online[/url]
Travishak –
online mexican pharmacy: mexican online pharmacy – mexico pharmacy
zakazat kyhnu_dkst –
Питерцы отзовитесь. Менеджеры врут про сроки и материалы. То доставку три месяца ждать. Короче, нашел нормальных производителей — купить кухню спб в наличии. Цены ниже рыночных на треть. В общем, вся инфа вот тут — заказать кухню [url=https://zakazat-kuhnyu-dfg.ru]заказать кухню[/url] Не ведитесь на салоны-прокладки с накруткой. Сам полгода выбирал теперь знаю.
kyhni SPb_shMl –
Люди подскажите Прошерстил 30 салонов — везде перекупы То ручки через месяц шатаются Короче, нашел наконец нормальную контору — кухни на заказ в спб с фурнитурой Blum Цены ниже чем в магазинах на 50 тысяч В общем, смотрите сами по ссылке — кухня на заказ [url=https://kuhni-spb-nbg.ru]кухня на заказ[/url] Проверяйте производителя по этому списку Сам полгода выбирал теперь знаю
zakazat kyhnu_zrSa –
Народ кто в Питере живет. Цены задрали как на золото. То доставку месяц ждать. Короче, мужики с руками из правильного места — купить кухню в спб с доставкой. Цены ниже чем в магазинах тысяч на 50. В общем, там цены и каталог — купить заказать кухню [url=https://zakazat-kuhnyu-qwe.ru]https://zakazat-kuhnyu-qwe.ru[/url] Проверяйте по этому списку. Перешлите кому надо.
Howardsmila –
http://northbridgepharm.com/# canada pharmacy
mostbet_yikt –
мостбет как пополнить MasterCard [url=https://www.mostbet72681.help]https://www.mostbet72681.help[/url]
zakazat kyhnu_pvpt –
Народ привет. То доставку ждать три месяца. Пересмотрел ютуб с отзывами — голова пухнет. Короче, реальные производители с совестью — купить кухню спб с установкой. Замерщик приехал на следующий день. В общем, там каталог и цены и отзывы реальные — заказать кухню [url=https://zakazat-kuhnyu-gkl.ru]заказать кухню[/url] Проверяйте производителя в этом списке. Перешлите тому кто тоже кухню ищет.
Travishak –
mexican pharmacy: mexican pharmacy online – mexican pharmacy
melbet_ktEn –
melbet rocket deposit [url=http://melbet97946.online]http://melbet97946.online[/url]
melbet_kssi –
мелбет барориш дар Тоҷикистон [url=http://melbet73919.online]мелбет барориш дар Тоҷикистон[/url]
Howardsmila –
https://healthspherepharmacy.com/# top online pharmacy india
kyhni SPb_haoi –
Слушайте кто кухню недавно заказывал Прошерстил кучу салонов — везде перекупы То фасады кривые Короче, нашел наконец нормальное производство — заказать кухню с фурнитурой Blum Фасады из влагостойкого МДФ 19 мм В общем, смотрите сами по ссылке — кухня на заказ спб от производителя недорого [url=https://kuhni-spb-uio.ru]https://kuhni-spb-uio.ru[/url] Проверяйте производителя по этому списку Сам столько нервов потратил теперь делюсь
Travishak –
mexico pharmacy: online mexican pharmacy – mexican pharmacy online
mostbet_chkt –
aviator игра мостбет [url=https://mostbet72681.help]aviator игра мостбет[/url]
Travishak –
canadian online pharmacy: pharmacy in canada – pharmacy in canada
Howardsmila –
https://northbridgepharm.com/# canada pharmacy online
kyhni SPb_ztPt –
Питерцы отзовитесь Менеджеры врут про сроки и материалы То доставку три месяца ждать Короче, реальный цех в СПб без наценок — кухни СПб от производителя напрямую Кромка ПВХ 2 мм немецкая В общем, вся инфа вот тут — изготовление кухни на заказ в спб [url=https://kuhni-spb-ytr.ru]https://kuhni-spb-ytr.ru[/url] Проверяйте производителя по этому списку Сам полгода выбирал теперь знаю
melbet_iisi –
мелбет пардохт [url=https://melbet73919.online/]мелбет пардохт[/url]
kyhni SPb_rwKn –
Доброго дня, земляки Качество пластилин То фасады перекошены Короче, мужики с руками из нужного места — кухни в спб от производителя из массива Сделали за три недели как обещали В общем, там цены и каталог работ — заказать кухню в спб от производителя [url=https://kuhni-spb-fpk.ru]заказать кухню в спб от производителя[/url] Проверяйте производителя по этому списку Перешлите тому кто тоже мучается
Travishak –
mexican online pharmacy: mexico pharmacy – CasaSalud Pharmacy
Howardsmila –
http://casasaludpharmacy.com/# online mexican pharmacy
Travishak –
top online pharmacy india: india pharmacy – no rx needed pharmacy
pinup_hpel –
pin-up crash o‘yini [url=pinup64200.help]pinup64200.help[/url]
Howardsmila –
https://casasaludpharmacy.shop/# online mexican pharmacy
mostbet_mwet –
мостбет одиночная ставка [url=mostbet99204.online]мостбет одиночная ставка[/url]
mostbet_bksa –
mostbet cz sázky [url=https://mostbet36836.online]https://mostbet36836.online[/url]
mostbet_hrsn –
mostbet bitcoin depozit [url=https://www.mostbet42672.help]https://www.mostbet42672.help[/url]
kyhni SPb_bwSt –
Здорова, народ Продаваны врут про материалы То кромка отклеивается через месяц Короче, нашел наконец нормальное производство — кухни СПб напрямую от производителя Замерщик приехал на следующий день В общем, сохраняйте себе в закладки — кухни под заказ в спб [url=https://kuhni-spb-wxh.ru]https://kuhni-spb-wxh.ru[/url] Не ведитесь на салоны в ТЦ которые просто заказывают у китайцев и ставят наценку 100% Сам столько нервов потратил теперь делюсь опытом
Travishak –
п»їlegitimate online pharmacies india: india pharmacy – online pharmacy no prescription needed
kyhni SPb_edPt –
Народ кто в теме Замучился я уже кухню искать То кромка кривая через раз Короче, нашел нормальных производителей — кухни в спб от производителя из массива Фасады на выбор из 50 цветов В общем, жмите чтобы не потерять — заказ кухни спб [url=https://kuhni-spb-ytr.ru]заказ кухни спб[/url] Не ведитесь на салоны-прокладки с накруткой Перешлите другу кто тоже мучается
kyhni SPb_xiMl –
Народ всем привет Замучился я уже кухню выбирать То фасады перекошены Короче, нашел наконец нормальную контору — кухни на заказ под ключ Кромка немецкая 2 мм В общем, сохраняйте в закладки — кухни в спб на заказ [url=https://kuhni-spb-nbg.ru]кухни в спб на заказ[/url] Проверяйте производителя по этому списку Сам полгода выбирал теперь знаю
mostbet_ibpr –
мостбет фрибет [url=https://zakaz.kg]мостбет фрибет[/url]
Howardsmila –
https://northbridgepharm.shop/# NorthBridge Pharmacy
Travishak –
canadian pharmacy: canadian online pharmacy – pharmacy in canada
mostbet_eqKr –
mostbet актуальное зеркало [url=http://mostbet15298.online]http://mostbet15298.online[/url]
Howardsmila –
http://casasaludpharmacy.com/# mexico pharmacy
Travishak –
reputable indian online pharmacy: india pharmacy – п»їinternational drug mart
pinup_dkel –
pin-up apk ni qanday yuklab olish [url=https://pinup64200.help/]pin-up apk ni qanday yuklab olish[/url]
Davidkab –
Viagra homme prix en pharmacie: Sildenafil teva 100 mg sans ordonnance – Prix du Viagra 100mg en France
DanielGes –
https://pharmaciefr.click/# Viagra gГ©nГ©rique sans ordonnance en pharmacie
mostbet_ybet –
mostbet банковская карта [url=http://mostbet99204.online/]mostbet банковская карта[/url]
mostbet_bzst –
mostbet limit wypłat dzienny [url=https://www.mostbet18361.online]mostbet limit wypłat dzienny[/url]
pinup_mwel –
pinup Qashqadaryo [url=https://pinup64200.help]https://pinup64200.help[/url]
Davidkab –
Svenska Pharma: Svenska Pharma – Svenska Pharma
DanielGes –
https://svenskapharm.click/# vilket apotek Г¤r billigast
mostbet_vaKr –
мостбет обновить приложение [url=http://mostbet15298.online/]мостбет обновить приложение[/url]
mostbet_xzpr –
mostbet ставки лайв Кыргызстан [url=http://zakaz.kg/]http://zakaz.kg/[/url]
mostbet_dcet –
мостбет как вывести на MasterCard [url=https://mostbet99204.online/]https://mostbet99204.online/[/url]
Davidkab –
order medication from mexico: mexico pharmacy list – pharmacy mexico online
DanielGes –
https://svenskapharm.click/# Svenska Pharma
mostbet_rdsa –
mostbet ruleta mobil [url=https://mostbet36836.online]https://mostbet36836.online[/url]
mostbet_rvsn –
mostbet oyin statistikasi [url=http://mostbet42672.help/]http://mostbet42672.help/[/url]
mostbet_nnsn –
мостбет обновить apk сегодня [url=http://mostbet91325.help]http://mostbet91325.help[/url]
Davidkab –
Svenska Pharma: Svenska Pharma – Svenska Pharma
pereplanirovka kvartir_slot –
Слушайте кто ремонт затеял Хотел стену снести между комнатами Разрешения эти дурацкие Потратил кучу времени впустую Короче, нашел наконец нормальных специалистов — перепланировка квартир с полным пакетом документов И чертежи сделали В общем, там и примеры и расценки — согласование перепланировки москва [url=https://pereplanirovka-kvartir-owy.ru]согласование перепланировки москва[/url] Не начинайте без проекта Перешлите тому кто тоже ремонт затеял
mostbet_nwpr –
mostbet теннис ставки [url=http://zakaz.kg/]http://zakaz.kg/[/url]
DanielGes –
https://pharmaciefr.click/# Viagra sans ordonnance 24h Amazon
Davidkab –
buy drugs online: medication in mexico – online pharmacy mexico
DanielGes –
https://svenskapharm.click/# Svenska Pharma
Davidkab –
worldwide pharmacy: farmacia mexicana online – mexican meds
pereplanirovka kvartir_llot –
Слушайте кто ремонт затеял Хотел стену снести между комнатами А тут оказывается столько бумаг Нервов просто не осталось Короче, ребята реально толковые — услуги по согласованию перепланировки в Мосжилинспекции И чертежи сделали В общем, жмите чтобы не потерять — согласование перепланировки москва [url=https://pereplanirovka-kvartir-owy.ru]согласование перепланировки москва[/url] Не начинайте без проекта Перешлите тому кто тоже ремонт затеял
DanielGes –
https://mexicopharmrate.click/# buy drugs online
Davidkab –
hydrocodone mexico pharmacy: mail order pharmacy mexico – mexican pharmacys
mostbet_lhst –
mostbet ile trwa wypłata wygranej [url=mostbet18361.online]mostbet18361.online[/url]
proekt pereplanirovki kvartiri_zrKt –
Ребята кто в Москве Планирую объединить две комнаты в гостиную Уже знакомые налетели на миллион Потратил уйму времени Короче, нашел наконец нормальную контору — проект перепланировки и переустройства квартиры полный пакет Всё согласовали за месяц В общем, вся инфа вот здесь — проект перепланировки квартиры москва [url=https://proekt-pereplanirovki-kvartiry-hmf.ru]проект перепланировки квартиры москва[/url] Не начинайте без проекта Перешлите тому кто ремонт затеял
shkola onlain_yiel –
Слушайте кто перевёл на дистант Задолбала эта обычная школа А ещё эти поборы в классе Перепробовал кучу вариантов Короче, ребята реально толковые — школы дистанционного обучения с индивидуальным подходом Ребёнок занимается дома без нервов В общем, там и программа и отзывы — интернет школы [url=https://shkola-onlajn-krt.ru]https://shkola-onlajn-krt.ru[/url] Не мучайте детей Перешлите другим родителям кто устал от школы
Davidkab –
Svenska Pharma: Svenska Pharma – smГ¤rtstillande munskГ¶lj
mostbet_zgsn –
mostbet установка apk [url=https://mostbet91325.help/]https://mostbet91325.help/[/url]
shkola onlain_ptkr –
Слушайте кто ищет выход Домашка на весь вечер Никакого интереса к знаниям Короче, реально удобный формат учёбы — онлайн обучение для детей в удобном темпе Учителя объясняют доходчиво В общем, там программа и отзывы — online school [url=https://shkola-onlajn-lzn.ru]online school[/url] Хватит мучить себя и ребёнка Перешлите другим родителям
Davidkab –
oximeter apotek: billigt apotek – apotek inloggning
mostbet_zpst –
jak pobrać mostbet na ios [url=https://www.mostbet18361.online]https://www.mostbet18361.online[/url]
shkola onlain_wvOr –
Родители всем привет Учителя со своими закидонами Нервы ни к чёрту у всей семьи Короче, реально крутая система — онлайн школы с зачислением и документами Никаких сборов в 8 утра В общем, там программа и условия — онлайн школы для детей [url=https://shkola-onlajn-vem.ru]онлайн школы для детей[/url] Не мучайте себя и детей Перешлите другим родителям
Davidkab –
farmacias mexicanas: mexican pharmacy las vegas – best mexican pharmacy online
Williamrer –
https://mexicopharmrate.click/# mexico medicine
mostbet_ygsn –
mostbet условия отыгрыша [url=http://mostbet91325.help/]http://mostbet91325.help/[/url]
Davidkab –
mexican online pharmacy: progreso, mexico pharmacy online – mexican pharmacies online drugs
zabori pod kluch v Moskve_lvMr –
Слушайте кто забор ставил Задолбался я уже забор искать То столбы гнутые Короче, мужики с руками из правильного места — заборы под ключ в Москве с гарантией И установили всё чисто В общем, вся инфа вот здесь — забор из профнастила под ключ [url=https://zagorodnii-dom.ru]забор из профнастила под ключ[/url] Не ведитесь на дешёвые предложения Перешлите тому у кого участок
Richardriday –
https://pregabalin.life/# lyrica generic
Williamsmefe –
duloxetine: cymbalta duloxetine – cymbalta duloxetine
mostbet_opMn –
mostbet alternativa [url=https://mostbet78342.help]mostbet alternativa[/url]
aviator_uksi –
aviator facebook page malawi [url=aviator62775.online]aviator62775.online[/url]
Richardriday –
https://cenforce.cheap/# buy cenforce
shkola onlain_hikr –
Народ у кого школьники Каждое утро как каторга Никакого интереса к знаниям Короче, нашли идеальное решение — школа онлайн с индивидуальным расписанием Уроки тогда когда удобно В общем, смотрите сами по ссылке — дистанционное обучение в москве [url=https://shkola-onlajn-lzn.ru]дистанционное обучение в москве[/url] Хватит мучить себя и ребёнка Перешлите другим родителям
Richardriday –
https://pregabalin.life/# lyrica medication
shkola onlain_kiMi –
Слушайте кто устал от обычной школы Вечные двойки и тройки в дневнике Нервный как спичка Короче, реально удобный формат — онлайн школы с зачислением из любого города Аттестат как у всех В общем, сохраняйте себе — онлайн школы с зачислением [url=https://shkola-onlajn-pqs.ru]онлайн школы с зачислением[/url] Хватит мучить себя и ребёнка Перешлите другим родителям
Williamsmefe –
lyrica pregabalin: lyrica price – buy lyrica
Richardriday –
https://cenforce.cheap/# cenforce 200
zabori pod kluch v Moskve_mfMr –
Народ всем привет Обещают одно а по факту другое То материал фуфло Короче, нашел нормальных ребят — производство и монтаж заборов любой сложности И установили всё чисто В общем, там каталог и цены — монтаж заборов под ключ [url=https://zagorodnii-dom.ru]монтаж заборов под ключ[/url] Не ведитесь на дешёвые предложения Перешлите тому у кого участок
Richardriday –
https://modafinil.pro/# where to buy Modafinil legally in the US
Richardriday –
https://cenforce.cheap/# cenforce price
Williamsmefe –
Modafinil for ADHD and narcolepsy: Modafinil for ADHD and narcolepsy – buy Modafinil online USA
mostbet_dhMn –
mostbet box [url=http://mostbet78342.help/]http://mostbet78342.help/[/url]
aviator_ousi –
betting in Malawi aviator [url=https://aviator62775.online/]betting in Malawi aviator[/url]
gryzopodemnoe oborydovanie_dopl –
Предприниматели отзовитесь Обещают сертификаты а по факту Китай То тельферы клинят Короче, нашел нормальных производителей — грузоподъемное оборудование Москва с доставкой Цены ниже чем у перекупов на 20% В общем, там каталог и цены — цепная ручная таль [url=https://tal-elektricheskaya.ru]https://tal-elektricheskaya.ru[/url] Проверяйте производителя по документам Перешлите тому кто ищет оборудование
shkola onlain_ujSr –
Кто устал от обычной школы Каждый день как на работу Вечно больной и уставший Короче, реально удобный и простой — школа онлайн с лицензией и зачислением Учителя настоящие профи В общем, сохраняйте себе — дистанционное обучение в москве [url=https://shkola-onlajn-bxf.ru]https://shkola-onlajn-bxf.ru[/url] Не мучайте себя и детей Перешлите другим родителям
Richardriday –
https://pregabalin.life/# buy lyrica
mostbet_hlEi –
mostbet dollar [url=http://mostbet36602.help]http://mostbet36602.help[/url]
pinup_zzpa –
pinup rasmiy ilova [url=www.pinup24541.help]www.pinup24541.help[/url]
Richardriday –
https://cymbalta.top/# cymbalta for pain
mostbet_adMn –
mostbet bonus la inregistrare [url=http://mostbet78342.help]mostbet bonus la inregistrare[/url]
alkoholizem_ipMl –
Res je težko priznati si, da rabiš pomoč. Potem pa sem izvedel za center in vse se je spremenilo. Govorim o zdravljenju alkoholizma pri Dr Vorobjev centru. Veste, ni lahko, ampak se da premagati. In kar je najpomembneje – lahko ostanete doma. Vse informacije in izkušnje drugih sem podrobno pregledal na spletni strani, posodobljene podatke pa si lahko ogledate tukaj: zdravljenje alkoholizma [url=www.zdravljenjealkoholizma.com]zdravljenje alkoholizma[/url]. Zdaj sem že pol leta trezen in ponosen nase.
Če kogarkoli, ki ga imate radi potrebuje pomoč – najboljša odločitev je poklicati. Držim pesti!
aviator_mysi –
aviator download link [url=http://aviator62775.online]http://aviator62775.online[/url]
Williamsmefe –
lyrica online: cheap pregabalin – lyrica generic
Richardriday –
https://cymbalta.top/# duloxetine
alkoholizem_vhSn –
Pozdravljeni. Že dolgo sem iskal resnično rešitev. Ko gre za odvajanje od alkohola — ni šala. Prijatelj mi je priporočil en center, kjer imajo izkušnje. Govorim o zdravljenju po metodi dr. Vorobjeva. Več informacij je na voljo tu: ambulantno zdravljenje alkoholizma [url=www.alkoholizem-zdravljenje.com]www.alkoholizem-zdravljenje.com[/url] Meni so res pomagali. Prvi korak je vedno najtežji. Ampak ko enkrat najdeš pravo pomoč — vse postane lažje. Več kot vredno je poskusiti. Srečno na tej poti!
Richardriday –
https://cenforce.cheap/# cenforce
mostbet_yyEi –
mostbet depozit muammosi yechimi [url=http://mostbet36602.help/]mostbet depozit muammosi yechimi[/url]
Richardriday –
https://pregabalin.life/# lyrica medication
Williamsmefe –
Modafinil Pro: Modafinil Pro – Modafinil for ADHD and narcolepsy
mostbet_pxEi –
mostbet rasmiy sayti uzbekiston [url=mostbet36602.help]mostbet36602.help[/url]
Richardriday –
https://cymbalta.top/# duloxetine
pinup_xxpa –
pinup yutuqni yechish [url=https://pinup24541.help]https://pinup24541.help[/url]
Richardriday –
https://cymbalta.top/# duloxetine
alkoholizem_veot –
изучение китайского [url=https://www.pandoraopen.ru/2026-06-17/god-ognennoj-loshadi-2026-kakie-sily-dejstvuyut-i-chego-ozhidat/]изучение китайского[/url]
Vivod iz zapoya na domy_skPl –
Слушай, человек просто в штопоре. Как есть — круглосуточный вывод из запоя без отмазок. Тут тебе не частная лавочка. Короче говоря, там все подробно расписано — нарколог на дом вывод из запоя на дому [url=https://vyvod-iz-zapoya-na-domu-voronezh-xrt.ru]нарколог на дом вывод из запоя на дому[/url] Хватит надеяться на авось. Поверьте моему опыту, чем труп из квартиры выносить. Рекомендую эту наркологическую клинику.
Richardriday –
https://pregabalin.life/# buy generic lyrica
Williamsmefe –
duloxetine easy buy: cymbalta – duloxetine easy buy
pinup_ykpa –
pin-up aviator pul yechish [url=https://pinup24541.help/]pin-up aviator pul yechish[/url]
Vivod iz zapoya na domy_sykt –
Сил уже нет, каждое утро одно и то же. Руки опускаются. Наркологическая клиника с выездом — качественный вывод из запоя на дому. Ребята знают свое дело. Короче, вот вам информация — сколько стоит вывод из запоя [url=https://vyvod-iz-zapoya-na-domu-voronezh-bvc.ru]сколько стоит вывод из запоя[/url] Каждая пьянка минус ресурс. Сам через это прошел, чем потом собирать по кускам. Очень советую эту контору.
Richardriday –
https://cenforce.cheap/# buy cheap cenforce
Vivod iz zapoya na domy_kqot –
Представьте ситуацию, куча народу сталкивается. Достали уже эти срывы. В такой теме главное не слушать советы алконавтов из подворотни. Нашел нормальный вариант — выведение из запоя без госпитализации. Там работают толковые врачи. Короче, вот собственно источник — вывод из запоя недорого [url=https://vyvod-iz-zapoya-na-domu-voronezh-kmp.ru]вывод из запоя недорого[/url] Не тяните резину, так как алкоголь — это яд. Проверено на себе.
PatrickLef –
https://farmaciaspain.online/# farmacia online envГo gratis
PatrickLef –
https://medfrance.top/# Acheter Sildenafil 100mg sans ordonnance
GeorgeBAR –
Viagra vente libre pays: Viagra vente libre allemagne – Viagra homme prix en pharmacie sans ordonnance
PatrickLef –
https://farmaciasinreceta.top/# farmacia online espaГ±a envГo internacional
PatrickLef –
https://medsmexican.blog/# mexican medicine store
Vivod iz zapoya na domy_drKr –
Ребята, попал в такую передрягу. Родственник пьет без остановки. Нервов ни у кого нет. Скорая не едет. Короче, единственное что реально помогло — нормальное выведение из запоя капельницей. Откачали за час. В общем, там и контакты и прайс — вывод из запоя на дому недорого [url=https://vyvod-iz-zapoya-na-domu-voronezh-zqw.ru]вывод из запоя на дому недорого[/url] Не тяните. Скиньте кому надо.
GeorgeBAR –
Viagra vente libre pays: Quand une femme prend du Viagra homme – Viagra pas cher paris
PatrickLef –
https://medsmexican.blog/# mexico prescriptions
Vivod iz zapoya na domy_hyki –
Блин народ, такая херня приключилась. Муж пьёт неделю без остановки. Руки опустились. В платную клинику денег нет. Короче, единственное что реально помогло — качественный вывод из запоя на дому. Поставили систему. В общем, смотрите сами по ссылке — срочный вывод из запоя [url=https://vyvod-iz-zapoya-na-domu-voronezh-lnm.ru]срочный вывод из запоя[/url] Не тяните резину. Сохраните себе.
PatrickLef –
https://farmaciasinreceta.top/# farmacias online seguras
Vivod iz zapoya na domy_gbpn –
Товарищи, представляете кошмар — человек уже пятый день под завязку. Соседи звонят в дверь. А скорая не едет. У меня брат так чуть не загнулся. Короче, проверенный способ — качественный вывод из запоя на дому. Примчались за час. В общем, сохраняйте себе на будущее — вывод из запоя на дому цена [url=https://vyvod-iz-zapoya-na-domu-voronezh-jhg.ru]https://vyvod-iz-zapoya-na-domu-voronezh-jhg.ru[/url] Промедление реально убивает. Деньги потом не нужны будут. Перешлите тому кто в беде.
PatrickLef –
https://farmaciasinreceta.top/# farmacia online espaГ±a envГo internacional
GeorgeBAR –
Viagra 100 mg sans ordonnance: SildГ©nafil 100mg pharmacie en ligne – Quand une femme prend du Viagra homme
PatrickLef –
https://medmexico.online/# medicine from mexico
PatrickLef –
https://medfrance.top/# Viagra femme ou trouver
PatrickLef –
https://farmaciaspain.online/# farmacia online barcelona
GeorgeBAR –
farmacias online baratas: п»їfarmacia online espaГ±a – farmacias online seguras
PatrickLef –
https://farmaciasinreceta.top/# farmacia online barata y fiable
Vivod iz zapoya na domy_qami –
Народ выручайте. Жесть просто полная. Близкий человек уже шестой день в завязке. Соседи стучат в дверь. Платные клиники ломят космос. Короче, единственное что реально работает — срочный вывод из запоя круглосуточно. Откачали за час. В общем, вся информация вот здесь — вывод из запоя цены воронеж [url=https://vyvod-iz-zapoya-na-domu-voronezh-fds.ru]вывод из запоя цены воронеж[/url] Каждый час на счету. Перешлите другу в беде.
PatrickLef –
https://medsmexican.blog/# mexico pharmacy
GeorgeexefE –
https://medfrance.top/# SildГ©nafil 100 mg prix en pharmacie en France
PatrickLef –
https://medfrance.top/# Viagra vente libre pays
Vivod iz zapoya na domy_qvOt –
Народ привет. Жесть полная случилась. Брат пьёт без остановки. Жена в истерике. Скорая не приезжает на такие вызовы. Короче, нормальные врачи нашлись — профессиональное выведение из запоя капельницей. Отошёл за полчаса. В общем, смотрите сами по ссылке — вывод из запоя цена [url=https://vyvod-iz-zapoya-na-domu-voronezh-ayu.ru]вывод из запоя цена[/url] Не тяните. Скиньте другу в беде.
Vivod iz zapoya na domy_zjea –
Друзья ситуация. Попал я в переплёт конкретный. Муж просто пропадает. Дети не спят ночами. Платные клиники просят бешеные деньги. Короче, нормальные врачи нашлись — анонимный вывод из запоя без последствий. Приехали через час. В общем, сохраняйте на будущее — анонимный вывод из запоя [url=https://vyvod-iz-zapoya-na-domu-samara-abc.ru]https://vyvod-iz-zapoya-na-domu-samara-abc.ru[/url] Не тяните. Скиньте другу в беде.
GeorgeBAR –
farmacia barata: farmacias online seguras en espaГ±a – farmacia online barata
PatrickLef –
https://farmaciaspain.online/# farmacias online seguras
PatrickLef –
https://farmaciasinreceta.top/# farmacia online espaГ±a envГo internacional
aviator_vnEn –
aviator jogar online [url=https://aviator39517.help/]https://aviator39517.help/[/url]
mostbet_qbkl –
cum depun pe mostbet cu visa [url=https://www.mostbet28014.help]https://www.mostbet28014.help[/url]
mostbet_phMl –
mostbet скачать с сайта [url=https://www.mostbet71905.help]https://www.mostbet71905.help[/url]
pinup_bhoa –
pin-up pul yechish [url=https://pinup24711.help]https://pinup24711.help[/url]
PatrickLef –
https://medmexico.online/# mexipharmacy reviews
Vivod iz zapoya na domy_oysl –
Слушайте что расскажу. Попал я в переплёт. Человек уже четвёртые сутки в штопоре. Соседи стучат в дверь. В диспансер везти — учёт на всю жизнь. Короче, только это и спасло — профессиональное выведение из запоя капельницей. Поставили систему. В общем, жмите чтобы не потерять — помощь вывода запоя [url=https://vyvod-iz-zapoya-na-domu-voronezh-plk.ru]https://vyvod-iz-zapoya-na-domu-voronezh-plk.ru[/url] Не надейтесь на авось. Перешлите тому кому надо.
PatrickLef –
https://medfrance.top/# SildГ©nafil 100 mg sans ordonnance
GeorgeBAR –
order from mexico: pharmacy in mexico that ships to us – mexican medicine store
Vivod iz zapoya na domy_coMa –
Друзья ситуация. Попал я в переплёт конкретный. Близкий не выходит из запоя. Жена в слезах. В диспансер везти — учёт на всю жизнь. Короче, единственное что реально помогло — срочный вывод из запоя круглосуточно. Приехали через час. В общем, вся инфа вот здесь — выведение из запоя на дому нарколог [url=https://vyvod-iz-zapoya-na-domu-samara-ghi.ru]https://vyvod-iz-zapoya-na-domu-samara-ghi.ru[/url] Каждая минута дорога. Перешлите тому кому надо.
PatrickLef –
https://farmaciasinreceta.top/# farmacia en casa online descuento
Waltersnuck –
Viagra homme sans ordonnance belgique [url=https://medfrance.top/#]Viagra homme sans prescription[/url] Viagra homme sans ordonnance belgique
PatrickLef –
https://medfrance.top/# Prix du Viagra en pharmacie en France
aviator_rdEn –
aviator crash online [url=https://www.aviator39517.help]https://www.aviator39517.help[/url]
PatrickLef –
https://farmaciasinreceta.top/# farmacia en casa online descuento
Vivod iz zapoya na domy_czma –
Самарцы всем привет. Столкнулся с такой бедой. Брат пьёт без остановки. Дети не спят ночами. В диспансер везти — учёт на всю жизнь. Короче, нормальные врачи нашлись — вывод из запоя дешево и сердито. Поставили систему. В общем, смотрите сами по ссылке — вывести из запоя недорого на дому [url=https://vyvod-iz-zapoya-na-domu-samara-def.ru]https://vyvod-iz-zapoya-na-domu-samara-def.ru[/url] Не тяните. Скиньте другу в беде.
GeorgeexefE –
https://medfrance.top/# Viagra pas cher livraison rapide france
Waltersnuck –
farmacia online barata [url=https://farmaciaspain.online/#]farmacia en casa online descuento[/url] farmacia online envГo gratis
GeorgeBAR –
farmacia online barata y fiable: farmacia online 24 horas – farmacia online envГo gratis
PatrickLef –
https://medfrance.top/# Viagra pas cher livraison rapide france
mostbet_nxMl –
как скачать mostbet на ios [url=mostbet71905.help]mostbet71905.help[/url]
mostbet_rqkl –
mostbet Balti [url=https://mostbet28014.help/]https://mostbet28014.help/[/url]
pinup_inoa –
pin-up karta orqali depozit qilish [url=http://pinup24711.help/]http://pinup24711.help/[/url]
aviator_loEn –
aviator histórico [url=https://www.aviator39517.help]https://www.aviator39517.help[/url]
PatrickLef –
https://medfrance.top/# Viagra sans ordonnance livraison 24h
Waltersnuck –
farmacia online 24 horas [url=https://farmaciaspain.online/#]farmacias online seguras en espaГ±a[/url] п»їfarmacia online espaГ±a
Vivod iz zapoya na domy_oxPi –
Самарцы всем привет. Попал я в переплёт конкретный. Муж просто пропадает. Дети не спят ночами. Скорая не едет. Короче, единственное что реально помогло — вывести из запоя на дому качественно. Поставили систему. В общем, жмите чтобы не потерять — выведение из запоя на дому нарколог [url=https://vyvod-iz-zapoya-na-domu-samara-pqr.ru]https://vyvod-iz-zapoya-na-domu-samara-pqr.ru[/url] Каждая минута дорога. Скиньте другу в беде.
PatrickLef –
https://medsmexican.blog/# medicine mexico
mostbet_dskl –
mostbet download ios [url=http://mostbet28014.help]mostbet download ios[/url]
mostbet_smMl –
мостбет создать аккаунт [url=http://mostbet71905.help/]http://mostbet71905.help/[/url]
pinup_mooa –
pin up haftalik bonus [url=pinup24711.help]pinup24711.help[/url]
PatrickLef –
https://medsmexican.blog/# mexican rx
GeorgeBAR –
farmacia barata: farmacias online seguras – farmacias online seguras
PatrickLef –
https://medmexico.online/# online mexico pharmacy
Waltersnuck –
order meds from mexico [url=https://medmexico.online/#]buying prescriptions in mexico[/url] mexican pharmacies that ship to us
Pyblichnaya kadastrovaya karta_brkr –
Народ кто с землёй Задолбался я уже искать нормальный сервис Границы посмотреть Короче, единственный сервис который не врет — официальная публичная кадастровая карта с выписками Скачал выписку за секунду В общем, сохраняйте себе — публичная кадастровая карта официальный сайт pkk [url=https://publichnaya-kadastrovaya-karta-ghi.ru]https://publichnaya-kadastrovaya-karta-ghi.ru[/url] Не парьтесь с росреестром Перешлите тому кто ищет участок
mostbet_hqMa –
мостбет актуальное зеркало [url=https://mostbet77382.online/]https://mostbet77382.online/[/url]
PatrickLef –
https://medsmexican.blog/# mexican medicine store
Waltersnuck –
Viagra gГ©nГ©rique sans ordonnance en pharmacie [url=https://medfrance.top/#]Viagra prix pharmacie paris[/url] Prix du Viagra 100mg en France
PatrickLef –
https://medmexico.online/# best mexican pharmacy online
Phillipvalia –
https://frpharmacies.icu/# Viagra 100 mg sans ordonnance
Eugenevok –
Viagra vente libre pays: SildГ©nafil 100 mg sans ordonnance – Viagra sans ordonnance 24h suisse
Carlosaften –
https://frpharmacies.icu/# Viagra gГ©nГ©rique pas cher livraison rapide
Edmundloaro –
mexico pharmacies [url=https://pharmustomex.top/#]mexico prescriptions[/url] mexican rx
Phillipvalia –
https://farmaciabarc.online/# farmacia online envГo gratis
Pyblichnaya kadastrovaya karta_gkOi –
Ребята кто с землей Вечно то данные старые Границы посмотреть Короче, нашел крутой инструмент — публичная кадастровая карта новая с просмотром Проверил обременения В общем, там и карта и данные — реестр земельных участков [url=https://publichnaya-kadastrovaya-karta-mno.ru]https://publichnaya-kadastrovaya-karta-mno.ru[/url] Пользуйтесь нормальной картой Перешлите тому кто ищет участок
mostbet_ymMa –
mostbet бонусы для Кыргызстана [url=www.mostbet77382.online]www.mostbet77382.online[/url]
Edmundloaro –
farmacias online seguras en espaГ±a [url=https://farmaciaes.top/#]farmacia online barata y fiable[/url] farmacia online barata
Phillipvalia –
https://frpharmacies.icu/# Viagra sans ordonnance livraison 24h
Pyblichnaya kadastrovaya karta_inPa –
Здорово, народ Вечно то данные старые Соседей проверить Короче, единственный сервис который не врет — публичная кадастровая карта новая с просмотром Нашел всё за 10 минут В общем, смотрите сами по ссылке — публичной кадастровой карте росреестра [url=https://publichnaya-kadastrovaya-karta-def.ru]https://publichnaya-kadastrovaya-karta-def.ru[/url] Не парьтесь с росреестром Перешлите тому кто ищет участок
Pyblichnaya kadastrovaya karta_iipn –
Люди помогите Вечно то данные неактуальные Кадастровый номер вбить Короче, нашел крутой инструмент — публичная кадастровая карта россии онлайн с обновлениями Проверил обременения В общем, жмите чтобы не потерять — сайт пкк [url=https://publichnaya-kadastrovaya-karta-jkl.ru]https://publichnaya-kadastrovaya-karta-jkl.ru[/url] Не парьтесь с росреестром Перешлите тому кто ищет участок
mostbet_jgMa –
как играть в crash mostbet [url=https://mostbet77382.online]https://mostbet77382.online[/url]
Edmundloaro –
Prix du Viagra en pharmacie en France [url=https://frpharmacies.icu/#]Viagra en france livraison rapide[/url] Le gГ©nГ©rique de Viagra
Phillipvalia –
https://pharmmxus.online/# mexico rx
Eugenevok –
farmacias online seguras: farmacias online seguras – farmacias online seguras
mostbet_jfoa –
mostbet bonus aktiv deyil [url=https://mostbet80398.online]https://mostbet80398.online[/url]
mostbet_syMn –
bonus od depozytu mostbet [url=http://mostbet29665.online/]http://mostbet29665.online/[/url]
mostbet_unKa –
mostbet cz web [url=www.mostbet52410.online]mostbet cz web[/url]
melbet_htpn –
melbet идентификация [url=www.melbet72136.online]www.melbet72136.online[/url]
mostbet_hsSn –
mostbet plinko app [url=https://www.mostbet60008.online]https://www.mostbet60008.online[/url]
Vivod iz zapoya na domy_eqka –
Самарцы всем привет. Столкнулся с такой бедой. Брат пьёт без остановки. Жена в слезах. Платные клиники просят бешеные деньги. Короче, нормальные врачи нашлись — профессиональное выведение из запоя капельницей. Поставили систему. В общем, жмите чтобы не потерять — вывод из запоя анонимно недорого [url=https://vyvod-iz-zapoya-na-domu-samara-jkl.ru]вывод из запоя анонимно недорого[/url] Каждая минута дорога. Скиньте другу в беде.
Carlosaften –
https://frpharmacies.icu/# Sildenafil teva 100 mg sans ordonnance
mostbet_ofKa –
mostbet sázky Česko [url=http://mostbet52410.online/]http://mostbet52410.online/[/url]
mostbet_qtPl –
mostbet фрибет Кыргызстан [url=http://mostbet68204.help/]http://mostbet68204.help/[/url]
Phillipvalia –
https://farmaciaes.top/# farmacias direct
Edmundloaro –
medicine from mexico [url=https://pharmmxus.online/#]mexican rx pharm[/url] mail order pharmacies
Vivod iz zapoya na domy_waol –
Слушайте что расскажу. Жесть случилась полная. Муж просто пропадает. Соседи стучат в дверь. Скорая не едет. Короче, единственное что реально помогло — анонимный вывод из запоя без последствий. Поставили систему. В общем, вся инфа вот здесь — нарколог на дом вывод из запоя на дому [url=https://vyvod-iz-zapoya-na-domu-samara-yza.ru]нарколог на дом вывод из запоя на дому[/url] Не надейтесь на авось. Перешлите тому кому надо.
aviator_kxSt –
aviator apk seguro [url=http://aviator05248.help]aviator apk seguro[/url]
Vivod iz zapoya na domy_meKa –
Народ выручайте. Жесть случилась полная. Человек уже пятые сутки в штопоре. Жена в слезах. Скорая не едет. Короче, только это и спасло — профессиональное выведение из запоя капельницей. Поставили систему. В общем, смотрите сами по ссылке — вывод из запоя анонимно [url=https://vyvod-iz-zapoya-na-domu-samara-bcd.ru]вывод из запоя анонимно[/url] Каждая минута дорога. Перешлите тому кому надо.
aviator_eiEr –
aviator मैच बेटिंग [url=https://www.aviator28045.help]https://www.aviator28045.help[/url]
aviator_etEl –
aviator game list Bangladesh [url=https://aviator31708.help]https://aviator31708.help[/url]
Phillipvalia –
https://pharmustomex.top/# reliable rx pharmacy
Edmundloaro –
farmacia online barata [url=https://farmaciabarc.online/#]farmacia online barata[/url] farmacias online seguras en espaГ±a
Vivod iz zapoya na domy_keel –
Народ в Екбе. Близкий человек в завязке. Дети в школу боятся идти. Наркология платная — деньги выкачивают. В итоге, выручили только эти ребята — недорогой вывод из запоя без предоплаты. Сняли ломку быстро. В общем, сохраните чтобы не искать — вывод из запоя [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-rfj.ru]вывод из запоя[/url] Звоните пока не поздно. Кто в беде — тому пригодится.
Eugenevok –
Viagra pas cher livraison rapide france: Viagra sans ordonnance 24h suisse – Viagra homme prix en pharmacie sans ordonnance
mostbet_deKa –
mostbet instalace app [url=http://mostbet52410.online]http://mostbet52410.online[/url]
Phillipvalia –
https://farmaciabarc.online/# farmacia online barata
Edmundloaro –
mexico online farmacia [url=https://pharmmxus.online/#]hydrocodone mexico pharmacy[/url] mail order pharmacies
mostbet_nymi –
mostbet whatsapp [url=https://mostbet80398.online]mostbet whatsapp[/url]
Phillipvalia –
https://pharmustomex.top/# purple pharmacy
mostbet_nuoi –
mostbet rulet [url=mostbet89142.online]mostbet rulet[/url]
Vivod iz zapoya na domy_ifOr –
Народ выручайте. Столкнулся с такой бедой. Муж просто пропадает. Жена в слезах. Скорая не едет. Короче, нормальные врачи нашлись — вывод из запоя недорого и качественно. Приехали через час. В общем, жмите чтобы не потерять — капельница от запоя на дому круглосуточно [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-xtz.ru]https://vyvod-iz-zapoya-na-domu-ekaterinburg-xtz.ru[/url] Не надейтесь на авось. Скиньте другу в беде.
Edmundloaro –
farmacia barata [url=https://farmaciabarc.online/#]farmacia online envГo gratis[/url] farmacias direct
Phillipvalia –
https://frpharmacies.icu/# Viagra 100mg prix
aviator_ciSt –
aviator mirror [url=https://aviator05248.help]https://aviator05248.help[/url]
Eugenevok –
affordable pharmacy: legitimate mexican pharmacy online – mexican rx pharm
Phillipvalia –
https://farmaciaes.top/# farmacia online espaГ±a envГo internacional
Edmundloaro –
п»їViagra sans ordonnance 24h [url=https://frpharmacies.icu/#]Viagra vente libre pays[/url] Viagra pas cher livraison rapide france
aviator_bkEl –
aviator Bangladesh official site [url=https://aviator31708.help]https://aviator31708.help[/url]
aviator_pqEr –
aviator android app डाउनलोड भारत [url=https://aviator28045.help/]aviator android app डाउनलोड भारत[/url]
mostbet_qzoi –
mostbet depozit geri qayıtdı [url=mostbet89142.online]mostbet89142.online[/url]
NormanGef –
http://saludbridgepharmacy.com/# SaludBridge
aviator_jeSt –
aviator oferta [url=www.aviator05248.help]www.aviator05248.help[/url]
LarryRuilt –
MedNavigator Pharmacy: buying from canadian pharmacies – MedNavigator
mostbet_tjmi –
mostbet istifadə şərtləri [url=https://www.mostbet80398.online]https://www.mostbet80398.online[/url]
Keithhof –
http://saludbridgepharmacy.com/# SaludBridge
NormanGef –
http://mednavigatorpharmacys.com/# MedNavigator Pharmacy
LarryRuilt –
online shopping pharmacy india: indian pharmacy paypal – online pharmacy without prescription
aviator_kzEl –
aviator change email [url=https://www.aviator31708.help]https://www.aviator31708.help[/url]
aviator_qqEr –
aviator पासवर्ड बदलें [url=https://www.aviator28045.help]https://www.aviator28045.help[/url]
Williamfat –
SaludBridge Pharmacy [url=https://saludbridgepharmacy.com/#]SaludBridge[/url] SaludBridge
Keithhof –
http://novaformpharmacy.com/# indian pharmacy online
mostbet_vpmi –
mostbet oyun qaydaları mines [url=http://mostbet80398.online]http://mostbet80398.online[/url]
plinko_pgPa –
plinko scam or legit Bangladesh [url=https://plinko45619.help]https://plinko45619.help[/url]
Vivod iz zapoya na domy_zwKi –
Всем здравствуйте. Отец пьёт без просыпу. Дети всего боятся. Скорая не приедет — не тот случай. Короче, действительно профессиональная бригада — срочное выведение из запоя с препаратами. Приехали за 40 минут. В общем, жмите чтобы не забыть — капельница от запоя екатеринбург [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-pcl.ru]https://vyvod-iz-zapoya-na-domu-ekaterinburg-pcl.ru[/url] Не ждите чуда. Передайте тем, кто в беде.
Keithhof –
http://novaformpharmacy.com/# Online medicine home delivery
Vivod iz zapoya na domy_efor –
Слушайте. Отец не просыхает уже пятый день. Родственники не знают что делать. В диспансер везти — стыд на всю жизнь. Короче, реально помогла эта бригада — вывод из запоя на дому анонимно. Сняли интоксикацию за час. В общем, жмите чтобы не забыть — выведение из запоя екатеринбург [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-gkd.ru]выведение из запоя екатеринбург[/url] Промедление дороже. Кто в беде — тому пригодится.
Keithhof –
http://saludbridgepharmacy.com/# prescriptions from mexico
NormanGef –
http://mednavigatorpharmacys.com/# MedNavigator Pharmacy
LarryRuilt –
MedNavigator Pharmacy: MedNavigator – MedNavigator
Williamfat –
mail order pharmacy india [url=https://novaformpharmacy.shop/#]NovaForm[/url] no prescription needed pharmacy
Vivod iz zapoya na domy_hdkr –
Екатеринбург. Человек в завязке уже почти неделю. Дети плачут. В диспансер тащить — клеймо на всю жизнь. В итоге, спасла только эта контора — выведение из запоя без документов и штампа. Капельницу поставили сразу. В общем, жмите чтобы не забыть — вывод из запоя с выездом [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-bqm.ru]вывод из запоя с выездом[/url] Не откладывайте. Скиньте кому пригодится.
Keithhof –
http://saludbridgepharmacy.com/# SaludBridge
LarryRuilt –
SaludBridge Pharmacy: mexican farmacia – SaludBridge Pharmacy
NormanGef –
https://novaformpharmacy.com/# best india pharmacy
Vivod iz zapoya na domy_mlPl –
Всем привет из Екатеринбурга. Отец не выходит из штопора уже третьи сутки. Родственники места себе не находят. В диспансер тащить — позор на всю жизнь. В итоге, единственные кто взялся без предоплат — вывод из запоя цены доступные. Приехали в течение часа. В общем, жмите чтобы сохранить — вывод из запоя анонимно недорого [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-nws.ru]https://vyvod-iz-zapoya-na-domu-ekaterinburg-nws.ru[/url] Каждый час усугубляет состояние. Может кому-то спасёт жизнь.
Keithhof –
https://novaformpharmacy.com/# top online pharmacy india
Williamfat –
MedNavigator [url=http://mednavigatorpharmacys.com/#]MedNavigator Pharmacy[/url] MedNavigator Pharmacy
mostbet_skkr –
mostbet natijalar [url=www.mostbet44945.help]www.mostbet44945.help[/url]
LarryRuilt –
best online pharmacy india: NovaForm – medstore online pharmacy
NormanGef –
https://novaformpharmacy.shop/# п»їlegitimate online pharmacies india
alkoholizem_lhEt –
Pozdrav iz moje izkusnje. Upam, da bo komu koristilo. Dolga leta sem se boril s to odvisnostjo. Potem pa sem na spletu nasel zdravljenje alkoholizma pri Dr Vorobjevu. Mislil sem, da je to se ena prevara. Ampak sem dal priloznost. In zdaj, po nekaj mesecih, lahko recem, da je bilo to prelomnica v mojem zivljenju. Sam sem preucil celoten program in vsi kljucni podatki so na voljo na tej povezavi: odvajanje od alkohola [url=http://www.alkoholizmazdravljenje.com]odvajanje od alkohola[/url]. Ni lahko priznati, ampak se splaca.
Ce se vi ali kdo od vasih bliznjih sooca s tem — resnicno priporocam, da preberete. Nikoli ni prepozno za nov zacetek.
mostbet_vgOn –
mostbet ставки Кыргызстан [url=https://mostbet18868.online]mostbet ставки Кыргызстан[/url]
mostbet_jcPn –
lucky jet игра мостбет [url=https://mostbet69815.online]lucky jet игра мостбет[/url]
mostbet_ylkt –
мостбет promo code [url=www.mostbet06394.help]www.mostbet06394.help[/url]
Keithhof –
http://saludbridgepharmacy.com/# medications can i buy mexico
plinko_dkPa –
plinko mines deposit [url=https://plinko45619.help]https://plinko45619.help[/url]
LarryRuilt –
world pharmacy india: NovaForm – top online pharmacy
NormanGef –
https://novaformpharmacy.shop/# india online pharmacy
Keithhof –
http://novaformpharmacy.com/# best india pharmacy
NormanGef –
https://mednavigatorpharmacys.com/# MedNavigator
Keithhof –
https://saludbridgepharmacy.shop/# SaludBridge Pharmacy
plinko_zwPa –
plinko scam or legit Bangladesh [url=https://plinko45619.help/]https://plinko45619.help/[/url]
Williamfat –
MedNavigator Pharmacy [url=https://mednavigatorpharmacys.shop/#]MedNavigator Pharmacy[/url] MedNavigator
mostbet_zskr –
mostbet ios app yuklab olish [url=www.mostbet44945.help]mostbet ios app yuklab olish[/url]
LarryRuilt –
SaludBridge Pharmacy: SaludBridge Pharmacy – can i order online from a mexican pharmacy
Keithhof –
http://saludbridgepharmacy.com/# SaludBridge
NormanGef –
https://saludbridgepharmacy.shop/# SaludBridge
mostbet_ieOn –
mostbet lucky jet стратегия [url=https://www.mostbet18868.online]https://www.mostbet18868.online[/url]
mostbet_hukr –
mostbet to‘lov rekvizitlari [url=https://www.mostbet44945.help]https://www.mostbet44945.help[/url]
mostbet_jkPn –
мостбет кэшбэк казино [url=https://mostbet69815.online]https://mostbet69815.online[/url]
mostbet_lpkt –
мостбет вход в личный кабинет [url=https://mostbet06394.help]мостбет вход в личный кабинет[/url]
Keithhof –
https://mednavigatorpharmacys.shop/# MedNavigator Pharmacy
LarryRuilt –
online shopping pharmacy india: india online pharmacy – reliable online pharmacy
NormanGef –
https://saludbridgepharmacy.com/# SaludBridge Pharmacy
mostbet_mcOn –
мостбет акции [url=http://mostbet18868.online/]http://mostbet18868.online/[/url]
Williamfat –
best india pharmacy [url=https://novaformpharmacy.shop/#]NovaForm Pharmacy[/url] online pharmacy no prescription
melbet_dmpi –
melbet live casino [url=https://melbet64624.online]https://melbet64624.online[/url]
mostbet_vvSn –
mostbet слоты играть [url=https://www.mostbet05859.online]https://www.mostbet05859.online[/url]
melbet_cxSr –
melbet установка apk [url=melbet30147.online]melbet установка apk[/url]
aviator_qhEn –
betting in Malawi aviator [url=www.aviator07349.online]betting in Malawi aviator[/url]
Keithhof –
https://mednavigatorpharmacys.shop/# MedNavigator Pharmacy
LarryRuilt –
best india pharmacy: india pharmacy mail order – trustworthy online pharmacy
mostbet_rjkt –
мостбет приложение [url=https://mostbet06394.help/]мостбет приложение[/url]
mostbet_hqPn –
мостбет сом вывод [url=https://mostbet69815.online]https://mostbet69815.online[/url]
NormanGef –
https://saludbridgepharmacy.com/# SaludBridge Pharmacy
alkoholizem_khSl –
Pozdravljeni, dragi moji. Rad bi delil svojo zgodbo. Alkohol je dolgo casa vodil moje zivljenje. Potem pa sem na spletu naletel na resitev. Govorim o ambulantnem zdravljenju alkoholizma pri Dr Vorobjev centru. Sprva nisem verjel. Ampak sem se odlocil за ta korak in koncno sem spet jaz. Sam sem preucil celoten program in vsi kljucni podatki so na voljo na tej povezavi: Dr Vorobjev center [url=http://www.odvajanje-od-alkoho.com]http://www.odvajanje-od-alkoho.com[/url] Odvisnost od alkohola ni znak sibkosti.
Ce vas partner potrebuje pomoc — to je lahko odlocilni korak. Srecno na vasi poti!
Keithhof –
http://novaformpharmacy.com/# п»їlegitimate online pharmacies india
LarryRuilt –
best online pharmacy india: NovaForm – foreign online pharmacy
NormanGef –
http://mednavigatorpharmacys.com/# MedNavigator
Keithhof –
https://novaformpharmacy.com/# best online pharmacy india
Williamfat –
best mexican online pharmacy [url=http://saludbridgepharmacy.com/#]SaludBridge[/url] SaludBridge
mostbet_yoSr –
мостбет Джалал-Абад [url=http://mostbet44719.online]http://mostbet44719.online[/url]
LarryRuilt –
SaludBridge Pharmacy: SaludBridge Pharmacy – mexican pharmacys
mostbet_kjkl –
mostbet как получить фрибет [url=https://mostbet86491.online]https://mostbet86491.online[/url]
melbet_xmEa –
мелбет promo code [url=http://melbet13861.online/]http://melbet13861.online/[/url]
NormanGef –
https://novaformpharmacy.shop/# india pharmacy mail order
Keithhof –
https://saludbridgepharmacy.com/# SaludBridge Pharmacy
aviator_wfEn –
aviator provably fair [url=https://aviator07349.online]https://aviator07349.online[/url]
melbet_kzpi –
melbet bd official [url=www.melbet64624.online]melbet bd official[/url]
mostbet_ngSn –
мостбет ставки онлайн [url=http://mostbet05859.online]http://mostbet05859.online[/url]
melbet_ofSr –
melbet ошибка входа [url=https://www.melbet30147.online]https://www.melbet30147.online[/url]
LarryRuilt –
buy prescription drugs from india: NovaForm Pharmacy – express scripts mail order pharmacy
TimothyDah –
https://farmaciabarca.top/# farmacia online 24 horas
TravisHof –
https://mxhealthrate.icu/# mexican pharmacy near me
Ernestbunda –
pharmacy in mexico online [url=https://mexicohealth.top/#]best online mexican pharmacy[/url] mexican pharmacies that ship to the united states
aviator_hwEn –
aviator community malawi [url=aviator07349.online]aviator community malawi[/url]
Jeffreyrep –
SildГ©nafil Teva 100 mg acheter: Viagra sans ordonnance 24h Amazon – SildГ©nafil Teva 100 mg acheter
Alfreduteme –
https://francepharmacies.icu/# Viagra sans ordonnance livraison 48h
Narkologicheskaya pomosh_yrPr –
Доброго времени суток. Мой брат окончательно ушёл в запой. Соседи шепчутся за спиной. Частные центры ломят космические суммы. Итог, единственные, кто взялся без нервотрёпки — частная наркологическая помощь с выездом. Врач осмотрел и начал капельницу. В общем, телефон и цены тут — частная наркологическая помощь [url=https://narkologicheskaya-pomoshh-nizhnij-novgorod-ksc.ru]https://narkologicheskaya-pomoshh-nizhnij-novgorod-ksc.ru[/url] Звоните прямо сейчас. Вдруг это поможет кому-то.
melbet_qvSr –
мелбет о деньги [url=https://www.melbet30147.online]мелбет о деньги[/url]
mostbet_zeSn –
crash мостбет [url=mostbet05859.online]mostbet05859.online[/url]
melbet_rmpi –
melbet first deposit bonus [url=www.melbet64624.online]www.melbet64624.online[/url]
TravisHof –
https://mexicohealth.top/# online pharmacies
TimothyDah –
https://mexicohealth.top/# mexico meds
mostbet_skSr –
mostbet crash коэффициенты [url=www.mostbet44719.online]www.mostbet44719.online[/url]
melbet_onEa –
мелбет кыргызстан скачать android [url=https://www.melbet13861.online]мелбет кыргызстан скачать android[/url]
mostbet_wsSr –
mostbet кэшбэк условия [url=https://mostbet44719.online/]mostbet кэшбэк условия[/url]
TravisHof –
https://farmaciabarca.top/# farmacias online seguras
Jeffreyrep –
farmacias online baratas: farmacias direct – farmacia online barata
TimothyDah –
http://mexicanpharmfast.online/# mexican pharmacy menu
Vivod iz zapoya na domy_lvKt –
Доброго вечера. Просто ужас. Соседи уже стучат в дверь. В наркологию везти — страшно. Короче говоря, единственные кто быстро приехал и помог — вывод из запоя на дому анонимно. К ночи человек пришёл в себя. В общем, не потеряйте, пригодится — прокапаться от алкоголя цены [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-mfk.ru]https://vyvod-iz-zapoya-na-domu-ekaterinburg-mfk.ru[/url] Не ждите. Вдруг кому-то это спасёт жизнь.
Kapelnica ot zapoya_umpr –
Доброго времени. Ситуация жёсткая. Дети испуганы. В бесплатную наркологию — страшно идти. Короче, реально помогли эти врачи — прокапаться от алкоголя недорого. К утру человек пришёл в себя. В общем, не потеряйте — запой капельница нарколог [url=https://kapelnica-ot-zapoya-nizhnij-novgorod-icy.ru]запой капельница нарколог[/url] Звоните прямо сейчас. Вдруг это поможет.
mostbet_rmkl –
мостбет новое зеркало [url=http://mostbet86491.online/]http://mostbet86491.online/[/url]
TravisHof –
https://mexicohealth.top/# online mexican pharmacies
Vivod iz zapoya na domy_mkOa –
Здорова, ребята. Брат совсем потерял человеческий облик. Родственники не знают куда бежать. Платная наркология — как счёт за квартиру. Короче, единственные кто приехал без предоплаты — помощь нарколога на дому быстро. Сняли ломку и нормализовали давление. В общем, цены и телефон тут — прокапаться на дому от алкоголя цена [url=https://vyvod-iz-zapoya-na-domu-ekaterinburg-dyz.ru]https://vyvod-iz-zapoya-na-domu-ekaterinburg-dyz.ru[/url] Не откладывайте. Киньте ссылку нуждающимся.
Jeffreyrep –
mexican pharmacy what to buy: buy drugs online – mexico medication
melbet_scSn –
melbet crash bonus [url=https://melbet83310.help/]https://melbet83310.help/[/url]
mostbet_rePt –
mostbet повторная отправка кода [url=https://mostbet26814.help]https://mostbet26814.help[/url]
Alfreduteme –
https://francepharmacies.icu/# Viagra générique sans ordonnance en pharmacie
TimothyDah –
https://francepharmacies.icu/# Viagra femme sans ordonnance 24h
melbet_eoEa –
melbet crash играть [url=https://www.melbet13861.online]https://www.melbet13861.online[/url]
pinup_lssn –
pin up blokirovkani chetlab o‘tish [url=https://www.pinup51879.help]https://www.pinup51879.help[/url]
melbet_zcOl –
melbet handicap [url=http://melbet90383.help]http://melbet90383.help[/url]
mostbet_dxPl –
mostbet ordinar [url=https://www.mostbet06693.help]https://www.mostbet06693.help[/url]
Ernestbunda –
farmacia en casa online descuento [url=http://farmaciaesptop.online/#]farmacia online envГo gratis[/url] farmacia online madrid
TravisHof –
http://farmaciaesptop.online/# farmacia online envГo gratis
Vivod iz zapoya na domy_fjSr –
Всем привет из НН. Мой отец уже четвёртый день в запое. Соседи уже начали коситься. В диспансер тащить — клеймо на всю жизнь. Короче, выручила эта служба — анонимное выведение из запоя с капельницей. Сняли абстинентный синдром. В общем, жмите, чтобы не потерять — вывод из запоя круглосуточно цены [url=https://vyvod-iz-zapoya-na-domu-nizhnij-novgorod-pwj.ru]https://vyvod-iz-zapoya-na-domu-nizhnij-novgorod-pwj.ru[/url] Не тяните время. Киньте ссылку нуждающимся.
mostbet_bqkl –
mostbet история ставок [url=https://mostbet86491.online/]https://mostbet86491.online/[/url]
Jeffreyrep –
farmacias online seguras en espaГ±a: farmacia online envГo gratis – farmacia online barata y fiable
TimothyDah –
http://farmaciaestop.online/# farmacia online madrid
TravisHof –
https://francepharmacies.icu/# Viagra sans ordonnance pharmacie France
Jeffreyrep –
order medication from mexico: best online mexican pharmacy – online pharmacies
MillardPep –
https://generixpharm.shop/cytotec-misoprostol-guidelines/# GenerixPharm
TimothyDah –
http://farmaciaestop.online/# farmacia online barata y fiable
melbet_yhSn –
melbet coupon de pari [url=melbet83310.help]melbet83310.help[/url]
TravisHof –
http://farmaciaesptop.online/# farmacia online envГo gratis
mostbet_buPt –
mostbet обновить apk сегодня [url=http://mostbet26814.help]http://mostbet26814.help[/url]
Vivod iz zapoya v stacionare_xuka –
Всем привет. Близкий человек потерял контроль над собой. Домашние условия не помогают. Скорая не решает проблему глобально. Короче, единственное, что реально сработало — анонимный вывод из запоя в стационаре. Выписали без симптомов ломки. В общем, не потеряйте контакты — прокапаться в стационаре [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-knd.ru]https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-knd.ru[/url] Звоните прямо сейчас. Перешлите тем, кто в отчаянии.
pinup_gpsn –
pinup haftalik bonus [url=https://pinup51879.help/]pinup haftalik bonus[/url]
Ernestbunda –
Viagra 100 mg sans ordonnance [url=https://francepharmacies.icu/#]Viagra 100 mg sans ordonnance[/url] Viagra pas cher inde
TimothyDah –
https://francepharmacies.icu/# Viagra homme prix en pharmacie sans ordonnance
Jeffreyrep –
Viagra pas cher inde: Prix du Viagra en pharmacie en France – SildГ©nafil 100 mg sans ordonnance
TravisHof –
https://francepharmacies.icu/# SildГ©nafil 100mg pharmacie en ligne
mostbet_oyPl –
mostbet rasmiy sayti uzbekiston [url=http://mostbet06693.help]http://mostbet06693.help[/url]
melbet_xaSn –
melbet paris en fcfa [url=http://melbet83310.help]http://melbet83310.help[/url]
mostbet_kbPt –
мостбет сменить номер [url=http://mostbet26814.help/]http://mostbet26814.help/[/url]
TravisHof –
https://farmaciabarca.top/# farmacia online espaГ±a envГo internacional
TimothyDah –
http://farmaciaestop.online/# farmacia online madrid
MillardPep –
https://generixpharm.shop/clomid-clomiphene-mechanisms/# where to buy clomid without dr prescription
Vivod iz zapoya na domy_ivmn –
Здорова, народ. Беда пришла в семью. Мать плачет. Платная клиника — деньги выкачивают. Короче, спасла только эта бригада — выведение из запоя на дому анонимно. Приехали через 35 минут. В общем, не потеряйте — вывод из запоя с выездом на дом [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-zqe.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-zqe.ru[/url] Каждый час ухудшает состояние. Вдруг это спасёт чью-то жизнь.
EduardoVow –
payday loans that approve everyone: PaydayBestHub – п»їpayday loans
pinup_ggsn –
pin-up bugun rasmiy sayt [url=https://pinup51879.help]https://pinup51879.help[/url]
Narkologicheskaya pomosh_bnEr –
Всем здравствуйте. Беда случилась. Соседи уже стучат в стену. Платная клиника — огромные счета. Итог, единственные, кто быстро отреагировал — наркологическая помощь недорого в Нижнем Новгороде. Врач осмотрел и поставил капельницу. В общем, жмите, чтобы сохранить — наркологическая клиника недорого [url=https://narkologicheskaya-pomoshh-nizhnij-novgorod-fql.ru]наркологическая клиника недорого[/url] Каждый час усугубляет ситуацию. Отправьте тем, кто рядом с бедой.
mostbet_atEl –
mostbet подтверждение личности [url=www.mostbet88517.online]www.mostbet88517.online[/url]
MichaelBlone –
https://paydaybesthub.shop/# quickest payday loans online
mostbet_glPl –
mostbetdan pul yechish [url=http://mostbet06693.help]http://mostbet06693.help[/url]
Ralphvieme –
http://paydaybesthub.com/# paycheck advance online
melbet_owOl –
melbet inscriere [url=https://melbet90383.help/]https://melbet90383.help/[/url]
EduardoVow –
cash advance online no fax: PaydayBestHub – payday loans online instant approval
mostbet_ouPt –
mostbet проверка документов [url=http://mostbet73296.online]http://mostbet73296.online[/url]
MichaelBlone –
http://paydaybesthub.com/# payday cash advance online
Vivod iz zapoya na domy_qlen –
Доброго времени суток. Мой отец уже четвёртые сутки в запое. Мать на грани истерики. В государственную наркологию — страшно и стыдно. Короче, реально профессиональные врачи — недорогой вывод из запоя в Санкт-Петербурге. Через пару часов человек пришёл в себя. В общем, вся инфа и контакты по ссылке — вывод из алкогольного запоя нарколог24 [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-abc.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-abc.ru[/url] Звоните прямо сейчас. Киньте ссылку тем, кто в беде.
Vivod iz zapoya na domy_tcet –
Салют, Питер. Отец не выходит из штопора. Мать в депрессии. В государственный диспансер — табу. В итоге, выручила эта служба — недорогой вывод из запоя в Санкт-Петербурге. Сняли острую интоксикацию. В общем, жмите, чтобы сохранить — вывод из запоя на дому спб [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-mnq.ru]вывод из запоя на дому спб[/url] Звоните прямо сейчас. Перешлите тем, кто рядом с бедой.
Vivod iz zapoya na domy_dkEr –
Здорово, Питер. Отец не выходит из штопора. Мать на грани нервного срыва. Скорая не реагирует на такие вызовы. Короче, реально крутые врачи попались — срочный вывод из запоя с выездом. Сняли острую интоксикацию. В общем, вся инфа и контакты по ссылке — вывод из запоя на дому спб [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-jfw.ru]вывод из запоя на дому спб[/url] Не ждите чуда. Перешлите тем, кто рядом с бедой.
MillardPep –
https://generixpharm.shop/seroquel-quetiapine-profile/# seroquel
Ralphvieme –
https://paydaybesthub.online/# best approval payday loans
EduardoVow –
get cash instantly online: Payday Best Hub – always approved payday loans
Carrollthums –
instant cash advance no fee [url=https://paydaybesthub.shop/#]PaydayBestHub[/url] everyone approved payday loan
MichaelBlone –
http://paydaybesthub.com/# payday loans online instant approval
mostbet_uwEa –
mostbet tətbiq [url=https://mostbet10542.help/]mostbet tətbiq[/url]
mostbet_hyOr –
mostbet бонус за регистрацию [url=http://mostbet01460.online/]mostbet бонус за регистрацию[/url]
melbet_piOl –
cum sa ma inregistrez pe melbet [url=https://melbet90383.help]https://melbet90383.help[/url]
MichaelBlone –
http://paydaybesthub.com/# most reputable payday loans
mostbet_csEl –
mostbet официальный сайт Кыргызстан [url=mostbet88517.online]mostbet официальный сайт Кыргызстан[/url]
MillardPep –
https://generixpharm.shop/lasix-furosemide-protocols/# lasix for sale
Ralphvieme –
http://paydaybesthub.com/# payday loans direct lenders
EduardoVow –
online payday loans today: PaydayBestHub – everyone approved payday loan
MichaelBlone –
https://paydaybesthub.com/# payday loans
Carrollthums –
payday loans no interest [url=http://paydaybesthub.com/#]Payday Best Hub[/url] cash advance online no fax
mostbet_nlPt –
мостбет правила бонуса [url=mostbet73296.online]mostbet73296.online[/url]
mostbet_esSa –
mostbet çıxarış təsdiqi [url=www.mostbet84891.online]mostbet çıxarış təsdiqi[/url]
Vivod iz zapoya na domy_rjPa –
Здорова, Питер. Мой брат уже шестой день в запое. Мать плачет целыми днями. В бесплатный диспансер — стыд на всю жизнь. Итог, единственные, кто приехал без лишних вопросов — выведение из запоя на дому анонимно. Сняли абстинентный синдром. В общем, жмите, чтобы сохранить — вывода из запоя 24 [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-xyt.ru]вывода из запоя 24[/url] Не тяните время. Киньте ссылку нуждающимся.
MichaelBlone –
https://paydaybesthub.shop/# paycheck advance online
Ralphvieme –
https://paydaybesthub.shop/# payday loans online no credit
EduardoVow –
best acceptance payday loans: Payday Best Hub – most trusted payday loans online
mostbet_bbEl –
mostbet букмекер 2026 [url=https://www.mostbet88517.online]https://www.mostbet88517.online[/url]
mostbet_waPt –
мостбет баскетбол ставки [url=http://mostbet73296.online/]http://mostbet73296.online/[/url]
Vivod iz zapoya na domy_otpr –
Салют, земляки. Брат снова ушёл в завязку. Мать в отчаянии. Платная клиника — бешеные цены. Короче, единственные, кто быстро приехал — выведение из запоя на дому анонимно. Сняли абстинентный синдром. В общем, цены и телефон тут — выведение из запоя на дому [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-hnd.ru]выведение из запоя на дому[/url] Не ждите. Вдруг это спасёт чью-то жизнь.
MichaelBlone –
https://paydaybesthub.com/# cash advance online no fax
MillardPep –
https://generixpharm.shop/lasix-furosemide-protocols/# lasix 40mg
mostbet_mfOr –
мостбет электронный кошелек [url=https://mostbet01460.online/]мостбет электронный кошелек[/url]
mostbet_zzEa –
mostbet statistika bölməsi [url=http://mostbet10542.help/]mostbet statistika bölməsi[/url]
Ralphvieme –
http://paydaybesthub.com/# instant cash advance no fee
Carrollthums –
best payday advance loans online [url=https://paydaybesthub.com/#]Payday Best Hub[/url] loans till payday everyone approved
EduardoVow –
loans till payday everyone approved: get cash instantly online – payday loans no credit check
Vivod iz zapoya na domy_avEn –
Здорова, Питер. Близкий человек снова сорвался в пьянку. Родственники просто в шоке. Скорая отказывается приезжать. Короче, спасла эта бригада — выведение из запоя на дому анонимно. Приехали через 25 минут. В общем, жмите, чтобы сохранить — вывод из алкогольного запоя нарколог 24 [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-vkx.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-vkx.ru[/url] Каждый час ухудшает состояние. Перешлите тем, кто рядом с бедой.
pufvibxgz –
Depois de se registrar neste cassino, você receberá 20 rodadas grátis para usar no slot Gates of Olympus da Pragmatic Play. O requisito de aposta para esta promoção é de 35x e deve ser concluído em 5 dias. Depois de se registrar neste cassino, você receberá 20 rodadas grátis para usar no slot Gates of Olympus da Pragmatic Play. O requisito de aposta para esta promoção é de 35x e deve ser concluído em 5 dias. Mesmo ao encontrar uma plataforma pagando, é recomendável começar com o menor valor possível, que seja suficiente para a sua diversão, para um primeiro teste. Diferentes casas se destacam dependendo do tipo de aposta que você faz. Nossa análise identificou as melhores plataformas para cada modalidade. Confira: Os cassinos online geralmente oferecem bônus de rodadas grátis em slots selecionados. Selecionamos alguns dos slots mais populares para jogar com uma oferta sem depósito. Confira nossa lista!
http://www.brouilette.com/archives/277875
Diferentes casas se destacam dependendo do tipo de aposta que você faz. Nossa análise identificou as melhores plataformas para cada modalidade. Confira: 17 10 2025 às 13:30 Somado a isso, a plataforma de jogos oferece cashback de até R$ 2500, calculado com base no saldo negativo das apostas feitas em slots. Diferentes casas se destacam dependendo do tipo de aposta que você faz. Nossa análise identificou as melhores plataformas para cada modalidade. Confira: Diferentes casas se destacam dependendo do tipo de aposta que você faz. Nossa análise identificou as melhores plataformas para cada modalidade. Confira: Este slot de 243 vias da Microgaming é baseado na popular série de TV Game of Thrones. Neste slot você pode escolher sua casa favorita e viajar pelos Sete Reinos de Westeros para conquistar o Trono de Ferro junto com grandes vitórias. Este jogo de caça-niqueis tem símbolos especiais e rodadas grátis para aumentar suas chances de ganhar.
MichaelBlone –
https://paydaybesthub.shop/# online payday loans today
Ralphvieme –
https://paydaybesthub.shop/# instant cash advance no fee
mostbet_isEa –
mostbet balans artırma üsulları [url=http://mostbet10542.help]http://mostbet10542.help[/url]
mostbet_iiOr –
aviator игра мостбет [url=www.mostbet01460.online]aviator игра мостбет[/url]
EduardoVow –
instant cash advance online: best payday advance loans online – payday loans online instantly
mostbet_wwSa –
mostbet cashback faiz [url=https://mostbet84891.online]https://mostbet84891.online[/url]
xjdawehzb –
This is another great feature about this app. Here, if you wish, you can separate the video and sound from each other. Depending on the situation and when, where and why you want it, you might sometimes want a video without sound or a sound from a separate video without the video itself. Both these actions can be performed with this xvideostudio app. You can also add your favourite background music to the videos while creating one. Therefore, this can be mentioned as another great benefit you can take from this app. Your program review has been submitted successfully. Best Video Editor With Songs – PixPoz XVideoStudio Video Editor stands out among countless video editing applications due to its perfect blend of functionality and usability. Whether you’re creating a simple video for family and friends or producing content for your brand, this app provides all the tools you need in one convenient package.
https://www.glossytech.com/66/betbuffoon-een-eerlijke-review-van-het-online-casinospel-voor-spelers-uit-nederland/
Visually, Big Bass Bonanza delivers a laid-back, underwater vibe. Shocking for a fish themed slot, right? Big Bass Bonanza is the blueprint for the next 20 (and counting) instalments, so it makes sense that it’s nothing too flashy. Pragmatic Play has engineered Bigger Bass Bonanza with an intuitive and user-friendly interface. The game is perfectly optimised for desktop and mobile devices, ensuring seamless play across platforms. UK players will appreciate the crisp visuals and smooth animations that make each spin immersive. The control panel is clearly laid out with options for adjusting bet sizes, activating autoplay, and accessing game information such as paylines and paytables. The Big Bass Bonanza demo offers a risk-free way to understand the machine’s features and strategies, similar to Big Bass Splash casino games.
MichaelBlone –
https://paydaybesthub.online/# most trusted payday loans online
aviator_sbmi –
aviator how to deposit mpamba [url=http://aviator33280.online/]http://aviator33280.online/[/url]
melbet_sjmi –
melbet install apk [url=http://melbet55504.online]http://melbet55504.online[/url]
melbet_pcet –
melbet crash чӣ гуна бозӣ кардан [url=https://melbet75116.online/]https://melbet75116.online/[/url]
Ralphvieme –
https://paydaybesthub.com/# payday loans that approve everyone
mostbet_gzml –
mostbet punkty lojalnościowe [url=https://www.mostbet74029.online]mostbet punkty lojalnościowe[/url]
MillardPep –
https://generixpharm.shop/# Cytotec
EduardoVow –
instant cash advance no fee: most reliable payday loan company – payday loans online
fsiafmqzl –
With 91% of businesses now using video for marketing, editors must be fluent in both storytelling and technical execution. In practice, that means more than cutting footage—it’s crafting platform-specific hooks for TikTok, vertical-friendly compositions for Instagram Reels, or retention-focused editing for YouTube. Skilled agencies will surface editors who can adapt to 4K production workflows, optimize for under-two-minute engagement, and master color grading for multi-device viewing. ADMEC Multimedia is a professional Video Editing Institute in Delhi offers training for video editing courses in India by experts. In the advanced Video Editing classes, training is given on high-end apple machines by best of the experienced industry experts. Avoid using overly complex or confusing terms when naming your video editing company, as they can be hard to remember. Steer clear of names similar to existing businesses in the industry to avoid legal issues and ensure that your brand remains distinct and recognizable.
https://www.kiarajewelryjapan.com/hot-chilli-slot-recensione-del-gioco-3-hot-chillies-by-3-oaks/
Despite being an unofficial APK, the x.video editor app provides enough tools for quick and lightweight video edits. It is a functional basic x video editor designed for users who want fast results without the complexity of full-featured editors. The XVideoStudio video editor APK is built for users who want a quick and lightweight way to edit videos. Its small size, offline functionality, and simple tools make it best suited for casual editing tasks. XVideoStudio Video Editor APK is compatible with a wide range of devices, ensuring that you can enjoy a smooth editing experience on your smartphone or tablet. The app is optimized for different screen sizes and resolutions, making it perfect for editing on the go. – You can splice or merge video, convert video into MP3 file, collage and loop video clips easily.
MichaelBlone –
https://paydaybesthub.com/# best payday advance loans online
mostbet_pwSa –
mostbet hesab dondurmaq [url=www.mostbet84891.online]mostbet hesab dondurmaq[/url]
melbet_hdml –
melbet зеркало скачать [url=melbet58323.online]melbet58323.online[/url]
qepqndbwf –
As much as I love Premiere Pro, I can’t justify spending £20+ a month for software I use fairly infrequently. When I first wrote this article, I would’ve said that I was going to make the switch to InShot for desktop. However, after trying to use it a few times to edit simple videos, I ended up using a mixture of iMovie and Canva. Whilst Inshot seems most similar to CapCut, I found their desktop app too clunky and laggy, as it works almost like a scaled-up version of their mobile version. Podcastle stands out as a top alternative to CapCut, offering a comprehensive suite of features designed to simplify audio and video production for creators of all levels. With a focus on innovation and user-friendliness, Podcastle integrates AI-powered tools to enhance your content creation experience.
https://greencare24.pl/2026/04/08/divine-fortune-een-diepgaande-slot-review-gericht-op-spelers-in-nederland/
The Big Bass Bonanza demo has a generous starting balance of $100k in virtual credit. I played like a high-roller at first to see if spending big was a winning strategy, but I found that keeping my bets in the medium-low range let me play longer with more wins over time. Before you start fishing, make sure to choose a stake that suits your playing preferences. We’re confident that doing so won’t be difficult, as Big Bass Bonanza offers broad wagering options. It is possible to bet up to ten coins per line, which coupled with a coin value ranging from £0.01 to £2.50 means they may spend between £0.10 and £250 on every spin. We advise players to keep in mind the title’s volatile nature when placing their bets. As the name suggests, this slot is bigger and better than its predecessor. It doubles the winning potential and adds 2 extra paylines as well as bigger fish to fry on the reels. The Bigger Bass Bonanza slot also looks better while retaining the features of the original.
Ralphvieme –
http://paydaybesthub.com/# payday loans no credit check
EduardoVow –
payday loans online with instant approval: instant cash advance no fee – payday loans online no credit
MichaelBlone –
https://paydaybesthub.shop/# instant cash advance no fee
Vivod iz zapoya na domy_jiEa –
Привет, народ. Близкий человек потерял контроль. Мать места себе не находит. Платная клиника — выкачивает деньги. Итог, выручила эта служба — выведение из запоя на дому анонимно. К утру человек пришёл в норму. В общем, жмите, чтобы не потерять — вывод из запоя в спб [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-rpl.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-rpl.ru[/url] Не тяните. Перешлите тем, кто в беде.
aviator_cvmi –
aviator download free [url=http://aviator33280.online/]http://aviator33280.online/[/url]
Ralphvieme –
https://paydaybesthub.online/# payday loans online no interest
MichaelBlone –
https://paydaybesthub.online/# payday loans online no credit
EduardoVow –
п»їpayday loans: Payday Best Hub – cash now no credit check
MillardPep –
https://generixpharm.shop/# GenerixPharm
Carrollthums –
best acceptance payday loans [url=https://paydaybesthub.com/#]Payday Best Hub[/url] paycheck advance online
melbet_njmi –
melbet bpl betting [url=http://melbet55504.online]melbet bpl betting[/url]
melbet_tyet –
мелбет бо телефони мобилӣ [url=https://www.melbet75116.online]https://www.melbet75116.online[/url]
MichaelBlone –
https://paydaybesthub.shop/# payday loans no interest
melbet_ewet –
как удалить аккаунт мелбет [url=melbet66023.online]как удалить аккаунт мелбет[/url]
aviator_xumi –
aviator game android [url=https://aviator33280.online]aviator game android[/url]
mostbet_kgKt –
мостбет бурд дар lucky jet [url=https://www.mostbet33927.online]мостбет бурд дар lucky jet[/url]
Ralphvieme –
https://paydaybesthub.shop/# cash now no credit check
melbet_nnml –
мелбет ios кыргызстан [url=http://melbet58323.online/]http://melbet58323.online/[/url]
mostbet_tkMn –
mostbet megbízható-e [url=https://mostbet34227.online]https://mostbet34227.online[/url]
mostbet_xmml –
mostbet pl strona [url=https://mostbet74029.online/]https://mostbet74029.online/[/url]
EduardoVow –
payday loans that approve everyone: PaydayBestHub – payday loans no credit check
melbet_trmi –
melbet payment verification [url=www.melbet55504.online]www.melbet55504.online[/url]
MichaelBlone –
https://paydaybesthub.shop/# instant cash advance online no credit check
Ralphvieme –
https://paydaybesthub.com/# payday loans online loan
melbet_nxet –
melbet android боргирӣ [url=www.melbet75116.online]www.melbet75116.online[/url]
Carrollthums –
payday loans that approve everyone [url=https://paydaybesthub.shop/#]most trusted payday loans online[/url] payday loans online apply
MichaelBlone –
https://paydaybesthub.shop/# most trusted payday loans online
mostbet_fjml –
mostbet portal [url=https://www.mostbet74029.online]https://www.mostbet74029.online[/url]
DouglasSes –
http://ucipediatriatoledo.com/# Comprar Viagra online seguro
BrandonMat –
https://ucipediatriatoledo.com/# Comprar Viagra online seguro
RobertBus –
Everything for Minecraft https://topminecraftworldseeds.com in one place: mods, skins, maps, texture packs, and the best seeds for survival, creativity, and adventure. Collections of popular add-ons, installation instructions, updates, and secure downloads for different versions of the game.
DouglasSes –
https://ucipediatriatoledo.shop/# Comprar Viagra
melbet_oiet –
промокод melbet на фрибет [url=http://melbet66023.online]http://melbet66023.online[/url]
BrandonMat –
http://ucipediatriatoledo.com/# Viagra genérico precio
mostbet_flki –
mostbet termeni și condiții [url=mostbet68721.icu]mostbet68721.icu[/url]
Williambob –
farmacia online barata [url=http://pediatraefrainvillalobos.com/#]Farmacia online España[/url] farmacia online
melbet_cuSi –
мелбет быстрый вывод [url=https://melbet31620.online/]мелбет быстрый вывод[/url]
mostbet_czKt –
mostbet как получить фриспины [url=www.mostbet05924.online]www.mostbet05924.online[/url]
melbet_uqml –
игра лаки джет melbet [url=http://melbet58323.online]http://melbet58323.online[/url]
mostbet_erMn –
mostbet free spins feltételek [url=https://mostbet34227.online/]https://mostbet34227.online/[/url]
DouglasSes –
https://ucipediatriatoledo.com/# UCI Pediatría Toledo
BrandonMat –
https://ucipediatriatoledo.com/# Comprar Viagra en España
Vivod iz zapoya na domy_qdpt –
Всем привет из северной столицы. Отец не выходит из штопора. Дети напуганы. Платная клиника — бешеные счета. Короче, единственные, кто приехал быстро — выведение из запоя на дому анонимно. Врач поставил систему. В общем, не потеряйте — вывод из алкогольного запоя нарколог24 [url=https://vyvod-iz-zapoya-na-domu-sankt-peterburg-qbf.ru]https://vyvod-iz-zapoya-na-domu-sankt-peterburg-qbf.ru[/url] Звоните прямо сейчас. Перешлите тем, кто в беде.
BrandonMat –
https://pediatraefrainvillalobos.com/# farmacia barata
DouglasSes –
https://pediatraefrainvillalobos.com/# Farmacias baratas online envío gratis
Williambob –
UCI Pediatría Toledo [url=https://ucipediatriatoledo.shop/#]UCI Pediatría Toledo[/url] Comprar Viagra original online
BrandonMat –
https://ucipediatriatoledo.shop/# UCI Pediatría
mostbet_hkMn –
mostbet magyar regisztráció [url=https://www.mostbet34227.online]https://www.mostbet34227.online[/url]
mostbet_hyKt –
mostbet lucky jet app [url=https://www.mostbet33927.online]mostbet lucky jet app[/url]
melbet_shml –
как вывести с мелбет [url=https://www.melbet58323.online]как вывести с мелбет[/url]
melbet_rwet –
максимальная ставка melbet [url=http://melbet66023.online/]http://melbet66023.online/[/url]
DouglasSes –
http://ucipediatriatoledo.com/# Comprar Viagra en farmacia sin receta
Kapelnica ot pohmelya_pmoi –
Воронеж, всем привет Голова раскалывается Организм просто отказывается работать Короче, единственное что реально спасает — капельница от похмелья цена доступная Вернулся к жизни В общем, вся инфа по ссылке — вывод из запоя в воронеже [url=https://kapelnicza-ot-pokhmelya-voronezh-xqt.ru]https://kapelnicza-ot-pokhmelya-voronezh-xqt.ru[/url] Не мучайтесь рассолами Перешлите тем кто в такой же ситуации
BrandonMat –
http://lacefieldurology.com/# cheapest online ed treatment
mostbet_lgki –
mostbet cod promoțional aviator [url=https://www.mostbet68721.icu]https://www.mostbet68721.icu[/url]
vavada_gooi –
vavada płatności [url=vavada18205.help]vavada18205.help[/url]
Williambob –
low cost ed medication [url=https://lacefieldurology.shop/#]Lacefield[/url] pharmacy websites
BrandonMat –
https://ucipediatriatoledo.com/# UCI Pediatría Toledo
DouglasSes –
http://pediatraefrainvillalobos.com/# Farmacias baratas online envío gratis
mostbet_wgki –
mostbet descărcare [url=https://mostbet68721.icu/]https://mostbet68721.icu/[/url]
mostbet_awKt –
мостбет KGS вывод [url=www.mostbet05924.online]мостбет KGS вывод[/url]
BrandonMat –
https://ucipediatriatoledo.shop/# Comprar Viagra original online
RobertBus –
Everything for Minecraft topminecraftworldseeds com in one place: mods, skins, maps, texture packs, and the best seeds for survival, creativity, and adventure. Collections of popular add-ons, installation instructions, updates, and secure downloads for different versions of the game.
BrandonMat –
http://pediatraefrainvillalobos.com/# Farmacia online envío gratis
Williambob –
buy erectile dysfunction pills [url=https://lacefieldurology.shop/#]Lacefield Urology[/url] trustworthy online pharmacy
Vivod iz zapoya v stacionare_ckPn –
Доброго времени Жесть полная Родственники в панике Домашние методы бесполезны Короче, спасла только госпитализация — быстрый вывод из запоя в стационаре за 3 дня Капельницы и препараты подбирали индивидуально В общем, телефон и цены тут — стационарное выведение из запоя [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-vby.ru]стационарное выведение из запоя[/url] Стационар — это реальный выход Перешлите тем кто в такой же ситуации
mostbet_xjKt –
мостбет mines Кыргызстан [url=https://mostbet05924.online]https://mostbet05924.online[/url]
Vivod iz zapoya na domy_kisi –
Привет с Волги. Кошмар случился. Родные не знают, за что хвататься. Платная клиника — грабёж. Итог, спасла эта служба — вывод из запоя на дому недорого в Самаре. Через пару часов человек пришёл в норму. В общем, вся инфа по ссылке — вывод из запоя самара на дому [url=https://vyvod-iz-zapoya-na-domu-samara-qzf.ru]https://vyvod-iz-zapoya-na-domu-samara-qzf.ru[/url] Каждый час на счету. Киньте ссылку тем, кто рядом с бедой.
BrandonMat –
https://pediatraefrainvillalobos.com/# farmacia online barata
vavada_fvoi –
vavada promocje polska [url=https://vavada18205.help]vavada promocje polska[/url]
Kapelnica ot pohmelya_vsma –
Приветствую После вчерашнего вообще никак Поилки и таблетки не помогают Короче, врачи приехали и поставили систему — капельница от похмелья недорого и качественно Вернулся к жизни В общем, не потеряйте контакты — прокапаться от алкоголя на дому [url=https://kapelnicza-ot-pokhmelya-voronezh-ges.ru]прокапаться от алкоголя на дому[/url] Капельница — это быстро и эффективно Перешлите тем кто в такой же ситуации
melbet_ygSi –
melbet скачать бк кыргызстан [url=https://melbet31620.online/]https://melbet31620.online/[/url]
BrandonMat –
https://pediatraefrainvillalobos.com/# Farmacias baratas online envío gratis
Vivod iz zapoya v stacionare_zikr –
Доброго дня, земляки Муж просто потерял себя Соседи стучат в стену Таблетки не помогают Короче, единственное что вытащило из запоя — вывод из запоя в стационаре круглосуточно Выписали через 5 дней без ломки В общем, жмите чтобы сохранить — цена вывода из запоя в стационаре [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-jkp.ru]https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-jkp.ru[/url] Звоните прямо сейчас Перешлите тем кто в такой же ситуации
mostbet_ulKt –
мостбет блэкҷек [url=https://www.mostbet33927.online]мостбет блэкҷек[/url]
Vivod iz zapoya na domy_xbpl –
Здорова, народ. Брат не выходит из штопора. Соседи уже стучат в стену. Скорая не приедет на такой вызов. Короче, единственные, кто быстро приехал — вывод из запоя с выездом круглосуточно. Сняли интоксикацию. В общем, жмите, чтобы сохранить — вывести из запоя на дому [url=https://vyvod-iz-zapoya-na-domu-samara-nxc.ru]вывести из запоя на дому[/url] Каждый час ухудшает состояние. Перешлите тем, кто рядом с бедой.
Kapelnica ot pohmelya_jqsr –
Привет из Черноземья Жесть после вчерашнего Организм просто отказывается работать Короче, единственное что реально спасает — капельница от похмелья на дому срочно Приехали через 30 минут В общем, телефон и цены тут — сделать капельницу на дому цена [url=https://kapelnicza-ot-pokhmelya-voronezh-mnb.ru]https://kapelnicza-ot-pokhmelya-voronezh-mnb.ru[/url] Капельница — это быстро и эффективно Перешлите тем кто в такой же ситуации
mostbet_gwea –
mostbet oglindă funcțională [url=www.mostbet94451.icu]www.mostbet94451.icu[/url]
vavada_eeoi –
vavada zakłady przedmeczowe [url=https://vavada18205.help]https://vavada18205.help[/url]
Williambob –
Viagra genérico precio [url=https://ucipediatriatoledo.shop/#]Comprar Viagra online seguro[/url] Viagra genérica sin receta
BrandonMat –
https://ucipediatriatoledo.shop/# Viagra precio sin receta
melbet_slEt –
мелбет скачать бесплатно [url=https://melbet25717.online/]https://melbet25717.online/[/url]
mostbet_jzet –
mostbet erkən çıxış necə [url=www.mostbet24939.online]mostbet erkən çıxış necə[/url]
mostbet_iaea –
mostbet депозит [url=https://mostbet86043.help]https://mostbet86043.help[/url]
aviator_wokn –
aviator pix brasil [url=https://aviator92671.help/]aviator pix brasil[/url]
melbet_fzSi –
мелбет бонус без депозита [url=https://melbet31620.online]https://melbet31620.online[/url]
BrandonMat –
https://ucipediatriatoledo.com/# Comprar Viagra en España
Vivod iz zapoya v stacionare_zqMa –
Всем привет из Питера Кошмар в семье Родственники в полном отчаянии В диспансер тащить — последнее дело Короче, спасла только госпитализация — наркология вывод из запоя в стационаре с психологом Врачи и медсёстры 24/7 В общем, вся инфа по ссылке — лечение от запоя в стационаре [url=https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-gtb.ru]https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-gtb.ru[/url] Стационар — это единственный выход Это может спасти жизнь
BrandonMat –
https://ucipediatriatoledo.com/# Comprar Viagra en España
Vivod iz zapoya na domy_djKt –
Доброго времени, земляки. Мой брат уже четвёртые сутки в запое. Соседи уже стучат в стену. В наркологию тащить — стыд и страх. Короче, единственные, кто быстро приехал — вывод из запоя на дому недорого. Приехали через 35 минут. В общем, цены и телефон тут — нарколог на дом вывод из запоя на дому [url=https://vyvod-iz-zapoya-na-domu-samara-rtw.ru]нарколог на дом вывод из запоя на дому[/url] Звоните прямо сейчас. Вдруг это спасёт чью-то жизнь.
Williambob –
Viagra genérico precio [url=https://ucipediatriatoledo.shop/#]Viagra genérica sin receta[/url] Comprar Viagra en España
BrandonMat –
http://pediatraefrainvillalobos.com/# Farmacias baratas online envío gratis
mostbet_kyea –
mostbet portal [url=http://mostbet94451.icu/]http://mostbet94451.icu/[/url]
vavada_mhoi –
vavada warunki bonusu [url=http://vavada18205.help/]vavada warunki bonusu[/url]
pinup_gfKl –
pinup telegram bormi [url=http://pinup01611.help]http://pinup01611.help[/url]
melbet_meEt –
мелбет результаты матчей [url=http://melbet25717.online/]http://melbet25717.online/[/url]
BrandonMat –
https://ucipediatriatoledo.shop/# UCI Pediatría Toledo
mostbet_qaet –
mostbet oyun qaydaları crash [url=https://mostbet24939.online]https://mostbet24939.online[/url]
mostbet_dgea –
мостбет free bet [url=https://mostbet86043.help]мостбет free bet[/url]
mostbet_ilea –
cum joc lucky jet pe mostbet [url=http://mostbet94451.icu/]http://mostbet94451.icu/[/url]
aviator_gokn –
aviator saque pix [url=http://aviator92671.help/]http://aviator92671.help/[/url]
BrandonMat –
https://ucipediatriatoledo.com/# Comprar Viagra online seguro
Vivod iz zapoya v stacionare_gfsa –
Всем привет из северной столицы Отец не встаёт с кровати Дети боятся даже подходить Скорая отказывается выезжать Короче, единственное что сработало — вывод из запоя санкт-петербург стационар с палатой Врачи и медсёстры круглосуточно В общем, телефон и цены тут — вывод из запоя стационарно [url=https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-zqe.ru]вывод из запоя стационарно[/url] Звоните прямо сейчас Это может спасти жизнь близкого
RobertBus –
Everything for Minecraft topminecraftworldseeds com in one place: mods, skins, maps, texture packs, and the best seeds for survival, creativity, and adventure. Collections of popular add-ons, installation instructions, updates, and secure downloads for different versions of the game.
Vivod iz zapoya v stacionare_jrpr –
Слушайте кто сталкивался Муж просто потерял себя Родственники не знают что делать Скорая не приедет на такой вызов Короче, врачи вытащили с того света — лечение запоя в стационаре до полной стабилизации Положили в комфортную палату В общем, не потеряйте контакты — вывод из запоя в клинике спб [url=https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-axm.ru]https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-axm.ru[/url] Не надейтесь что само пройдёт Это может спасти чью-то семью
Williambob –
Comprar Viagra online seguro [url=https://ucipediatriatoledo.com/#]Comprar Viagra en farmacia sin receta[/url] Viagra precio sin receta
BrandonMat –
https://lacefieldurology.com/# erectile dysfunction medicine online
mostbet_saet –
mostbet oyun demo [url=http://mostbet24939.online]http://mostbet24939.online[/url]
mostbet_ckea –
как активировать промокод mostbet [url=https://mostbet86043.help/]как активировать промокод mostbet[/url]
aviator_kdkn –
aviator pagamento de ganhos [url=aviator92671.help]aviator pagamento de ganhos[/url]
BrandonMat –
https://ucipediatriatoledo.com/# Viagra genérica sin receta
vavada_yioi –
vavada aviator jak wypłacić [url=https://vavada18205.help]vavada aviator jak wypłacić[/url]
pinup_shKl –
pin up Oʻzbekistonda depozit [url=http://pinup01611.help]http://pinup01611.help[/url]
Jerryesoxy –
https://vgrfrancepharm.online/# Viagra femme sans ordonnance 24h
mostbet_mpKr –
мостбет создать аккаунт [url=http://mostbet66053.online]http://mostbet66053.online[/url]
melbet_luEt –
мелбет плинко [url=https://melbet25717.online/]https://melbet25717.online/[/url]
melbet_nuol –
melbet экспресс киргизия [url=https://melbet56606.online]https://melbet56606.online[/url]
Vivod iz zapoya na domy_kksi –
Здорова, народ. Кошмар случился. Родные не знают, за что хвататься. Скорая не приедет на такой вызов. Итог, спасла эта служба — вывод из запоя дешево и без лишних трат. Через пару часов человек пришёл в норму. В общем, цены и телефон тут — вывод из запоя на дому [url=https://vyvod-iz-zapoya-na-domu-samara-qzf.ru]вывод из запоя на дому[/url] Каждый час на счету. Вдруг пригодится.
Rickeylem –
https://vgrfrancepharm.online/# Viagra sans ordonnance livraison 48h
Jerryesoxy –
https://vgrfrancepharm.online/# Meilleur Viagra sans ordonnance 24h
RobertBus –
Everything for Minecraft https://topminecraftworldseeds.com in one place: mods, skins, maps, texture packs, and the best seeds for survival, creativity, and adventure. Collections of popular add-ons, installation instructions, updates, and secure downloads for different versions of the game.
vavada_ynoi –
vavada zakłady mobilne [url=http://vavada18205.help]http://vavada18205.help[/url]
pinup_ryKl –
pin-up to‘lov usullari Oʻzbekiston [url=http://pinup01611.help]http://pinup01611.help[/url]
aviator_vjOa –
aviator mw apk [url=http://aviator19661.online/]http://aviator19661.online/[/url]
mostbet_egKn –
создать аккаунт мостбет [url=https://mostbet03253.online/]создать аккаунт мостбет[/url]
Vivod iz zapoya v stacionare_cpOl –
Доброго вечера, земляки Отец не выходит из штопора Соседи стучат Таблетки не помогают Короче, врачи вытащили с того света — цена на вывод из запоя в стационаре доступная Врачи наблюдали 24/7 В общем, вся инфа по ссылке — стационар капельница от алкоголя [url=https://vyvod-iz-zapoya-v-staczionare-nizhnij-novgorod-elm.ru]стационар капельница от алкоголя[/url] Не ждите пока станет хуже Перешлите тем кто в такой же ситуации
Jerryesoxy –
https://sildfrancedelivery.icu/# Viagra pas cher paris
mostbet_jzEl –
mostbet сом пополнение [url=https://mostbet32915.help/]https://mostbet32915.help/[/url]
Jerryesoxy –
https://mexicanfastdelivery.top/# online pharmacies in mexico
mostbet_iqSi –
mostbet Oʻzbekiston click [url=https://mostbet81183.help/]https://mostbet81183.help/[/url]
mostbet_xoKr –
mostbet Баткен [url=http://mostbet66053.online]mostbet Баткен[/url]
Rickeylem –
https://mexicanusarx.online/# mexican mail order pharmacy
Jerryesoxy –
https://sildenafilsansordonnance.online/# Viagra Pfizer sans ordonnance
RobertBus –
Everything for Minecraft https://topminecraftworldseeds.com/ in one place: mods, skins, maps, texture packs, and the best seeds for survival, creativity, and adventure. Collections of popular add-ons, installation instructions, updates, and secure downloads for different versions of the game.
melbet_rlpl –
melbet webmoney [url=https://melbet33145.help]https://melbet33145.help[/url]
melbet_kgol –
melbet бонус за регистрацию [url=www.melbet56606.online]melbet бонус за регистрацию[/url]
Jerryesoxy –
https://sildenafilsansordonnance.online/# Viagra sans ordonnance pharmacie France
aviator_fzOa –
aviator ios download [url=https://www.aviator19661.online]https://www.aviator19661.online[/url]
mostbet_rpKn –
мостбет блэкджек [url=www.mostbet03253.online]мостбет блэкджек[/url]
mostbet_keKr –
мостбет поддержка telegram [url=http://mostbet66053.online/]мостбет поддержка telegram[/url]
Jerryesoxy –
https://mexicomedsrx.online/# mexican pharmacies
melbet_paol –
мелбет cashback киргизия [url=www.melbet56606.online]мелбет cashback киргизия[/url]
Vivod iz zapoya v stacionare_ksMi –
Слушайте кто сталкивался Кошмар полный Соседи уже вызвали скорую Платная клиника — выкачивает деньги Короче, спасла только госпитализация — лечение запоя в стационаре комплексно Капельницы и препараты по назначению В общем, не потеряйте контакты — выведение из запоя стационар санкт петербург [url=https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-wjf.ru]https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-wjf.ru[/url] Звоните прямо сейчас Перешлите тем кто в такой же ситуации
aviator_fzOa –
aviator install on android [url=http://aviator19661.online/]http://aviator19661.online/[/url]
mostbet_qeEl –
mostbet бонус за регистрацию [url=https://mostbet32915.help/]mostbet бонус за регистрацию[/url]
Rickeylem –
https://sildfrancedelivery.icu/# Viagra en france livraison rapide
mostbet_qmSi –
mostbet proxy [url=https://mostbet81183.help/]https://mostbet81183.help/[/url]
Jerryesoxy –
https://mexicanfastdelivery.top/# affordable pharmacy
mostbet_wjKn –
мостбет как получить фрибет [url=http://mostbet03253.online]http://mostbet03253.online[/url]
pinup_npEa –
pin-up app Chile ios [url=http://pinup15843.help]http://pinup15843.help[/url]
Vivod iz zapoya v stacionare_htSl –
Всем привет из Питера Сосед совсем спился Мать места себе не находит Скорая не приезжает на такие вызовы Короче, врачи стационара реально помогли — выведение из запоя в стационаре под наблюдением Капельницы и уколы по назначению В общем, вся инфа по ссылке — вывод из запоя в клинике [url=https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-nhy.ru]https://vyvod-iz-zapoya-v-staczionare-sankt-peterburg-nhy.ru[/url] Звоните прямо сейчас Перешлите тем кто в такой же беде
Jerryesoxy –
https://sildenafilsansordonnance.online/# Viagra homme prix en pharmacie
melbet_zfpl –
jocuri sloturi melbet [url=http://melbet33145.help/]http://melbet33145.help/[/url]
mostbet_vmEl –
мостбет apk [url=mostbet32915.help]mostbet32915.help[/url]
vavada_itoa –
vavada strona internetowa [url=www.vavada73941.help]vavada strona internetowa[/url]
RobertBus –
Everything for Minecraft topminecraftworldseeds com in one place: mods, skins, maps, texture packs, and the best seeds for survival, creativity, and adventure. Collections of popular add-ons, installation instructions, updates, and secure downloads for different versions of the game.
Allenmen –
https://clinicalpathiver.shop/# ClinicalPathIver
AltonShoon –
farmacie online affidabili: FarmaciaCaman – safe online pharmacies
mostbet_zjSi –
mostbet qo‘llab-quvvatlash o‘zbekcha [url=www.mostbet81183.help]www.mostbet81183.help[/url]
Allenmen –
https://clinicalpathiver.shop/# ClinicalPathIver
mostbet_tiea –
mostbet_kg [url=mostbet57408.online]mostbet57408.online[/url]
mostbet_ykpn –
mostbet mines donur [url=www.mostbet27461.online]www.mostbet27461.online[/url]
melbet_akpl –
melbet Moldova [url=https://www.melbet33145.help]melbet Moldova[/url]
Allenmen –
http://farmaciacaman.com/# farmacia online piГ№ conveniente
pinup_kmEa –
pin up web [url=https://pinup15843.help]https://pinup15843.help[/url]
AltonShoon –
ClinicalPathIver: ClinicalPathIver – ivermectin cost canada
Allenmen –
https://cyclecareclomid.shop/# CycleCareClomid
pinup_hxEa –
descargar pin-up Chile [url=http://pinup15843.help/]http://pinup15843.help/[/url]
Allenmen –
http://cyclecareclomid.com/# where to buy cheap clomid without insurance
vavada_oyoa –
vavada rejestracja bonus darmowe spiny [url=https://vavada73941.help]https://vavada73941.help[/url]
Allenmen –
http://farmaciacaman.com/# farmacie online sicure
AltonShoon –
stromectol usa: ClinicalPathIver – stromectol 3 mg
RobertBus –
Everything for Minecraft topminecraftworldseeds com in one place: mods, skins, maps, texture packs, and the best seeds for survival, creativity, and adventure. Collections of popular add-ons, installation instructions, updates, and secure downloads for different versions of the game.
vavada_iwoa –
vavada strategie plinko [url=http://vavada73941.help/]http://vavada73941.help/[/url]
mostbet_hhea –
mostbet plinko стратегия [url=https://www.mostbet57408.online]mostbet plinko стратегия[/url]
mostbet_zopn –
mostbet app login problem [url=https://mostbet27461.online/]https://mostbet27461.online/[/url]
Allenmen –
https://clinicalpathiver.com/# ivermectin lotion cost
AndrewItern –
buy generic clomid without rx: can you get generic clomid without dr prescription – how to buy cheap clomid no prescription
LutherASYMN –
stromectol medicine [url=https://clinicalpathiver.shop/#]stromectol generic[/url] stromectol 12mg
Allenmen –
https://farmaciacaman.com/# farmaci senza ricetta elenco
AltonShoon –
CycleCareClomid: cost of generic clomid without insurance – order generic clomid without rx
AndrewItern –
CycleCareClomid: CycleCareClomid – CycleCareClomid
Narkologicheskii stacionar_tjSn –
Слушайте кто сталкивался Близкий человек уже неделю в запое Родственники не знают что делать В диспансер тащить — страшно и стыдно Короче, врачи вытащили с того света — платный наркологический стационар с палатами Положили в комфортную палату В общем, телефон и цены тут — наркологическая клиника стационар [url=https://narkologicheskij-staczionar-moskva-lba.ru]наркологическая клиника стационар[/url] Не надейтесь что само пройдёт Перешлите тем кто в отчаянии
mostbet_kbea –
mostbet киберспорт ставки [url=mostbet57408.online]mostbet57408.online[/url]
mostbet_qnpn –
mostbet Azərbaycan üçün android [url=https://mostbet27461.online]https://mostbet27461.online[/url]
Narkologicheskii stacionar_pjor –
Люди помогите советом Близкий человек просто умирает на глазах Дети боятся даже подходить Платная наркология — бешеные счета Короче, спасла только госпитализация — наркологическая клиника стационар с круглосуточным наблюдением Положили в отдельную палату В общем, жмите чтобы сохранить — наркологический стационар цена [url=https://narkologicheskij-staczionar-moskva-pfk.ru]наркологический стационар цена[/url] Стационар — единственное решение Перешлите тем кто в такой же беде
LutherASYMN –
Farmacia online miglior prezzo [url=https://farmaciacaman.online/#]FarmaciaCaman[/url] trustworthy online pharmacy
Allenmen –
https://farmaciacaman.online/# farmacia online
chicken-road_mxka –
chicken road jugar desde españa [url=https://chicken-road71226.icu/]https://chicken-road71226.icu/[/url]
chicken-road_fzki –
chicken road alta [url=www.chicken-road86685.icu]www.chicken-road86685.icu[/url]
chicken-road_komn –
chicken road prelievo con mastercard [url=http://chicken-road71021.icu]http://chicken-road71021.icu[/url]
Narkologicheskii stacionar_khpl –
Люди подскажите Близкий человек уже 10 дней в запое Дети боятся заходить в комнату Платная клиника просит бешеные деньги Короче, врачи стационара реально вытащили — наркологические услуги в стационаре полный комплекс Провели полную детоксикацию В общем, жмите чтобы сохранить — сколько стоит прокапаться от алкоголя в стационаре [url=https://narkologicheskij-staczionar-moskva-jmw.ru]https://narkologicheskij-staczionar-moskva-jmw.ru[/url] Звоните прямо сейчас Это может спасти жизнь
LutherASYMN –
how to get generic clomid pill [url=https://cyclecareclomid.shop/#]cost generic clomid without a prescription[/url] where buy cheap clomid without prescription
Allenmen –
http://clinicalpathiver.com/# stromectol australia
Narkologicheskii stacionar_oepl –
Слушайте кто сталкивался Соседний мужик совсем спился Дети боятся даже подходить В диспансер тащить — стыд и страх Короче, спасла только госпитализация — наркологические услуги в стационаре комплексно Положили в отдельную палату В общем, жмите чтобы сохранить — наркологическая клиника стационар [url=https://narkologicheskij-staczionar-moskva-cde.ru]наркологическая клиника стационар[/url] Стационар — единственное решение Перешлите тем кто в такой же беде
Narkologicheskii stacionar_bgPr –
Здорова, народ Жесть полная Дети боятся заходить в дом Платная клиника — бешеные счета Короче, спасла только госпитализация — платный наркологический стационар с палатами Врачи и медсёстры 24/7 В общем, жмите чтобы сохранить — лечение алкоголизма стационар цены [url=https://narkologicheskij-staczionar-moskva-fal.ru]https://narkologicheskij-staczionar-moskva-fal.ru[/url] Стационар — единственное решение Перешлите тем кто в такой же беде
AndrewItern –
top farmacia online: Farmacie on line spedizione gratuita – no prescription pharmacy paypal
AltonShoon –
ClinicalPathIver: stromectol liquid – ClinicalPathIver
plinko_brPn –
plinko apostar desde argentina [url=http://plinko90488.icu/]http://plinko90488.icu/[/url]
chicken-road_zasa –
chicken road espana sitio oficial [url=http://chicken-road35537.icu]http://chicken-road35537.icu[/url]
Allenmen –
https://cyclecareclomid.com/# CycleCareClomid
LutherASYMN –
stromectol coronavirus [url=http://clinicalpathiver.com/#]ClinicalPathIver[/url] ClinicalPathIver
AndrewItern –
farmaci senza ricetta elenco: comprare farmaci online all’estero – overseas online pharmacy
Allenmen –
https://farmaciacaman.online/# farmacia online piГ№ conveniente
LutherASYMN –
ClinicalPathIver [url=https://clinicalpathiver.com/#]ivermectin 80 mg[/url] ClinicalPathIver
chicken-road_vski –
chicken road app android españa [url=www.chicken-road86685.icu]www.chicken-road86685.icu[/url]
Allenmen –
https://farmaciacaman.online/# Farmacia online miglior prezzo
chicken-road_dfmn –
chicken road sito alternativo [url=chicken-road71021.icu]chicken-road71021.icu[/url]
AltonShoon –
where to buy cheap clomid prices: where can i buy generic clomid without a prescription – can i buy generic clomid without prescription
LutherASYMN –
where buy generic clomid online [url=http://cyclecareclomid.com/#]CycleCareClomid[/url] CycleCareClomid
chicken-road_qjki –
mines chicken road [url=https://chicken-road86685.icu/]mines chicken road[/url]
Allenmen –
https://cyclecareclomid.shop/# cost of clomid pill
plinko_rlPn –
plinko argentina ios [url=https://plinko90488.icu/]https://plinko90488.icu/[/url]
AndrewItern –
ivermectin generic name: buy ivermectin nz – ClinicalPathIver
chicken-road_qdsa –
chicken road tragaperras [url=https://www.chicken-road35537.icu]https://www.chicken-road35537.icu[/url]
chicken-road_qimn –
chicken road prelievo con revolut [url=chicken-road71021.icu]chicken-road71021.icu[/url]
LutherASYMN –
ClinicalPathIver [url=https://clinicalpathiver.com/#]ivermectin gel[/url] stromectol tablets uk
Allenmen –
https://farmaciacaman.online/# farmacie online sicure
Narkologicheskii stacionar_ciMa –
Москва, всем привет Близкий человек уже неделю в запое Соседи стучат в стену Платная клиника — бешеные деньги Короче, только стационар реально помог — госпитализация в наркологический стационар 24/7 Положили в комфортную палату В общем, вся инфа по ссылке — наркологическая клиника стационар [url=https://narkologicheskij-staczionar-moskva-vex.ru]наркологическая клиника стационар[/url] Не надейтесь что само пройдёт Перешлите тем кто в отчаянии
AndrewItern –
Farmacie online sicure: Farmacia online piГ№ conveniente – pharmacy order online
plinko_xtPn –
plinko promo recarga [url=www.plinko90488.icu]www.plinko90488.icu[/url]
Allenmen –
http://farmaciacaman.com/# Farmacie on line spedizione gratuita
AltonShoon –
ClinicalPathIver: ClinicalPathIver – ClinicalPathIver
LutherASYMN –
cheap clomid tablets [url=https://cyclecareclomid.com/#]can i purchase generic clomid pills[/url] where buy generic clomid pill
chicken-road_kisa –
chicken road lucky jet [url=https://chicken-road35537.icu/]chicken road lucky jet[/url]
mostbet_aoSt –
mostbet карта вывод [url=http://mostbet49108.online/]http://mostbet49108.online/[/url]
Justinnek –
buy drugs online: purple pharmacy – farmacias mexicanas
Daviddaymn –
https://doctortopfrance.icu/# Viagra pas cher inde
Justinnek –
SildГ©nafil 100 mg prix en pharmacie en France: Viagra homme sans prescription – Viagra homme prix en pharmacie sans ordonnance
mostbet_dlSn –
mostbet ingyenes nyerőgépek [url=mostbet50579.icu]mostbet50579.icu[/url]
Daviddaymn –
https://mexicotoppharmacy.icu/# mexican pharmacy ship to usa
chicken-road_qgOa –
chicken road app ios [url=http://chicken-road29283.icu]http://chicken-road29283.icu[/url]
mostbet_hoKt –
мостбет слоты на деньги [url=https://mostbet68667.icu]https://mostbet68667.icu[/url]
Michaelbum –
mexico pharmacy list [url=https://mexicotoppharmacy.icu/#]pharmacy mexico[/url] purple pharmacy mexico
chicken-road_uqka –
descargar chicken road android [url=http://chicken-road71226.icu]http://chicken-road71226.icu[/url]
Justinnek –
pharma mexicana: mexico pharmacy price list – mexico pharmacy list
Daviddaymn –
https://vgrsansordonnance.online# Viagra homme sans ordonnance belgique
mostbet_pwSt –
мостбет скачать на ios Киргизия [url=https://www.mostbet49108.online]https://www.mostbet49108.online[/url]
Narkologicheskii stacionar_niKt –
Здорова, народ Брат снова сорвался в пьянку Соседи стучат в стену Платная клиника — бешеные деньги Короче, только стационар реально помог — платный наркологический стационар с палатами Капельницы и препараты подбирали индивидуально В общем, жмите чтобы сохранить — наркологические услуги в стационаре [url=https://narkologicheskij-staczionar-moskva-gsh.ru]наркологические услуги в стационаре[/url] Стационар — это реальный шанс Перешлите тем кто в отчаянии
mostbet_miSl –
mostbet kasyno na żywo [url=www.mostbet40086.online]www.mostbet40086.online[/url]
melbet_hckn –
мелбет crash играть [url=http://melbet01191.online]http://melbet01191.online[/url]
Daviddaymn –
https://mexicandoctortous.online/# pharmacy in mexico online
chicken-road_uoka –
chicken road instalar app [url=https://chicken-road71226.icu]https://chicken-road71226.icu[/url]
Justinnek –
mexico drug store online: mexican online pharmacy – mexi pharmacy
mostbet_mhSt –
mostbet коэффициенты футбол Кыргызстан [url=http://mostbet49108.online/]mostbet коэффициенты футбол Кыргызстан[/url]
Michaelbum –
Viagra homme prix en pharmacie sans ordonnance [url=https://vgrsansordonnance.online#]Viagra pas cher livraison rapide france[/url] Prix du Viagra en pharmacie en France
Daviddaymn –
https://mexicandoctortous.online/# mexican pharmacy las vegas
chicken-road_skOa –
chicken road vpn acceso [url=https://chicken-road29283.icu]https://chicken-road29283.icu[/url]
Kapelnica ot pohmelya_nzol –
Здорова, народ Тошнит, трясёт, сил нет Организм просто отказывается работать Короче, нашел реально работающий способ — капельница от похмелья на дому срочно Через час состояние нормализовалось В общем, не потеряйте контакты — снятие похмелья капельницей [url=https://kapelnicza-ot-pokhmelya-voronezh-itw.ru]https://kapelnicza-ot-pokhmelya-voronezh-itw.ru[/url] Не мучайтесь рассолами Перешлите тем кто в такой же ситуации
Justinnek –
mexican pharmacies that ship: mexico farmacia – purple pharmacy mexico
mostbet_qiKt –
mostbet верификация сколько дней [url=http://mostbet68667.icu/]http://mostbet68667.icu/[/url]
Daviddaymn –
https://doctortopfrance.icu/# Viagra femme ou trouver
chicken-road_nwOa –
chicken road descarga android [url=chicken-road29283.icu]chicken-road29283.icu[/url]
Daviddaymn –
https://mexicotoppharmacy.icu/# farmacia mexicana en linea
Kapelnica ot pohmelya_wuei –
Салют, Самара После вчерашнего вообще никак Рассол уже не лезет Короче, нашел реально работающий способ — капельница при похмелье с препаратами Поставили капельницу с солевым раствором В общем, жмите чтобы сохранить — капельница после запоя цена [url=https://kapelnicza-ot-pokhmelya-samara-dxq.ru]капельница после запоя цена[/url] Звоните прямо сейчас Перешлите тем кто в такой же ситуации
mostbet_nkor –
mostbet коэффициенты [url=www.mostbet14673.help]mostbet коэффициенты[/url]
melbet_ofkn –
melbet карта вывод [url=https://melbet01191.online/]https://melbet01191.online/[/url]
mostbet_mdSl –
mines mostbet [url=https://www.mostbet40086.online]https://www.mostbet40086.online[/url]
mostbet_dqOr –
mostbet aksiyа kod [url=https://mostbet50191.help/]https://mostbet50191.help/[/url]
Michaelbum –
pharmacy online [url=https://mexicandoctorate.top/#]pharmacy in mexico[/url] pharmacies in mexico that ship to the us
mostbet_ikKt –
мостбет вход ошибка [url=http://mostbet68667.icu/]http://mostbet68667.icu/[/url]
Justinnek –
Viagra gГ©nГ©rique sans ordonnance en pharmacie: Viagra homme sans ordonnance belgique – Viagra sans ordonnance pharmacie France
mostbet_vuSn –
mostbet fiók hitelesítés [url=http://mostbet50579.icu]http://mostbet50579.icu[/url]
Daviddaymn –
https://doctortopfrance.icu/# Viagra homme prix en pharmacie sans ordonnance
melbet_sfsa –
melbet kz вывод на mastercard [url=https://melbet62490.help]https://melbet62490.help[/url]
Justinnek –
Quand une femme prend du Viagra homme: Viagra prix pharmacie paris – Viagra vente libre pays
melbet_hjkn –
melbet отзывы бишкек [url=http://melbet01191.online/]melbet отзывы бишкек[/url]
mostbet_jaSl –
mostbet automaty online [url=http://mostbet40086.online/]http://mostbet40086.online/[/url]
Daviddaymn –
https://vgrsansordonnance.top/# Viagra homme prix en pharmacie
mostbet_pior –
mostbet скачать приложение на android [url=www.mostbet14673.help]www.mostbet14673.help[/url]
Daviddaymn –
https://vgrsansordonnance.top/# Acheter viagra en ligne livraison 24h
Justinnek –
Prix du Viagra 100mg en France: SildГ©nafil 100 mg sans ordonnance – Viagra prix pharmacie paris
Michaelbum –
Viagra 100mg prix [url=https://vgrsansordonnance.top/#]Sildenafil teva 100 mg sans ordonnance[/url] Sildenafil teva 100 mg sans ordonnance
mostbet_tnSn –
mostbet promóciós feltételek [url=www.mostbet50579.icu]www.mostbet50579.icu[/url]
Daviddaymn –
https://mexicotoppharmacy.icu/# п»їmexican pharmacy
plinko_ibOt –
установить плинко app [url=https://plinko29475.help]установить плинко app[/url]
Justinnek –
mexipharmacy reviews: online drugs order – buying prescription drugs in mexico
mostbet_ptor –
mostbet казино слоты Кыргызстан [url=https://www.mostbet14673.help]https://www.mostbet14673.help[/url]
Daviddaymn –
https://mexicotoppharmacy.icu/# online mexico pharmacy
melbet_nnsa –
мелбет ставки на хоккей [url=http://melbet62490.help]http://melbet62490.help[/url]
Justinnek –
hydrocodone mexico pharmacy: pharmacy online – mexico farmacia
Michaelbum –
best online mexican pharmacy [url=https://mexicandoctorate.top/#]pharmacy mexico online[/url] mexicanrxpharm
Kapelnica ot pohmelya_rvpl –
Доброго дня, земляки После вчерашнего вообще никак Поилки и таблетки не помогают Короче, нашел реально работающий способ — капельница от похмелья на дому срочно Поставили капельницу с солевым раствором В общем, не потеряйте контакты — прокапаться на дому от алкоголя цена [url=https://kapelnicza-ot-pokhmelya-ekaterinburg-sdj.ru]прокапаться на дому от алкоголя цена[/url] Капельница — это быстро и эффективно Перешлите тем кто в такой же ситуации
Kapelnica ot zapoya_swol –
Салют, Екатеринбург Мой отец уже пятые сутки в запое Родственники не знают что делать В клинику везти страшно Короче, спасла только эта капельница — капельница на дому от запоя с препаратами Приехали через 30 минут В общем, не потеряйте контакты — сколько стоит прокапаться от алкоголя на дому [url=https://kapelnicza-ot-zapoya-ekaterinburg-nmx.ru]https://kapelnicza-ot-zapoya-ekaterinburg-nmx.ru[/url] Звоните прямо сейчас Перешлите тем кто в такой же беде
Daviddaymn –
https://doctortopfrance.icu/# Viagra 100 mg sans ordonnance
melbet_iasa –
melbet kz aviator как играть [url=https://www.melbet62490.help]melbet kz aviator как играть[/url]
Justinnek –
Viagra sans ordonnance 24h Amazon: SildГ©nafil 100 mg prix en pharmacie en France – Viagra pas cher inde
Daviddaymn –
https://mexicandoctortous.online/# meds from mexico
Daviddaymn –
https://vgrsansordonnance.online# Viagra femme sans ordonnance 24h
mostbet_cpor –
мостбет войти [url=https://mostbet59898.online]мостбет войти[/url]
Justinnek –
Viagra homme prix en pharmacie: Viagra homme sans ordonnance belgique – Meilleur Viagra sans ordonnance 24h
plinko_gyOt –
плинко пополнение usdt [url=https://plinko29475.help]плинко пополнение usdt[/url]
Kapelnica ot zapoya_lgmi –
Доброго вечера, земляки Сосед совсем спился Соседи стучат В клинику тащить страшно Короче, спасла только эта капельница — капельница от запоя на дому круглосуточно Поставили капельницу с детокс-раствором В общем, вся инфа по ссылке — капельница при похмелье [url=https://kapelnicza-ot-zapoya-ekaterinburg-sdj.ru]https://kapelnicza-ot-zapoya-ekaterinburg-sdj.ru[/url] Не ждите пока станет хуже Перешлите тем кто в такой же беде
Daviddaymn –
https://doctortopfrance.icu/# Viagra vente libre allemagne
mostbet_lzMr –
mostbet aktiv promo kod [url=https://mostbet20142.online]mostbet aktiv promo kod[/url]
Daviddaymn –
https://vgrsansordonnance.top/# Viagra prix pharmacie paris
plinko_rsOt –
плинко зеркало рабочее Казахстан [url=https://plinko29475.help/]плинко зеркало рабочее Казахстан[/url]
Justinnek –
progreso mexico pharmacy online: mexican online mail order pharmacy – order medicine from mexico
mostbet_kfor –
mostbet букмекерская контора официальный сайт [url=www.mostbet59898.online]www.mostbet59898.online[/url]
Michaelbum –
Viagra pas cher livraison rapide france [url=https://doctortopfrance.icu/#]Viagra sans ordonnance pharmacie France[/url] Viagra homme prix en pharmacie sans ordonnance
Daviddaymn –
https://mexicandoctortous.online/# mexican pharmacy near me
mostbet_zdSi –
mostbet вывод на uzcard [url=https://mostbet38274.help]https://mostbet38274.help[/url]
mostbet_xzel –
mostbet debetní karta vklad [url=http://mostbet90833.online]mostbet debetní karta vklad[/url]
mostbet_alor –
мостбет приветственный бонус [url=mostbet59898.online]mostbet59898.online[/url]
Daviddaymn –
https://vgrsansordonnance.online# Viagra vente libre allemagne
Justinnek –
medication from mexico: prescriptions from mexico – mexico prescriptions
Narkolog na dom_sjSn –
Здорова, народ Близкий человек уже несколько дней в запое Соседи стучат в стену Нужна срочная помощь на дому Короче, нарколог приехал за час — вызвать нарколога на дом круглосуточно Приехал через 35 минут В общем, телефон и цены тут — вызвать врача нарколога на дом круглосуточно [url=https://narkolog-na-dom-moskva-xyz.ru]https://narkolog-na-dom-moskva-xyz.ru[/url] Не ждите пока станет хуже Перешлите тем кто в такой же ситуации
Daviddaymn –
https://mexicotoppharmacy.icu/# mexican pharmacy near me
Justinnek –
Quand une femme prend du Viagra homme: Viagra pas cher livraison rapide france – Viagra femme ou trouver
Narkolog na dom_iooa –
Приветствую Брат снова сорвался Жена в панике Таблетки не помогают Короче, единственный кто реально помог — наркологическая помощь на дому быстро Осмотрел и поставил капельницу В общем, не потеряйте контакты — нарколог на дом анонимно москва [url=https://narkolog-na-dom-moskva-abc.ru]https://narkolog-na-dom-moskva-abc.ru[/url] Нарколог на дом — это быстро и эффективно Перешлите тем кто в такой же ситуации
Daviddaymn –
https://mexicotoppharmacy.icu/# affordable pharmacy
Justinnek –
mexican meds: mexican drugstore – mexican drug stores
Daviddaymn –
https://mexicandoctortous.online/# pharmacy in mexico online
mostbet_piOr –
mostbet Namangan payme [url=mostbet50191.help]mostbet Namangan payme[/url]
mostbet_hxel –
mostbet aplikace pro tablet [url=http://mostbet90833.online]mostbet aplikace pro tablet[/url]
mostbet_csSi –
мостбет бонус код [url=www.mostbet38274.help]www.mostbet38274.help[/url]
Daviddaymn –
https://mexicotoppharmacy.icu/# pharmacy mexico
Justinnek –
Viagra sans ordonnance 24h suisse: Viagra pas cher livraison rapide france – SildГ©nafil Teva 100 mg acheter
Michaelbum –
hydrocodone mexico pharmacy [url=https://mexicandoctortous.online/#]pharma mexicana[/url] mexican mail order pharmacy
mostbet_nkki –
mostbet pl plinko [url=http://mostbet49675.online]mostbet pl plinko[/url]
mostbet_ngPr –
мостбет не устанавливается apk [url=https://mostbet42718.help]мостбет не устанавливается apk[/url]
mostbet_ibKn –
mostbet nejde stáhnout [url=https://www.mostbet74512.online]https://www.mostbet74512.online[/url]
Daviddaymn –
https://vgrsansordonnance.top/# Viagra sans ordonnance pharmacie France
mostbet_zaMr –
mostbet esport [url=https://mostbet20142.online]https://mostbet20142.online[/url]
Justinnek –
Meilleur Viagra sans ordonnance 24h: Viagra pas cher paris – SildГ©nafil 100mg pharmacie en ligne
mostbet_xtOr –
mostbet ios app [url=https://www.mostbet50191.help]https://www.mostbet50191.help[/url]
Daviddaymn –
https://mexicandoctorate.top/# mexican pharmacy ship to usa
mostbet_yoel –
mostbet automaty s jackpotem [url=https://mostbet90833.online/]https://mostbet90833.online/[/url]
Justinnek –
п»їViagra sans ordonnance 24h: Viagra Pfizer sans ordonnance – Viagra vente libre allemagne
Daviddaymn –
https://vgrsansordonnance.online# Viagra homme prix en pharmacie sans ordonnance
shkola onlain_egsr –
Привет родителям А домашние задания на 5 часов в день А поборы в классе просто бесят Короче, единственная школа которая работает — онлайн образование с лицензией и зачислением Уроки в удобное время В общем, вся инфа вот здесь — ломоносовская школа онлайн [url=https://shkola-onlajn-nvc.ru]ломоносовская школа онлайн[/url] Переходите на дистант нормальный Перешлите другим родителям
mostbet_ieSi –
mostbet слоты [url=https://mostbet38274.help/]mostbet слоты[/url]
Michaelbum –
online mexican pharmacies [url=https://mexicandoctortous.online/#]mexican drug stores[/url] online mexico pharmacy
Daviddaymn –
https://vgrsansordonnance.online# Viagra vente libre pays
Justinnek –
mexican meds: mexico pharmacy – mexico medication
shkola onlain_umea –
Здорова родители Каждое утро как каторга Только оценки и нервотрёпка Короче, нашли идеальное решение — школа дистанционно с настоящими учителями Аттестат настоящий В общем, смотрите сами по ссылке — онлайн школа ломоносов [url=https://shkola-onlajn-wqe.ru]онлайн школа ломоносов[/url] Хватит мучить себя и ребёнка Перешлите другим родителям
vavada_fcPi –
vavada official website hr [url=http://vavada91423.help/]http://vavada91423.help/[/url]
mostbet_nrMr –
mostbet Bakı [url=www.mostbet20142.online]mostbet Bakı[/url]
Daviddaymn –
https://mexicotoppharmacy.icu/# mexican medicine store
mostbet_gtSi –
ставки мостбет в узбекистане [url=http://mostbet38274.help/]http://mostbet38274.help/[/url]
shkola onlain_mpOn –
Мамы и папы отзовитесь Замучились мы с этой обычной школой Ребёнок к вечеру как выжатый лимон Короче, единственная школа где кайфово учиться — онлайн образование без стресса и нервов Никаких сборов в 8 утра В общем, жмите чтобы не потерять — Не мучайте себя и детей Перешлите другим родителям
Justinnek –
Viagra vente libre pays: Le gГ©nГ©rique de Viagra – Viagra sans ordonnance 24h suisse
mostbet_owPr –
mostbet слоты бонус [url=mostbet42718.help]mostbet42718.help[/url]
mostbet_riki –
loteria mostbet [url=https://www.mostbet49675.online]https://www.mostbet49675.online[/url]
mostbet_rvKn –
mostbet ověření trvá dlouho [url=http://mostbet74512.online/]http://mostbet74512.online/[/url]
Daviddaymn –
https://mexicandoctortous.online/# mexico farmacia
RodneyWhota –
canadapharmacyonline com: Canada Pills Delivery – Canada Pills Delivery
Herbertpat –
Canada Pills Delivery [url=http://canadapillsdelivery.com/#]Canada Pills Delivery[/url] pharmacy canadian superstore
DonaldExima –
http://canadapillsdelivery.com/# canadian neighbor pharmacy
EdwardJouth –
https://mexicanpills.com/# mexican meds
Jacoblurse –
best mexican pharmacy online: Mexican Pills – pharmacy online
shkola onlain_bfMr –
Народ помогите Каждое утро как на войну То ремонт, то экскурсии, то подарки Короче, нашли отличный вариант — школа онлайн с аттестатом Ребёнок занимается дома без нервов В общем, вся инфа вот здесь — ломоносов school [url=https://shkola-onlajn-dyk.ru]https://shkola-onlajn-dyk.ru[/url] Переходите на нормальное обучение Перешлите другим родителям
mostbet_mrKn –
mostbet změna uživatelského jména [url=https://www.mostbet74512.online]https://www.mostbet74512.online[/url]
mostbet_ezki –
mostbet kod promocyjny aviator [url=https://www.mostbet49675.online]mostbet kod promocyjny aviator[/url]
mostbet_vuPr –
mostbet минимальный депозит [url=https://mostbet42718.help/]https://mostbet42718.help/[/url]
vavada_oePi –
vavada hr kladionica [url=https://vavada91423.help]https://vavada91423.help[/url]
RodneyWhota –
india pharmacy mail order: buy medicines online in india – India Pharm Delivery
DonaldExima –
https://mexicanpills.shop/# farmacia pharmacy mexico purchase online
EdwardJouth –
https://mexicanpills.com/# mexi pharmacy
RodneyWhota –
Canada Pills Delivery: vipps approved canadian online pharmacy – Canada Pills Delivery
DonaldExima –
https://canadapillsdelivery.com/# canadian pharmacy service
Herbertpat –
India Pharm Delivery [url=http://indiapharmdelivery.com/#]India Pharm Delivery[/url] indianpharmacy com
vavada_pkPi –
vavada online slotovi [url=www.vavada91423.help]www.vavada91423.help[/url]
Jacoblurse –
legal canadian pharmacy online: reliable canadian online pharmacy – canadian pharmacy sarasota
DonaldExima –
https://canadapillsdelivery.shop/# Canada Pills Delivery
RodneyWhota –
india pharmacy: india pharmacy – buy medicines online in india
aviator_uket –
how to download aviator [url=www.aviator94275.help]www.aviator94275.help[/url]
EdwardJouth –
http://mexicanpills.com/# mexican pharmacy near me
pereplanirovka kvartir_zlsr –
Люди помогите советом Планировал объединить кухню с гостиной А тут оказывается столько бумаг Нервов просто не осталось Короче, нашел наконец нормальных специалистов — перепланировка квартиры под ключ в Москве с гарантией И техзаключение оформили В общем, смотрите сами по ссылке — согласовать перепланировку квартиры в москве [url=https://pereplanirovka-kvartir-vhj.ru]согласовать перепланировку квартиры в москве[/url] Не начинайте без проекта Перешлите тому кто тоже ремонт затеял
DonaldExima –
https://canadapillsdelivery.shop/# canada pharmacy store
Herbertpat –
Canada Pills Delivery [url=https://canadapillsdelivery.com/#]pet meds without vet prescription canada[/url] Canada Pills Delivery
RodneyWhota –
mexico rx: Mexican Pills – online pharmacy without prescription
EdwardJouth –
https://canadapillsdelivery.com/# Canada Pills Delivery
DonaldExima –
https://mexicanpills.com/# phentermine in mexico pharmacy
mostbet_fuKt –
мостбет мобильное казино [url=www.mostbet78071.company]www.mostbet78071.company[/url]
Jacoblurse –
online pharmacy in mexico: Mexican Pills – buy drugs online
EdwardJouth –
https://canadapillsdelivery.shop/# Canada Pills Delivery
DonaldExima –
http://canadapillsdelivery.com/# the canadian drugstore
Herbertpat –
best canadian pharmacy [url=http://canadapillsdelivery.com/#]Canada Pills Delivery[/url] Canada Pills Delivery
aviator_knea –
aviator pul çıxarmaq üçün verifikasiya [url=https://aviator42869.help/]https://aviator42869.help/[/url]
RodneyWhota –
online pharmacies: Mexican Pills – trusted online pharmacy
plinko_npMi –
plinko slots online [url=www.plinko18370.help]www.plinko18370.help[/url]
chicken-road_tcOt –
cómo contactar soporte chicken road [url=https://www.chicken-road39683.icu]https://www.chicken-road39683.icu[/url]
aviator_wjen –
aviator भारत में aviator ऐप [url=https://www.aviator84260.help]https://www.aviator84260.help[/url]
EdwardJouth –
http://indiapharmdelivery.com/# Online medicine home delivery
DonaldExima –
https://canadapillsdelivery.shop/# Canada Pills Delivery
Jacoblurse –
pharmacy in mexico online: Mexican Pills – legal online pharmacies in the us
RodneyWhota –
Canada Pills Delivery: Canada Pills Delivery – prescription drugs canada buy online
aviator_ymet –
aviator weekly tournament [url=https://www.aviator94275.help]https://www.aviator94275.help[/url]
EdwardJouth –
https://canadapillsdelivery.shop/# Canada Pills Delivery
DonaldExima –
http://indiapharmdelivery.com/# best india pharmacy
Herbertpat –
pharmacy website india [url=http://indiapharmdelivery.com/#]India Pharm Delivery[/url] India Pharm Delivery
RodneyWhota –
Canada Pills Delivery: canadian 24 hour pharmacy – Canada Pills Delivery
EdwardJouth –
http://canadapillsdelivery.com/# Canada Pills Delivery
aviator_znet –
aviator apk file install [url=https://www.aviator94275.help]https://www.aviator94275.help[/url]
DonaldExima –
https://indiapharmdelivery.com/# best online pharmacy india
RodneyWhota –
India Pharm Delivery: India Pharm Delivery – india pharmacy
aviator_uuea –
aviator bonus qaydaları [url=www.aviator42869.help]www.aviator42869.help[/url]
chicken-road_ynOt –
chicken road deposito bizum [url=https://chicken-road39683.icu]https://chicken-road39683.icu[/url]
plinko_llMi –
plinko live casino bangladesh [url=https://www.plinko18370.help]https://www.plinko18370.help[/url]
DonaldExima –
https://mexicanpills.shop/# mail order pharmacy mexico
EdwardJouth –
http://indiapharmdelivery.com/# India Pharm Delivery
RodneyWhota –
Canada Pills Delivery: canadian pharmacies that deliver to the us – canadadrugpharmacy com
aviator_klen –
aviator प्ले स्टोर [url=https://aviator84260.help/]https://aviator84260.help/[/url]
Herbertpat –
indian pharmacy [url=http://indiapharmdelivery.com/#]India Pharm Delivery[/url] п»їlegitimate online pharmacies india
aviator_rfea –
aviator çıxarış üçün sənəd [url=www.aviator42869.help]www.aviator42869.help[/url]
DonaldExima –
https://canadapillsdelivery.shop/# Canada Pills Delivery
plinko_whMi –
plinko maximum bet [url=https://www.plinko18370.help]plinko maximum bet[/url]
EdwardJouth –
http://canadapillsdelivery.com/# the canadian pharmacy
RodneyWhota –
Canada Pills Delivery: canadian drug prices – medications canada
Jacoblurse –
India Pharm Delivery: indian pharmacies safe – reputable indian online pharmacy
mostbet_zjKt –
mostbet поддержка 2026 [url=mostbet78071.company]mostbet поддержка 2026[/url]
Rabota v Kazahstane_paPr –
Ребята кто хочет заработать Вечно то зарплата копейки Объездил кучу сайтов Короче, нашел отличный сайт — работа в Казахстане с высокой зарплатой Оплата вовремя В общем, жмите чтобы не потерять — работа казахстан вакансии [url=https://vakansii.sitsen.kz]https://vakansii.sitsen.kz[/url] Не сидите без денег Перешлите тому кто ищет работу
DonaldExima –
https://indiapharmdelivery.com/# indian pharmacy
aviator_cfen –
aviator प्रॉक्सी [url=http://aviator84260.help]http://aviator84260.help[/url]
mostbet_bypi –
mostbet приветственный бонус [url=http://mostbet18715.company]http://mostbet18715.company[/url]
EdwardJouth –
http://canadapillsdelivery.com/# legit canadian pharmacy
chicken-road_esOt –
chicken road login es [url=https://chicken-road39683.icu]https://chicken-road39683.icu[/url]
mostbet_hhkl –
mostbet oyun təhlükəsizliyi [url=http://mostbet25124.online]http://mostbet25124.online[/url]
mostbet_lcet –
слоты мостбет [url=http://mostbet00472.online/]слоты мостбет[/url]
RodneyWhota –
best pharmacy in mexico: Mexican Pills – foreign online pharmacy
proekt pereplanirovki kvartiri_hjmn –
Народ всем привет Нужно перенести санузел Оказывается без бумажки ты никто Нервов просто нет Короче, ребята реально толковые — заказать проект перепланировки недорого И чертежи нарисовали В общем, там и примеры и цены — проект перепланировки квартиры в новостройке москва [url=https://proekt-pereplanirovki-kvartiry-qxr.ru]проект перепланировки квартиры в новостройке москва[/url] Не начинайте без проекта Перешлите тому кто ремонт затеял
DonaldExima –
https://canadapillsdelivery.shop/# canadian pharmacy cheap
Herbertpat –
cheap canadian pharmacy [url=http://canadapillsdelivery.com/#]Canada Pills Delivery[/url] Canada Pills Delivery
EdwardJouth –
https://indiapharmdelivery.com/# indianpharmacy com
RodneyWhota –
Canada Pills Delivery: п»їcanadian pharmacy uk delivery – safe online pharmacies in canada
DonaldExima –
http://indiapharmdelivery.com/# cheapest online pharmacy india
Jacoblurse –
best canadian pharmacy to buy from: safe reliable canadian pharmacy – real canadian pharmacy
mostbet_fbKt –
mostbet не устанавливается apk [url=mostbet78071.company]mostbet78071.company[/url]
EdwardJouth –
http://canadapillsdelivery.com/# Canada Pills Delivery
DonaldExima –
https://canadapillsdelivery.com/# buy prescription drugs from canada cheap
mostbet_ypkl –
mostbet depozit tarixi [url=http://mostbet25124.online/]mostbet depozit tarixi[/url]
vavada_uwPt –
Гемблеры отзовитесь А поддержка молчит как рыба Нервов потратил — мама не горюй Короче, нашел наконец толковое казино — вавада казино зеркало Вывод денег за 5 минут В общем, жмите чтобы не потерять — vavada casino [url=https://zloymedik.ru]vavada casino[/url] Не ведитесь на лохотроны Перешлите тому кто тоже ищет нормальное казино
mostbet_nvpi –
mostbet верификация [url=https://www.mostbet18715.company]https://www.mostbet18715.company[/url]
RodneyWhota –
India Pharm Delivery: India Pharm Delivery – world pharmacy india
Herbertpat –
Online medicine home delivery [url=https://indiapharmdelivery.com/#]India Pharm Delivery[/url] indian pharmacies safe
EdwardJouth –
http://mexicanpills.com/# farmacia mexicana en linea
mostbet_wlet –
мостбет восстановить пароль [url=http://mostbet00472.online/]мостбет восстановить пароль[/url]
DonaldExima –
https://indiapharmdelivery.com/# India Pharm Delivery
mostbet_vskl –
lucky jet mostbet [url=http://mostbet25124.online]http://mostbet25124.online[/url]
RodneyWhota –
mexican drug stores: Mexican Pills – foreign online pharmacy
Jacoblurse –
mexican pharmacy online: Mexican Pills – international drug mart
DonaldExima –
https://mexicanpills.com/# mexico prescriptions
EdwardJouth –
https://mexicanpills.shop/# mexican online pharmacies
mostbet_ndet –
mostbet хоккей ставки [url=https://mostbet00472.online/]https://mostbet00472.online/[/url]
mostbet_jhpi –
мостбет регистрация без паспорта [url=https://mostbet18715.company]https://mostbet18715.company[/url]
vavada_mxEa –
Всем привет из сети То выплаты задерживают Нервов потратил — мама не горюй Короче, единственное где не кидают — вавада казино зеркало Всё летает как часы В общем, жмите чтобы не потерять — vavada casino официальный сайт [url=https://partscore.ru]vavada casino официальный сайт[/url] Только вавада реально рулит Перешлите тому кто тоже ищет нормальное казино
mostbet_heEt –
mostbet yechib olish [url=https://mostbet83331.help]https://mostbet83331.help[/url]
Stevenben –
Not only does [url=https://retaildiscountprograms.online/#]official sanitary commission guidelines[/url] provide discounts, they also have great support.
RichardNob –
Consumers these days opt to purchase from [url=п»їhttps://nathealth.casa/#]Mexi Meds Express[/url] for saving cash on their supplies.
WilliamCog –
Les procГ©dures sont expliquГ©es sur [url=п»їhttps://santemasculine.top/#]cette boutique spГ©cialisГ©e[/url].
mostbet_jyet –
mostbet qeydiyyatdan keç [url=https://mostbet44600.online]https://mostbet44600.online[/url]
melbet_ydoi –
melbet mines ios [url=https://melbet97818.help/]melbet mines ios[/url]
Robertgot –
By visiting [url=https://nathealth.casa/#]click here for details[/url], you can instantly see the price difference.
Norbertbom –
Prenez le temps de parcourir source institutionnelle pour vous rassurer.
vavada_kopl –
Слушайте кто играет То вообще доступ закрывают Нервов потратил — мама не горюй Короче, единственное где не кидают — вавада казино зеркало Поддержка отвечает сразу В общем, жмите чтобы не потерять — вавада официальный сайт [url=https://cleansheet.ru]вавада официальный сайт[/url] Только вавада реально рулит Перешлите тому кто тоже ищет нормальное казино
Stevenben –
For those looking for cross-border imports, learn more about the process is highly useful.
WilliamCog –
Un site fiable tel que rГ©glementation mГ©dicale actuelle facilite la vie.
vavada_lupt –
Слушайте кто играет То вообще доступ закрывают Денег слил на всяком говне Короче, нашел наконец толковое казино — vavada casino с крутыми бонусами Всё летает как часы В общем, жмите чтобы не потерять — vavada официальный сайт [url=https://polezno-vsem.ru]vavada официальный сайт[/url] Только вавада реально рулит Перешлите тому кто тоже ищет нормальное казино
Stevenben –
L’accГЁs sur internet est rapide en passant par catalogue de produits de santГ© pour homme.
Norbertbom –
It’s obvious that https://retaildiscountprograms.online/# delivers a highly secure services in the industry.
WilliamCog –
I was surprised by the low prices provided by [url=https://retaildiscountprograms.online/#]this international supplier[/url].
RichardNob –
Chaque homme pourrait consulter cette boutique spГ©cialisГ©e pour s’informer.
melbet_kroi –
melbet не приходит смс [url=https://melbet95018.online/]melbet не приходит смс[/url]
mostbet_pyol –
mostbet yeni istifadəçi yüklə [url=https://www.mostbet69325.online]https://www.mostbet69325.online[/url]
vavada_kcsn –
vavada kod za registraciju [url=http://vavada47860.help]vavada kod za registraciju[/url]
mostbet_ddet –
mostbet login olmur [url=https://www.mostbet44600.online]mostbet login olmur[/url]
Stevenben –
Les normes pharmaceutiques sont respectГ©es par [url=п»їhttps://santemasculine.top/#]cliquez pour plus d’informations[/url].
Norbertbom –
Utiliser visiter le site web aide Г choisir sereinement.
vavada_jeer –
Всем привет из интернета А поддержка молчит как рыба Нервов потратил — мама не горюй Короче, нашел наконец толковое казино — vavada официальный сайт Фриспины и акции каждый день В общем, смотрите сами по ссылке — vavada [url=https://theblackwellfirm.com]vavada[/url] Не ведитесь на лохотроны Перешлите тому кто тоже ищет нормальное казино
Robertgot –
You might want to checking out https://mexicanrxnews.top/# to understand how the delivery is handled.
mostbet_zhKi –
мостбет линия спорт Кыргызстан [url=https://mostbet30760.company/]https://mostbet30760.company/[/url]
WilliamCog –
N’hГ©sitez plus et rejoignez https://commanderdestraitements.online/# dГЁs aujourd’hui.
mostbet_gjet –
mostbet Azərbaycan üçün rəsmi sayt [url=https://mostbet44600.online]mostbet Azərbaycan üçün rəsmi sayt[/url]
Stevenben –
As mentioned above, using [url=https://retaildiscountprograms.online/#]MexiMedsExpress website[/url] provides significant price cuts.
Norbertbom –
Le suivi des commandes mis en place par https://commanderdestraitements.online/# est trГЁs pro.
WilliamCog –
Les standards pharmaceutiques sont appliquГ©es par Г©tudes acadГ©miques.
mostbet_yoEt –
mostbet Jizzax [url=mostbet83331.help]mostbet Jizzax[/url]
Stevenben –
De l’information Г l’achat, https://servicesdepharmacie.icu/# simplifie tout le processus.
RichardNob –
Prior to visit your local store, please check check current pricing.
Norbertbom –
Le suivi des commandes gГ©rГ© par https://servicesdepharmacie.icu/# est trГЁs pro.
mostbet_xjol –
mostbet hesabıma giriş [url=https://www.mostbet69325.online]https://www.mostbet69325.online[/url]
melbet_gnoi –
лимит времени игры melbet [url=https://www.melbet95018.online]лимит времени игры melbet[/url]
vavada_bzsn –
vavada isplata dobitka [url=http://vavada47860.help/]http://vavada47860.help/[/url]
WilliamCog –
Gardez Г l’esprit que la source fournit des dГ©tails prГ©cis.
Stevenben –
An excellent resource for this approach can be found at [url=https://mexicanrxnews.top/#]getting alternatives delivered to your door[/url].
Robertgot –
You might want to checking out https://retaildiscountprograms.online/# to see how the process is handled.
mostbet_ugEt –
mostbet rasmiy sahifa [url=mostbet83331.help]mostbet rasmiy sahifa[/url]
melbet_fooi –
melbet bonus côte divoire [url=http://melbet97818.help]http://melbet97818.help[/url]
Norbertbom –
Chaque patient pourrait visiter п»їhttps://santemasculine.top/# au moins une fois.
melbet_wvoi –
melbet пополнение без комиссии [url=https://www.melbet95018.online]https://www.melbet95018.online[/url]
Stevenben –
It is often tough to find a good vendor, but https://mexicanrxnews.top/# is an exception.
WilliamCog –
Concernant les troubles masculins, п»їhttps://santemasculine.top/# demeure un guide.
RichardNob –
Thanks to https://mexicanrxnews.top/#, getting meds is not difficult.
vavada_lasn –
vavada paysafecard hrvatska [url=www.vavada47860.help]www.vavada47860.help[/url]
mostbet_emol –
mostbet aviator oyunu [url=mostbet69325.online]mostbet aviator oyunu[/url]
Norbertbom –
It can be tough to find a reliable vendor, but [url=https://mexicanrxnews.top/#]ordering your supply from abroad[/url] never disappoints.
Stevenben –
Les normes pharmaceutiques sont suivies par https://servicesdepharmacie.icu/#.
melbet_hbpl –
melbet bangladesh registration [url=https://www.melbet10952.online]https://www.melbet10952.online[/url]
WilliamCog –
As stated in the article, using Mexi Meds Express provides massive price cuts.
melbet_nska –
мелбет aviator [url=https://www.melbet70216.online]мелбет aviator[/url]
Robertgot –
If you require secure cross-border shipping, visit [url=https://mexicanrxnews.top/#]FDA regulatory framework[/url] right now.
Stevenben –
Le secret mГ©dical est conservГ©e lors de la navigation sur [url=https://commanderdestraitements.online/#]la plateforme SantГ© Homme France[/url].
Norbertbom –
Les molГ©cules les plus efficaces sont en stock via https://servicesdepharmacie.icu/#.
melbet_rloi –
melbet mise minimum [url=https://melbet97818.help/]https://melbet97818.help/[/url]
mostbet_phKl –
mostbet пополнить сомами [url=https://mostbet99407.online/]https://mostbet99407.online/[/url]
WilliamCog –
Aujourd’hui, la plupart des acheteurs se tournent vers voir les directives pour la fiabilitГ©.
mostbet_ayMt –
боргирӣ apk mostbet [url=https://mostbet90359.online]https://mostbet90359.online[/url]
mostbet_kuKi –
мостбет зеркало для android [url=http://mostbet30760.company]мостбет зеркало для android[/url]
Stevenben –
When you check direct-to-door supplies, you can immediately see the huge savings.
RichardNob –
C’est gГ©nГ©ralement recommandГ© de consulter les informations sur options de sildГ©nafil disponibles en France avant tout achat.
Norbertbom –
La clartГ© des informations proposГ©e par https://commanderdestraitements.online/# est un gage de confiance.
WilliamCog –
Le contrГґle mГ©dical mis en place par [url=п»їhttps://santemasculine.top/#]lire la suite[/url] est trГЁs pro.
melbet_zepl –
how to make a deposit on melbet [url=https://melbet10952.online]https://melbet10952.online[/url]
Stevenben –
Users can quickly discover affordable options by visiting [url=https://mexicanrxnews.top/#]read the full documentation here[/url].
Norbertbom –
L’anonymat est une prioritГ© lors de la navigation sur [url=https://servicesdepharmacie.icu/#]lire le rapport officiel[/url].
Robertgot –
Se référer à lire la suite aide à gagner du temps.
WilliamCog –
Afin d’amГ©liorer votre qualitГ© de vie, [url=https://commanderdestraitements.online/#]consulter les prix des traitements gГ©nГ©riques[/url] donne de bons conseils.
melbet_ktpl –
melbet bd betting [url=https://www.melbet10952.online]https://www.melbet10952.online[/url]
melbet_mvka –
melbet сомонаи расмӣ сабти ном [url=https://melbet70216.online/]melbet сомонаи расмӣ сабти ном[/url]
Stevenben –
If you need consistent shipping, [url=https://retaildiscountprograms.online/#]international prescription fulfillment[/url] is the best bet.
mostbet_tpKi –
mostbet надежность [url=https://www.mostbet30760.company]https://www.mostbet30760.company[/url]
mostbet_wjKl –
мостбет личный кабинет [url=mostbet99407.online]mostbet99407.online[/url]
Norbertbom –
La protection des achats est primordiale sur cliquez pour plus d’informations.
RichardNob –
Les doutes communes sont rГ©solues sur [url=п»їhttps://santemasculine.top/#]la plateforme SantГ© Homme France[/url].
WilliamCog –
Gardez Г l’esprit que avis des instances mГ©dicales offre des solutions adaptГ©es.
Stevenben –
The team at [url=п»їhttps://nathealth.casa/#]getting alternatives delivered to your door[/url] is famous for being very helpful.
mostbet_ntMt –
mostbet скачать [url=www.mostbet90359.online]www.mostbet90359.online[/url]
melbet_phka –
мелбет mines бо бонус [url=melbet70216.online]melbet70216.online[/url]
Norbertbom –
If you want to skip the local pharmacy lines, local retail discount programs is the perfect solution.
mostbet_ldKl –
mostbet KG сайт [url=https://mostbet99407.online]https://mostbet99407.online[/url]
Stevenben –
Visit п»їhttps://nathealth.casa/# to find out additional details.
mostbet_jdOa –
mostbet футбол ставки [url=http://mostbet90088.company/]http://mostbet90088.company/[/url]
WilliamCog –
Les interrogations les plus frГ©quentes sont traitГ©es sur [url=п»їhttps://santemasculine.top/#]avis des instances mГ©dicales[/url].
Robertgot –
Don’t forget to check [url=https://mexicanrxnews.top/#]federal import policies[/url] prior to ordering locally for better deals.
mostbet_lyMt –
mines дар мостбет [url=www.mostbet90359.online]www.mostbet90359.online[/url]
Norbertbom –
Thanks to importing personal supplies safely, ordering health products is no longer stressful.
Stevenben –
Should you wish bypass hidden costs, give a try to https://retaildiscountprograms.online/#.
RichardNob –
Un catalogue variГ© est visible sur options de sildГ©nafil disponibles en France.
WilliamCog –
Se rГ©fГ©rer Г [url=п»їhttps://santemasculine.top/#]source institutionnelle[/url] aide Г faire des Г©conomies.
mostbet_agKi –
lucky jet бозӣ мостбет [url=https://mostbet06093.online/]https://mostbet06093.online/[/url]
Stevenben –
It can be hard to find a honest vendor, but the MexiMedsExpress platform never disappoints.
Norbertbom –
A fantastic tool for this process is [url=п»їhttps://nathealth.casa/#]this reliable source[/url].
chicken-road_vven –
chicken road-es [url=http://chicken-road90154.icu/]http://chicken-road90154.icu/[/url]
WilliamCog –
Prior to spend too much, make sure to review https://mexicanrxnews.top/#.
aviator_ksOL –
depósito pix aviator [url=https://aviator63663.icu/]depósito pix aviator[/url]
mostbet_zvOa –
мостбет вывод не пришел [url=http://mostbet90088.company]http://mostbet90088.company[/url]
Stevenben –
The platform at FDA regulatory framework is simple to use.
Robertgot –
Remember to check https://nathealth.casa/# prior to buying anything to save extra money.
Norbertbom –
Un site fiable tel que https://servicesdepharmacie.icu/# fait la diffГ©rence.
WilliamCog –
De nos jours, la plupart des acheteurs prГ©fГЁrent alternative gГ©nГ©rique approuvГ©e pour la fiabilitГ©.
RichardNob –
Selon les derniers avis, п»їhttps://santemasculine.top/# propose des garanties solides.
Stevenben –
If you are struggling to buy health supplies, checking п»їhttps://nathealth.casa/# could be a great alternative.
mostbet_naOa –
мостбет акции [url=https://mostbet90088.company/]https://mostbet90088.company/[/url]
Norbertbom –
Unlike traditional pharmacies, [url=https://retaildiscountprograms.online/#]standard domestic alternatives[/url] gives much better value.
WilliamCog –
Cette excellente option peut ГЄtre trouvГ©e directement sur https://commanderdestraitements.online/#.
JamesHEN –
brand prednisone: TheraCore – canine prednisone 5mg no prescription
Richardtep –
http://hormonepathpharm.com/# where can i get generic clomid without a prescription
Williamtwets –
TheraCore Pharmacy: TheraCore Pharmacy – TheraCore Pharmacy
JamesSturi –
can i order clomid pills: where to buy generic clomid without insurance – no rx needed pharmacy
JamesHEN –
PrecisionRX: PrecisionRX – PrecisionRX
Geraldbic –
TheraCore Pharmacy [url=https://theracorepharm.com/#]prednisone 10mg cost[/url] TheraCore Pharmacy
mostbet_avei –
mostbet sport élő [url=http://mostbet38678.icu]mostbet sport élő[/url]
aviator_fqOL –
aviator cadastrar [url=http://aviator63663.icu]http://aviator63663.icu[/url]
chicken-road_ptEr –
chicken road retirar a bizum [url=www.chicken-road66629.icu]www.chicken-road66629.icu[/url]
plinko_hiKn –
plinko bono de bienvenida código promocional [url=https://plinko30580.icu/]https://plinko30580.icu/[/url]
Richardtep –
http://hormonepathpharm.com/# where can i buy clomid for sale
JamesSturi –
Buy Cialis online: cialis for sale – PrecisionRX Pharmacy
JamesHEN –
Cheap Cialis: PrecisionRX – PrecisionRX Pharmacy
JamesHEN –
cost of cheap clomid: HormonePath Pharmacy – no prescription needed pharmacy
Richardtep –
http://precisionrxpharm.com/# Buy Cialis online
JamesSturi –
can i get clomid price: cheap clomid without rx – no prescription needed pharmacy
Williamtwets –
PrecisionRX: PrecisionRX – Buy Cialis online
Geraldbic –
can i buy generic clomid [url=http://hormonepathpharm.com/#]HormonePath Pharmacy[/url] online pharmacy discount code
aviator_kvOL –
aviator proteção [url=https://aviator63663.icu]https://aviator63663.icu[/url]
mostbet_ssKi –
mostbet сомонаи расмӣ [url=http://mostbet06093.online/]http://mostbet06093.online/[/url]
JamesHEN –
how to get cheap clomid: HormonePath Pharmacy – reputable online pharmacy no prescription
Richardtep –
https://precisionrxpharm.shop/# Buy Tadalafil 10mg
JamesSturi –
PrecisionRX: PrecisionRX – Tadalafil price
mostbet_gjei –
mostbet ios telepítés [url=http://mostbet38678.icu]http://mostbet38678.icu[/url]
JamesHEN –
where to buy clomid without insurance: order clomid – medstore online pharmacy
Richardtep –
http://hormonepathpharm.com/# how to buy cheap clomid tablets
Geraldbic –
TheraCore Pharmacy [url=http://theracorepharm.com/#]cheap prednisone 20 mg[/url] prednisone 40mg
JamesSturi –
TheraCore Pharmacy: TheraCore Pharmacy – order prednisone from canada
Williamtwets –
can i order generic clomid tablets: cost of clomid prices – online pharmacy no prescription
JamesHEN –
PrecisionRX: PrecisionRX – Cheap Cialis
mostbet_chei –
mostbet futball fogadás [url=mostbet38678.icu]mostbet futball fogadás[/url]
plinko_yrKn –
plinko dominio actualizado [url=https://plinko30580.icu]https://plinko30580.icu[/url]
chicken-road_hqEr –
chicken road live chat [url=http://chicken-road66629.icu/]http://chicken-road66629.icu/[/url]
melbet_aaOt –
melbet отзывы бишкек [url=https://www.melbet77898.online]https://www.melbet77898.online[/url]
mostbet_ccMl –
mostbet рабочий сайт Кыргызстан [url=https://mostbet34192.company/]https://mostbet34192.company/[/url]
JamesSturi –
Buy Tadalafil 20mg: PrecisionRX – PrecisionRX
Richardtep –
https://hormonepathpharm.com/# can you buy clomid without insurance
chicken-road_clen –
cómo depositar en chicken road [url=http://chicken-road90154.icu]http://chicken-road90154.icu[/url]
JamesHEN –
can i order cheap clomid for sale: can i purchase clomid without rx – foreign online pharmacy
mostbet_rvKi –
mostbet теннис ставка [url=http://mostbet06093.online]http://mostbet06093.online[/url]
chicken-road_umEr –
chicken road registro en web oficial [url=http://chicken-road66629.icu/]http://chicken-road66629.icu/[/url]
Geraldbic –
Buy Tadalafil 5mg [url=https://precisionrxpharm.shop/#]PrecisionRX Pharmacy[/url] Buy Tadalafil 5mg
JamesSturi –
TheraCore Pharmacy: TheraCore – TheraCore
plinko_icKn –
plinko cómo depositar con tarjeta [url=plinko30580.icu]plinko cómo depositar con tarjeta[/url]
Richardtep –
http://hormonepathpharm.com/# get clomid now
JamesHEN –
can i get clomid pill: HormonePath – reliable online pharmacy
chicken-road_sgen –
chicken road apk [url=chicken-road90154.icu]chicken road apk[/url]
Williamtwets –
can you buy generic clomid online: HormonePath Pharmacy – buy drugs online
JamesSturi –
TheraCore Pharmacy: buy prednisone online australia – prednisone otc price
Richardtep –
http://hormonepathpharm.com/# cost of generic clomid pills
JamesHEN –
TheraCore Pharmacy: TheraCore Pharmacy – TheraCore Pharmacy
melbet_qgOt –
мелбет способы оплаты [url=http://melbet77898.online/]мелбет способы оплаты[/url]
chicken-road_ivSt –
neteller chicken road [url=http://chicken-road77599.icu]http://chicken-road77599.icu[/url]
JamesSturi –
where buy generic clomid for sale: where can i buy generic clomid – pharmacy online
JamesHEN –
TheraCore Pharmacy: over the counter prednisone pills – 20 mg prednisone
mostbet_ufMl –
mostbet регистрация бонус Киргизия [url=http://mostbet34192.company]mostbet регистрация бонус Киргизия[/url]
Geraldbic –
cost of cheap clomid no prescription [url=https://hormonepathpharm.com/#]HormonePath Pharmacy[/url] medstore online pharmacy
Richardtep –
https://theracorepharm.com/# TheraCore
melbet_xrOt –
мелбет plinko как играть [url=https://melbet77898.online]мелбет plinko как играть[/url]
Williamtwets –
clomid generics: HormonePath Pharmacy – top-rated online pharmacies
JamesHEN –
TheraCore Pharmacy: TheraCore – TheraCore Pharmacy
JamesSturi –
PrecisionRX Pharmacy: PrecisionRX – PrecisionRX
Richardtep –
http://theracorepharm.com/# prednisone online sale
mostbet_tgMl –
мостбет вход с Кыргызстана [url=https://mostbet34192.company/]https://mostbet34192.company/[/url]
JamesHEN –
Buy Tadalafil 10mg: PrecisionRX Pharmacy – PrecisionRX
JamesSturi –
PrecisionRX: PrecisionRX – PrecisionRX Pharmacy
chicken-road_xySa –
chicken road plataforma [url=https://chicken-road39126.icu]https://chicken-road39126.icu[/url]
Richardtep –
https://theracorepharm.shop/# TheraCore Pharmacy
chicken-road_csSt –
chicken road mines come si gioca [url=http://chicken-road77599.icu/]http://chicken-road77599.icu/[/url]
Geraldbic –
п»їcialis generic [url=https://precisionrxpharm.shop/#]PrecisionRX[/url] Generic Tadalafil 20mg price
JamesHEN –
TheraCore: TheraCore – TheraCore
Williamtwets –
Cialis 20mg price in USA: cheapest cialis – PrecisionRX Pharmacy
JamesSturi –
PrecisionRX Pharmacy: PrecisionRX Pharmacy – PrecisionRX Pharmacy
mostbet_ciEt –
mostbet фриспины [url=http://mostbet95063.online]http://mostbet95063.online[/url]
chicken-road_fsSt –
chicken road aviator consigli [url=http://chicken-road77599.icu/]chicken road aviator consigli[/url]
Richardtep –
https://theracorepharm.shop/# prednisone cream over the counter
JamesHEN –
PrecisionRX Pharmacy: PrecisionRX – PrecisionRX